 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 10, No. 2, July 2003, pp. 31-39 REVIEW OF GLOBAL MENACE OF ROAD ACCIDENTS WITH SPECIAL REFERENCE TO MALAYSIA- A SOCIAL PERSPECTIVE Abdul Kareem Department of Radiology, School of Medical Sciences,
Universiti Sains Malaysia, Health Campus, 16150 Kubang Kerian, Kelantan,
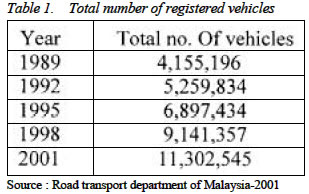
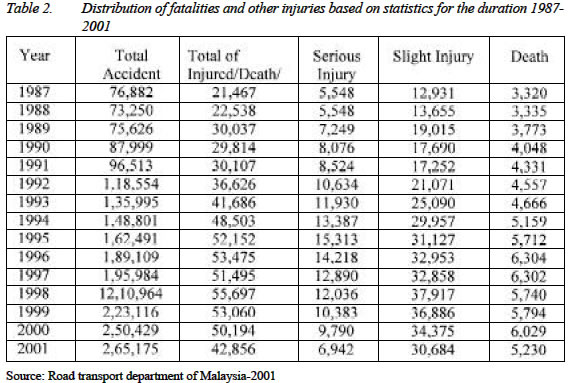
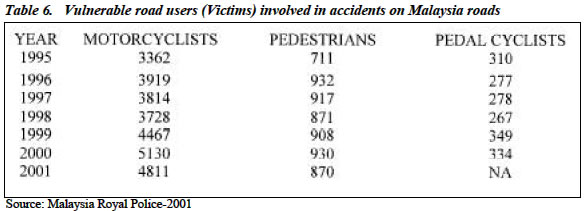
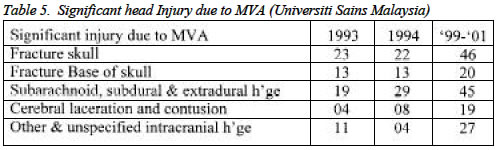
Malaysia Submitted-12.6.2002, Code Number: mj03020 Road accident is `a global tragedy' with ever-rising trend. The goal of this article includes review of the causes and nature of accidents, statistical data regarding road accidents and the economical impact. 1.17 million deaths occur each year worldwide due to road accidents 70 % of which occur in developing countries. 65% of deaths involve pedestrians, 35 % of which are children. Estimates suggest that 23-34 million people are injured worldwide every year in road crashes - a value almost twice that previously estimated. It is estimated that more than 200 U.S. citizens die each year due to road accidents abroad. Every year in Europe, more than 50,000 peoples are killed in road accidents, and more than 150,000 remain disabled. It is a sad fact that the total number of road accidents in Malaysia exceeded 223,000 in 1999. On the average, 16 persons died from these road accidents, every single day in 1999. Lack of attention, reckless driving, lack of proper protection, speeding, bad personal habits, social and behavioral misconduct and inconsiderate drivers of larger vehicles are some of the problems that cause accidents. In Malaysia, motorcycle fatal accidents (60%) warrant a high degree of concern. Young children and senior citizens are found to be in the vulnerable age group. In Malaysia, in 1999 alone, general insurers paid RM1.67 billion or an average of RM4.6 million a day on motor claims. It is now recognized that road traffic accidents represent a major public health problem, because of the high number of victims involved and because of the seriousness of the consequences for themselves and for their families. Key words : Global menace, road accidents, Malaysia INTRODUCTION Road accident is one of the major causes of death and injuries in Malaysia. In the year 2001, the total number of road accidents was 265,175 with fatalities of 5230, seriously injured 6942, and slightly injured 30,684. It is a shocking fact that road accidents kill more people in other developing countries too, every year, than war and disease. In Asia alone, 400,000 people are killed on the roads annually and more than four million injured. According to WHO, every year, nearly one million people are killed, three millions are severely disabled for life and thirty millions are injured in road traffic accidents. The social and economic, economical cost also proportionately increased by five times from 12,043 kilometers to 60,734 kilometers (2). About 25 % of the road network being Federal Roads, whilst the remaining 75% forms the State Roads. Over the last seven years from 1991 to 1997, the Malaysian economy has been growing at 7% annually. The number of registered vehicles showed a step pattern of increase. Between 1970 and 1997, the vehicle population has grown from 669,294 to 8,550,469, an average growth rate of about 47% a year or 13 times more than in 1970 (3). As on 31st. December 2001, Malaysia had a total vehicle population of 11.3 million (Table 1). Of this 5.6 million are motorcycles. Though high economic growth had transcended into high accident rate in Malaysia, recently it has witnessed a change in the trend. Malaysia has the second lowest road accident rate in ASEAN region, second only to Singapore. In a report published by the Malaysian Ministry of Transport, Malaysia had 5.7 deaths for every 10,000 registered vehicles in the year 2000, a drop from 8.2 deaths per 10, 000 registered vehicles in 1996. This is despite the fact that overall number of accidents had risen from over 189, 000 in 1996 to 240,417 last year as the number of registered vehicles had risen from 7.6 million to 10.5 million over the same period (4). In 1989, the fatality index for Malaysia stood at 9.0 fatalities per 10,000 vehicles. In 1997, the fatality index was 7.4, an improvement from 1996 figure of 8.2 fatals/10,000vehicles (3). Fatality figure due to road accidents increased from 3320 in 1987 to 6,304 in 1996 and decreased to 5230 in 2001. Total of seriously injured in road accidents increased from 5548 in 1987 to 15313 in 1995 and fortunately decreased to 6942 in 2001 due to the constant efforts of the government (Table 2). In the case of cars, however, the fatality figures declined from 1.89 per 10,000 registered cars in 1990 to 1.41 in 1996(2). Causes and Nature of Injury As elsewhere in the world, the causes of road accident are faulty vehicles, uneven