 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 10, No. 2, July 2003, pp. 60-65 Approaches and Methodological as well as Interpretative Issues In Quality Of Life Research In Malaysia C. I. Hasanah Department of Psychiatry, School of Medical Sciences,
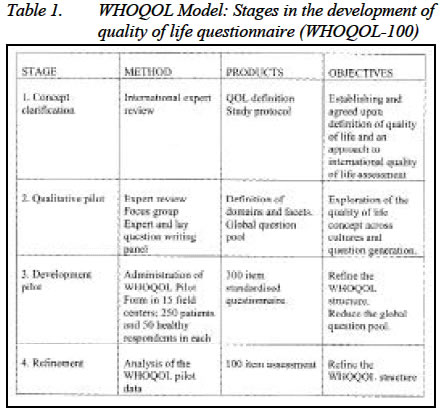
Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia Submitted-16.4.2003, Code Number: mj03023 Quality of life measures are designed to enable patients' perspectives on the impact of health and healthcare interventions on their lives to be assessed and taken into account in clinical decision-making and research. This paper discusses some approaches, methodological as well as interpretative issues of health related quality of life research. Key words : Quality of life, methodological and interpretative issues INTRODUCTION Quality of life (QOL) has become an integral variable of outcome measures in clinical research and is being incorporated into pre-consultation and follow-up assessments on individual patients. The recognition of the importance of understanding the impact of healthcare interventions on patients' lives rather than just objective disabilities as well as mortality is particularly important for patients with chronic, disabling or life threatening diseases who live without the expectation of cure. Despite its utility, there is still no agreed definition or method of assessment, and clinical significance of research results are frequently left undefined. The objective of this paper is to highlight those aspects of quality of life study that Malaysian researchers may find useful in choosing or designing their assessment tools and presenting their results. Conceptual issues The concept of "quality of life" developed in the social sciences was first applied in medical practice to determine if available cancer treatments could not only increase the survival time of patients but also improve their sense of well being (1). Up to date, there is no single definition of quality of life that is universally accepted. The emerging of new assessment tools amidst many already available, reflect the myriad definitions of quality of life. A number of assessment tools were actually claiming to assess quality of life when in actual fact they are looking into assessment of disability or impairment. From clinical practices as well as researches there are enough evidences to say that quality of life is at least partly independent of health status (2) and "is a reflection of the way that patients perceive and react to their health status and to other non-medical aspects of their lives" (3). Many authours maintained that quality of life is inherently subjective and that only perceived wellbeing, not functional assessment, should be used to determine quality of life (4 & 5). One questionnaire that has been widely considered and used in assessing quality of life in researches in Malaysia is the 36-item short-form (SF-36) questionnaire (6). SF-36 was constructed to survey health status in the Medical Outcome Study and it did not consider individuals' opinion on their satisfaction with the various aspects of their life. Measuring someone's ability to perform common tasks or activities is putatively objective, while asking patients to rate the effects of health status on personal wellbeing is explicitly subjective. For example, the question "Are you able to carry two bags of groceries 20 yards?" seeks explicitly behavioural information, whereas "Does your health interfere with your enjoyment of life?" invites respondents to make subjective ratings. Almost all items focused on the functional status of the individual and do not asked patients' appraisal of how their health affects their quality of life (7). Of interest is the WHOQOL (100 items questionnaire), developed by World Health Organization. The multi-domains approach to quality of life by WHO is based on its definition, "Quality of life can be defined as the individual's perception of his/her position in life in the context of the culture and value system in which he/she lives and in relation to his/her goals, expectations, standards and concerns". WHO's quality of life scale is unique from the others, as it is multi-centered (15 centers) and cross-cultural from the beginning of its conception. The validation of the abbreviated version with 26 items (WHOQOL-Bref) incorporated data from its collaborative center (Universiti Sains Malaysia) in Kelantan, Malaysia. The transcultural approach as well as collaboration with a center in Malaysia and other Asian countries, makes it easily adopted into study on quality of life in Malaysia. WHO's concept and definition of quality of life conforms to a subjective assessment, that is pertaining to an individual's judgement or cognitive assessment of personally important aspects of life and sets it apart from many other scales. Dividing the assessment into physical, psychological, social and environmental domains provides further structure for understanding the effects of health status on quality of life. Contrary to quality of life instruments that produce composite indices this multi-domains instrument offers precision and clarity. Multi-domain measures also served the investigators different aspects of quality of life that are of interest for different studies. Two general questions in WHOQOL-Bref i.e. on assessment of quality