roads, careless/reckless driving, speeding, drunk driving, inadequate sleep, alcohol and other drug effect and many more. According to a case-control study of 571 drivers involved in road crashes, it was found that driving when sleepy, driving after five hours' or less of sleep, and driving between 2 am and 5 am were associated with a substantial increase in the risk of a car crash resulting in serious injury or death. Such cases are responsible for up to a fifth of all such road crashes. The authors conclude that a reduction in these behaviors may reduce the incidence of injuries or death up to 19% (5). In Malaysia, according to the Ministry of Health, the incidence of motor vehicle accident in the year 1985 was 225 for every 10,000 vehicles to rising to 250/10000 in 1995 (Table 3). The number of casualties due to motor vehicle accident in the year 1998 was 52,218. During the year 1997-98, according to Ministry of Health Malaysia, accident was the third principal cause of hospitalization in hospitals and accident was the fourth principal cause of death behind heart diseases, septicemia and cerebrovascular accident. Hospital Universiti Sains Malaysia in Kelantan, a tertiary referral center with a neuroscience center, registered a total of 522 cases of head injury in the year 1997 and 570 in the year 1999. An analysis shows that the accidents are more common between motor vehicles and between motor vehicles and other non-motorized vehicles. Next comes, the accidents between motor vehicles and pedestrians (Table 4). In next two years, the total number of MVA swelled up to 1382 cases in Kelantan in which 428 were fatal- 8% of national incidence. Majority (95 %) of the patients who involved in the MVA were Malays. At any one time, the number of motorcycles is about 45-50% of total number of vehicles on the road posing the greatest challenge to road safety efforts in Malaysia. According to a study by the Road Safety Research Center of University Putra Malaysia, motorcyclists constitute about 55-57% of total number of road accidents and 60 percent of traffic fatalities in Malaysia. Their risk of injury is estimated to be 20 times higher than that of car passengers. The fatalities of motorcyclists and pillion riders have increased steadily from 1,570 in 1990 to 3362 in 1995 and 3,919 in 1996. On the other hand, fatalities per 10000 registered vehicles have declined from 8.9 per 10000 to 7.4 per 10000 in the period 1990 to 1997. The number of victims involved increased to 5130; 930; and 334 among motorcyclists, pedestrians and cyclists respectively in the year 2000 (Table 6). However, an interesting point was that motorcyclists' fatalities increased from 6 per 10000 in 1996 to 8.7 in 1997 after registering a high of 9.6 per 10000 motorcycles in 1999. (2) Surprisingly, the road transport authorities claim that 75% of the accidents between motorcycles and heavy and large vehicles is not due to the fault of motorcyclists! Improper use of helmets is a further problem, as only 55 percent are found using their helmets properly, the others did not strap it or strapped it loosely (6). According to data from the National Highway Traffic Safety Administration, motorcycle deaths are on the rise in the United States, even though it is a well developed country. Researchers, who published their findings in the February 2002 issue of the Annals of Emergency Medicine, reported that not wearing a helmet was a factor in more than half of the fatalities (7). But, even when the helmet is used, the motor cyclist must be very alert as a " legal" helmet is only effective up to and including 13 MPH impact speed, raising the reasonable doubt that the helmet will ever save the head from 80 mph or more. More than half of the fatalities in MVA proved to be due to over speeding. However, there is an appreciable decrease in the rate of speeding related fatal accident in Malaysia from 90 cases in 1998 to 69 in 2001. This might have been due to the detection of speedsters more accurately by ASRCS (Automatic Speed Radar Camera System and Laser Speed Camera). The impact on the victim and the property damage in MVA are due to the force, which is directly proportional to the weight (heaviness) and velocity. Speeding reduce time to response. However, according to the Director General of Road Transport Department in Malaysia, 40% of road accidents in the country is caused by following the front vehicles too closely, 26% dangerous cornering, 13% dangerous overtaking and 12% over speeding. Speeding-related crashes cost an estimated $28.9 billion per year. The major cause of death in road accident is severe head injury. Lawrence et al (8) had reported 483 victims including pedestrians out of 746 of total head injury patients are due to motor vehicle accidents (~ 65%). He pointed out 89% of the patients were in coma immediately following injury. Head injury ranges from minor injury to the scalp to severe damage to the brain. Jeret et al(1993) and Borczuk et al (1995) had reported that the commonest mechanism of injury was motor vehicle accident (9,10,11). In a study conducted at Universiti Sains Malaysia in 1999-2001, motor vehicle accident accounted for the commonest mechanism of injury in 75.5% of the total number. Minor head injuries constitutes about 70-80 % of all head injuries cases that are seen in the Accident and Emergency department. Serious head injury occurs in only 3% of non-vehicular and 15% of vehicular injuries(13). Susceptibility of the brain tissue to shearing forces plays a vital role. Rapid acceleration and deceleration of the head causes different levels in the brain to move differently relative to one another. This produces stretching and tearing of axons at the gray-white matter junction, swelling of the brain, increased intra-cranial pressure and brain herniation leading to grave consequences. Generally head injury does not occur in isolation. It usually is associated either with fracture of skull and/or limbs. In a study conducted at University Sains Malaysia in 1998, it was found that approximately 50% of 103 patients with intra-cranial hemorrhage had associated skull fractures (13). In another study conducted during 1999-2001 at the sample hospital, 54% of MVA cases had fracture in the skull vault and 23% had fracture base of skull. Out of these, the commonest type of skull fracture was linear (77%) followed by depressed fracture (22%) and mixed type (1%). Table 5 reveals that in 1993 and 1994, the association of skull fracture with head injury due to motor vehicle accident was lesser than in 1999-2001 (12). Stiell et al had show patients with basal skull fracture were at five fold increase risk of needing neurological intervention (11). Dacey et al pointed out that the presence of skull fracture increased the need of neurological operation by a factor of 20 (14). Under type of road users, the key road users in the traffic accident picture are motorcyclists, pedestrians and bicyclists (Vulnerable Road User type). Fifty percent or more of road deaths in cities involve pedestrians. 60% of all fatal road accidents involve motorcyclists (4). Motorcycle riders (including pillion passengers) sustain substantially more deaths and serious injuries than any other groups of road users accounting for 3362 (59%) of all traffic accident deaths in Malaysia in 1995. Pedestrians form the next highest group with 711 (12%) deaths, bicycle riders contribute 310 (5%) of deaths. All other vehicle drivers and passengers contribute 1096 (19%) deaths (Table 6). According to the government's figures, pedestrian causes more than 80% of vehicle/pedestrian accidents. This is mostly due to failure in following the necessary traffic regulations both by the pedestrians and drivers. In 1995, Borczuk concluded that pedestrians and bicyclists struck by cars were more likely to suffer from intracranial injury's with p value of 0.0004 and 0.002 respectively (10). Steill et al, in 2001, had reasoned out that certain injuries such as pedestrians struck by motorcycle, occupant ejected from motor vehicle, bicycle collision were found to be independently associated with brain injury (11). A pedestrian hit by a car at 30 km/h has less than 10% chance of dying, whereas this probability increases to more than 80% at 50 km/h. This is why all European cities are limiting vehicle speeds to less than 30 km/h in residential and shopping areas. As can be adduced from news reports, buses or heavy trucks can cause greater damage and more casualties than a car in a road accident. Drunk driving cannot be underestimated in the total making of road accidents. Drunk driving is found to occur in 949 persons in 1996, 706 in 1997, 1470 in 2000 and 1613 in the year 2001. Drunk driving accidents resulted in 57 casualties in 1996, 29 in 1997, 238 in 2000 and 179 in 2001. Another important distraction factor causing accident in Malaysia the use of `Hand phone'. According to NHTSA, 85% of all cellular customers are using the devices while driving; it estimates 20 to 30% of fatal accidents are due to "distractions"—including cell-phone usage. In1997, The New England Journal of Medicine reported the results of a University of Toronto study of 699 collisions and concluded that the risk of a crash more than doubled after 5 minutes of cell-phone use. The risk of a collision was between 3 and 6.5 times higher after 10 minutes of cell-phone use, compared with the risk for drivers not using cell-phones (15) Malaysia in the map of "Global Tragedy" Highest fatality rates (deaths per 10,000 motor vehicles) worldwide occur in African countries, particularly Ethiopia, Uganda and Malawi whilst fatality risk (deaths per 100,000 population) is highest in a disparate group of countries including Thailand, Malaysia, South Africa and Saudi Arabia. Every year in Europe, more than 50,000 peoples are killed in