of life and satisfaction with health enable one to analyze the criterion validity of the questionnaire. Choosing the quality of life instrument. One of the reasons behind the rapid development of quality of life measures in health care has been the growing recognition of the importance of understanding the impact of healthcare interventions in patients' lives rather than just on their bodies. This is particularly important for patients with chronic, disabling, or life threatening diseases who live without the expectation of cure and have conditions that are likely to have an impact on their physical, psychological, and social wellbeing (8). Researchers in Malaysia are often not sure of which quality of life assessment to use and frequently resort to the one already translated and validated, which are not many. Those used in published studies overseas are mostly developed in North America and the United Kingdom. Translating these questionnaires for use in the local population or setting is not only time consuming, but may results in items with different meanings between the source and target populations. When a study incorporating QOL is being designed, the following key questions should be addressed to put into context the clinical significance of expected QOL results.
In Malaysia, researchers with interest in different illnesses will find that the generic measures are either insensitive to the types of changes resulting from intervention with specific diseases or that they simply do not include items important to a particular area. Choosing the right questionnaire may be a problem and translation of a questionnaire from source language to the target population's language is another problem. In scientific research this needs to be done by an acceptable process and the translated version is yet to be pilot tested for validity and reliability. Despite the less work involved in translating accepted questionnaire to the language of target population, there are researchers who probably find that the available questionnaire does not comprehensively cover aspects of quality of life that they intend to assess. For some, there is no available tool to measure aspects of QOL specific to illness or disease under study. These researchers probably could not avoid designing a novel illness specific quality of life questionnaire and probably have to start their research with a qualitative research design. The advantage is that one will get an assessment tool that is tailored to the illness and the population under study. Available questionnaires may not include aspects that are considered important for our population, e.g. religious, spiritual or cultural practices or may have item that is important in the source population but with pejorative connotation in our culture, e.g. being independent of other people's help may be considered as selfish. Translation methodology Translation process as proposed by WHO involves, a number of steps. One or two translators are normaly utilised persons if two translate the source instrument into the target language, they consult one another in the course of their work. These translators should have a clear and detailed understanding of the instrument, and the population who will use the instrument. This will increase the likelihood that the instrument is translated appropriately, and that the language used in the translated document matches closely the language usage of the target group. At least four mono lingual and a bilingual panel made up of flora to six individual are needed to amist in remaining the transtated qushonaie. The adjusted and finalized document is then back translated into the original language by the back-translator who had never seen a copy of the original English version before completing the translation. The bilingual group then considers the original and back-translated documents. Any significant differences should lead to iterations in the process until an acceptable conceptual, semantic and technical equivalence has been achieved. The author of the questionnaire will endorse the translated version and this may only be done after approval of the back-translation. Translation of the quality of life instrument may be initiated by the organization that originally designed the questionnaire. One example is the functional assessment of chronic illness therapy organization (www.facit.org) that has included the author as a bilingual assessor for their FACIT Multilingual Translations Project. A number of their disease specific assessments have been validated. Their web site will indicate the available Malay versions. Development of quantitative tools from qualitative study; designing a new questionnaire. A quantitative phase, dedicated to the psychometric analysis and construct validation of a QOL measurement scale must be preceded by a qualitative phase. Its goal is to create an initial list of items under identified facet or domains of QOL to be submitted for psychometric analysis. Data came from in-depth interviews as well as focus groups conducted with therapist as well as sufferer of illness to be studied. In a large scale and well-conducted study, a large number of items are generated and may require a computer-based content analysis (using NUD*IST software). This type of work requires a team effort from clinical expertise and allied therapists for the specific