road accidents, and more than 150,000 remain disabled for life. Thus the European Union has today a rate of 200,000 bereaved families or families with a seriously disabled member, every year. The cumulative total of survivors is at least 6 millions in Europe, 100 millions in the world. In USA, more than injuries from injuries per year. It is now recognized that road traffic accidents represent a major public health problem, because of the high number of victims involved and because of the seriousness of the consequences for themselves and for their families. Lawrence et al reported 36% death, 37% disability in his series of 746 patients with head injuries (8). It is disheartening to see how much these bereaved families and families of severely handicapped victims are depressed, distressed, and even suicidal. These psychological sufferings are often intense, lasting, and even permanent. They may generate somatic illnesses, which worsen this psychological distress, creating a vicious circle. Long term consequences such as loss of memory, cerebral atrophy, hydrocephalus, loss of memory, loss of any part of the body, paresis, paralysis, depression etc. worsen their remaining life period. The involvement of vulnerable road users, i.e. pedestrians, cyclists, motorcyclists, the children and the elderly had a higher fatality involvement than with injuries in middle aged. The vast majority of pedestrian casualties occurred to the economically active cohort (21-60 years). In Asia-Pacific region, the highest percentages of pedestrian deaths (of the total) were found in Hong Kong (67 per cent), Korea and Sri Lanka (48 and 45 per cent respectively). Malaysia had 15 %; lowest in Thailand and China (9 & 11% respectively). Conversely, the percentage of Motor and deaths is highest in China (64%) and Malaysia is the second highest with 57%. Road accidents are a major cause of death for all children aged between 1 and 15 years. 1 out of every 14 deaths in children is from accidental injury. Many studies revealed that age is an important prognostic factor in predicting the outcome of head injuries.50% of accidents involve age group between 16-25.(4). Torner and schootmans in their review in 1996, found that the peak age with highest mortality is in the age group of 15-24 (16) and the mortality is steadily increasing with age. Pedestrian injuries account for most of the 280,000 childhood road deaths each year (17, 18). The UK has one of the worst child pedestrian fatality rates in Europe. The group most at risk is between 12 and 21. It is estimated that the probable number of road accidents involving children is 270,000 a year. Among countries in Asia-Pacific region, fatal injury percentage in children under the age of 15 years in Malaysia, Fiji and New Guinea are 11, 16 and 24% respectively. Between 200 and 220 children (under 14) are injured every year on the roads in Malaysia during the past five years. 1-3 % of them are killed. A systematic review including 15 controlled trials, 14 of which were in children, by Duperrex and colleagues in 2002 shows that safety education for pedestrians could improve children's knowledge of safe road crossing (17). In 1998, fatality rates for children aged 0-4 and 5-14 years were five to seven times greater in developing countries than in higher income countries. Vulnerable groups and also road traffic injuries in developing countries particularly affect the productive (working) age group (15-44 years). There exists a gross difference between developing and developed nations. In 1998, the fatality rate for children aged 0-4 years was 29.5 per 100 000 population in South East Asia and low income countries of the western Pacific region, compared with 4.5 deaths per 100 000 population in high income countries. For older children, aged 5-14 years, the fatality rate was 28.1 per 100 000 population in Africa compared with 4.8 for North America, Western Pacific countries, and high-income countries in Europe. In developing countries, mostly pedestrians, passengers, and cyclists are involved in accidents as opposed to drivers in the developed world. In the United States, for example, more than 60% of road crash fatalities occur in drivers, whereas drivers make up less than 10% of the deaths due to road traffic injuries in the least motorized countries. In developing countries, where most injuries occur in urban areas, pedestrians, passengers, and cyclists combined account for around 90% of deaths due to road traffic injuries. Urban pedestrians account for 55-70% of deaths. (16,17, 19,). Such accidents can bring considerable suffering, not only to the casualty themselves but also to family and friends. Most of the accidents in rural areas are caused by non-usage or improper use of helmets (not securing the helmet belt properly while riding.) The odds of children sustaining fatal or moderately severe injury in the front passenger seat are more than nine times higher for unbelted children than for belted ones, and for those in the rear left seat are more than twice as high (20). Comparative analysis puts Malaysia in the right place among some selected countries: Fatality rate of Malaysia stands high (8.4) while that of Singapore (4.3), Japan (1.3) and Australia (1.8) is very low. Likewise, fatality rate of motorcyclists also very high in Malaysia (7.2) when compared to Thailand (6), Singapore (4.2), Japan (2.6), Australia (2.9) and New Zeland (4). Countries like Germany, Finland, USA and Great Britain have fatality rates of 1.8 to 2.1 per 10,000 vehicles. In 1998, Malaysia notched up another world record after witnessing highest road accident in one holiday season during Chinese New Year and Hari Raya Puasa by recording a total of 9901 accidents killing 274 victims and causing fatal injuries in 240. In Belgium, the year 1998 counted 15,812 young victims (0-19 years old) of road traffic accidents. Results from several studies reveal that 35 to 50% of these children suffer from a Post- Traumatic Stress Disorder within three months following their accident. Three categories of factors have been specified to be responsible: the accident characteristics (objective and subjective severity), the child characteristics (personal history, emotional reactions, coping style), and the social environment characteristics (social support, family functioning). Senior Citizens - above 60 years of age- are vulnerable to frequent accidents because of decreased alertness, less responsive to dangers on the road, poor eyesight, poor judgment, and poor hearing. Jeret et al, 1993, Borczuk et al 1995 and Stiell et al 2001 had showed that patients with age greater than 60 years old tend to have significant intracranial injury than those are younger and they were at higher risk of developing brain injury following even minor head injury (9,10,11). Servadei et al, 2001, had stressed that patient over the age of 60 years old with minor head injury would be regarded as in a high risk group regardless of other clinical features (21). Lawrence et al (1991) concluded after studying 83 patients in old age group (out of a total of 746 patients of head injury) that they, particularly pedestrians, fared poorly. This is a product of not only their age but also greater frequency of systemic compromise, particularly hypotension and hypoxia(8). Impact On Economy And Insurance There is no doubt that motorization has contributed in a significant way to the prosperity of Malaysia. However, the price being paid for this is exorbitant. Road accidents in Malaysia resulting in injury or fatality, loss of man power, loss of productivity, high medical expenses, costly management, property damage and others are estimated to cost an annual economic loss of about RM 7 billion (4). The average per claim paid by insurers for physical damage to vehicles has continued to surge its upward trend to RM 4,293 in 1998 from RM 3,846 in 1995. The increasing numbers and cost of road accidents would only push insurance premium up and the sheer numbers of road accidents on Malaysian roads was a terrible „economic waste'' to the nation as a whole. Poor people in developing countries have the highest burden of injuries and fatalities due to road traffic crashes. In 1998, more than 85% of all deaths in road accident, 96% of all children killed, and 90% of disability adjusted life years lost worldwide because of road traffic crashes occurred in developing countries (18). According to Transport Research Laboratory-UK report on "Estimating Global Road Fatalities", during 1999 between 750.000 and 880.000 people died worldwide in road accidents; 85% of them in developing and transitional countries. Globally, in 1998, 51% of fatalities and 59% of disability adjusted life years lost due to road traffic injuries occurred in the productive age group. The global economic burden of road traffic crashes is estimated at $ 500bn (17, 18). In USA, these injuries drain economies of 1-2% of gross domestic product (about $100 billion) each year. The social-economic costs in Europe amounts to 200 billion EUR per year. This amount is of the same order as that of the total yearly car production in Europe. The Asia-Pacific Region accounts for almost half (around 0.5 million) of all estimated worldwide road accident deaths. The estimated economic loss in ADB's developing member countries is more than $35 billion annually. This is more than double the amount of annual foreign development aid they receive. General insurers are hurt from the high rate of road accidents in Malaysia. In 1999 alone, general insurers paid RM1.67 billion or an average of RM4.6 million a day on motor claims. During that year, statistics showed that there were 611 accidents a day or about 25 accidents an hour and at least 909 vehicles getting into accidents every single day and 16 persons were killed on Malaysian