illness, psychometrician as well as a linguist. As a guideline, the work for WHOQOL questionnaire is summarized in table 1. Interpreting QOL results Having discussed the conceptual issues and methodological approaches in assessing QOL, we are left with the issue of interpreting the results of the QOL. The outcomes of the QOL research are usually intended for various audiences. They are patients, health care practitioners, clinical researchers and policy makers. For patients, the changes in their QOL with treatment or intervention communicate to their care giver how aspects of their life that were perceived cognitively or subjectively have been translated objectively, and how progress have been shown by changes in each domain or by a composite score. Generally for an individual patient, whatever improvement in the score is a significant improvement. This is important as studies show that physicians' perception and ultimate decisions regarding the patient's needs and desires frequently differ from the patient's own reports (9.10,11,12 &13). Without a structured approach to these data, the patient's perceived QOL needs and goals for treatment are either ignored or misinterpreted. Assessment of QOL has been incorporated into patient's data. A research group at Northwestern University has accomplished an example of this. The patient is given a general QOL measure such as the Functional Assessment of Cancer Therapy, which is scored electronically as the patient waits for his or her clinical appointment. The resultant data are summarized for the clinician and become part of the vital statistics for that day's consultation with the patient (14). Interpretation of QOL results by clinical researchers as well as policy makers focused on group differences. Often researchers presented their results by emphasizing level of statistical difference as reported by P values. Smaller P value is interpreted as larger difference in QOL. The greater the change the treatment intervention has on QOL, the more likely physicians are to take notice of this information. Unfortunately P values do not indicate whether this particular finding has clinical significance. All it means is whether the results of the study are found purely by chance, or otherwise. Methods used to measure QOL questionnaire's responsiveness to change are relative change (15), effect size (16), relative efficiency (17), standardized response mean (18), responsiveness statistic (19), paired t statistic (20) and standard error of measurement (21). These statistical measures, by themselves, do not provide an evaluation of the significance of the change, i.e., whether the change is minimally important to the decision-maker. Each measure is a quantitative descriptor of change. Researchers in reporting their results should include guidance on clinical importance of observed change in QOL. Further, they should comment on the extent of statement of the clinical importance as appropriate and empirically warranted. Many who are interested in the result of the study may not be very familiar with the ways used in assessing meaningful change in quality of life. Thus, it is best for the researcher to use an easy-to-understand rule of-thumb approach to indicate clinical significance (e.g., changing QOL score by 10%). Estimates of clinically significant change can be divided into those that are instrument specific and those that are study specific. Instrument-specific estimates may be derived from normative or defined sample validation data, whereas study-specific estimates are derived from clinical trials (22). As an example, an instrument-specific estimate, illustrates that a 9-point difference in physical functioning on the 36-Item Short-Form Health Survey is equivalent to the effect of having arthritis or back problems, "a clinically meaningful difference." (23) For a policy maker or an administrator, results that include cost-effectiveness analyses (CEAs) are more relevant. This is obtained from quality-adjusted life-year (QALY) and its cost. QALY attempts to capture gains from reduced morbidity and reduced mortality and integrate these into a single measure. The metric used is from 0 for death to 1.0 for perfect health. If by certain treatment, a person QOL index could be maintained at 0.5 for 4 years, then the QALY is 2 years. Besides the statistical jargon that one needs to understand to make a sense of the clinical significance of QOL change, there are other issues that are beyond the accepted length of this paper. The paper "Assessing meaningful change in quality of life over time: A users' guide for clinicians" is highly recommended for Malaysian researchers (24). Conclusions Health related quality of life research is here to stay, and is incorporated in the latest clinical trial research. Clinical researchers and practitioners should be able to understand the approach, methodologies and interpretative issues associated with such studies to be able to assess meaningful change in quality of life. Acknowledgement The author wishes to thank WHOQOL group and FACIT Multilingual Translations Project, Center on Outcomes, Research, and Education (CORE) for giving her the opportunity to work with them as well as for the advice and resources provided. REFERENCES
Copyright 2003 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj03023t1.jpg] |
| |||||||||

{kind=link}