roads every day in 1999. However, Kelantan state stands in third place in the country in recording lowest fatal accidents. Highest fatal road accidents are recorded in 1998 in Selangor and Johor while Perlis recorded the lowest.The death toll on Malaysian roads is relatively high when compared to other countries. Road accidents significantly inhibit economic and social development. They are associated with millions of premature deaths and injuries, billions of dollars in medical costs, strain in welfare service, loss of productivity, low economic growth, and poverty. The General Insurance Association of Malaysia is concerned over the recent spate of accidents involving commercial vehicles. Statistics reveal that while buses plying the nation's roads have increased by 35.3 per cent to 47,674 in 1999 from 36000 in 1995, the average accident rate among buses in that period remained high at over 25 per cent. In 1999, the total number of commercial vehicles stood at 746,276 compared to 3,787,047-registered private car. The insurance compensation has proportionately increased. General Insurance Association of Malaysia's (PIAM) statistics show that the frequency of third party property damage and bodily injury claims involving buses are six times more than private cars, that is, 131 per thousand for buses compared to 21 per thousand for private cars. Furthermore, the average cost per claim for accidents involving buses is 62 per cent higher than that for private cars. For taxis, the claim frequency is three times higher than private cars while the average cost per claim is 33 percent higher. The number of accidents involving a taxi, on the other hand, was 6,773 giving an accident rate for taxis of 12.2 percent. For lorries or vans, the number of accidents was 49,982, giving an accident rate of 7.8 per cent. Compared to private cars, these statistics show that lorries and vans have a slightly higher propensity to get into accidents than private cars, whereas taxis were twice more likely to get involved in an accident than private cars. Conclusion A large-scale review by the Asian Development Bank (ADB) on regional road safety in 1996 and 1998 showed (summarized from the study's `Road Safety Guidelines for the Asian and Pacific Region' as well as the report on `Vulnerable Road Users in the Asian and Pacific Region') that the road deaths took the greatest toll on the Asia and Pacific region where 44 per cent of the world's road deaths occurred and only 16 per cent of the total motor vehicles are found. The analysis everywhere is based on official statistics. But, under-reporting of road fatalities is intensive. For instance, the actual number of China's road deaths has been estimated by the official Beijing Traffic Engineering Research Institute to be over 40 per cent greater than that reported in official statistics. Such discrepancies in data need to be re-emphasized here as it is quite likely that the actual current situation is much worse than that being reported and acknowledged. Malaysia is a federal parliamentary democracy with a constitutional monarch with a population of 22.7 million. Everyday, she faces the tragedy of 611 accidents, 16 deaths, 33 severely injured and104 contended lightly injured. Of all road accidents in Malaysia, the over-representation of motorcycle fatal accidents (60%) warrants a high degree of concern. However, road authorities can feel contended with the figures of 6029 deaths in the year 2000(fatality rate of 5.6) and 5230 in 2001 (fatality rate of 4.6) when compared to a fatality rate of 9 in 1989. It is greatly appreciable if the declining trend continues forever! The need for providing a safe and efficient road system has been a cause of concern to the Malaysian government. Extra measures such as good geometric design of roads with adequate sight distance, good, safer, pedestrian friendly streets and walkways, collapsible rubber poles, striking pavement marking etc. have to be taken up. Encouraging a culture of walking and cycling as an alternative to cars, providing. Safe routes, perhaps, discouraging the habit of owning one or more cars for every one in the family; and instead having one car for the whole family and frequent use of public transport are a few ways out. Accident fatality in Malaysia should be reduced thus saving millions of Ringgit in terms of productivity loss, property damage, medical cost, and others. Acknowledgement The author 15 grateful to Dr. Azian Abdul Aziz, Dr. Azman Kiflie, and Dr. Laili Suriani and to the Medical Record staff of Universiti Sains Malaysia- Kubang Kerian, Traffic Police Department, Police Head Kelantan state for their direct or indirect help in formulating this paper. REFERENCES
Copyright 2003 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj03020t5.jpg] [mj03020t4.jpg] [mj03020t2.jpg] [mj03020t6.jpg] [mj03020t1.jpg] [mj03020t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}