 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 10, No. 2, July 2003, pp. 66-70 Prevalence and ethnic distribution of Helicobacter pylori infection among endoscoped patients in North Eastern Peninsular Malaysia Gurjeet Kaur and Nyi Nyi Naing* Department of Pathology and *Unit of Biostatistics and Research
Methodology, School of Medical Sciences, Universiti Sains Malaysia,
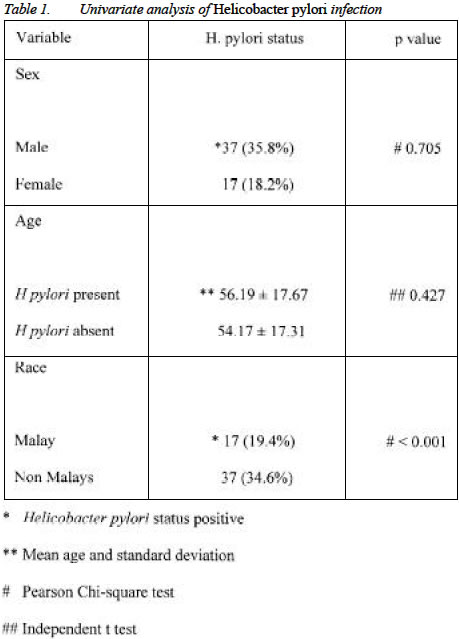
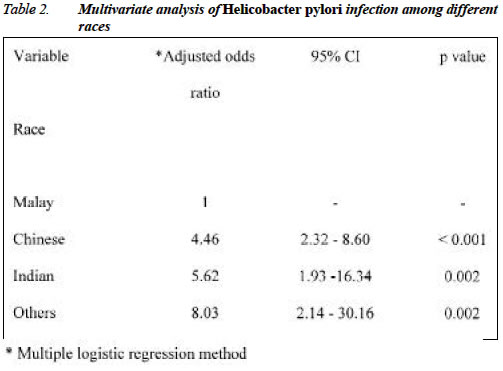
Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Code Number: mj03024 Objective: The objective of this study was to determine the prevalence and ethnic distribution of Helicobacter pylori infection in an endoscoped population in North Eastern Peninsular Malaysia. Methods: Pathology records of 400 consecutive gastric biopsies received at the pathology laboratory in a university hospital were reviewed. Demographic data of patients including their ethnic groups were documented. Evidence of gastritis and H. pylori infection were ascertained by routine histology and Warthin Starry stain. Univariate and multivariate analysis were applied to determine the prevalence of H. pylori infection in the sampled population and the difference in prevalence among the ethnic groups. Results: The overall H. pylori infection prevalence rate was unusually low at 13.5% (54 of 400) in this region. The prevalence among the races were as follows: Malay 6.6% (17/256), Chinese 24.1% (27/112) and Indian 28.6% (6/21). Gender and age were not significant associated factors for H. pylori infection. However there was an increased risk of H. pylori infection in Chinese (OR= 4.46, 95%CI, 2.3-8.6) and Indians (OR=5.6, 95%CI, 1.9-16.3) compared to Malays. Conclusion: The difference in prevalence of H. pylori infection between the three major ethnic groups concurs with other studies done in Malaysia. The reason for this interesting finding is uncertain and is suspected to be due to different environmental, genetic and socio-cultural practices in the various races. Key words : low H. pylori prevalence, ethnic difference, Malaysia Demographic data of patients including their ethnic groups were documented. The presence or absence of H. pylori in gastric biopsies was noted using Warthin Starry stain. Histological gastritis was deemed as present or absent. Other histological variables were not looked into. When a subject was endoscoped repeatedly, it was regarded as a single case and H. pylori status was regarded as positive if any of the biopsies demonstrated the organism. Statistical analysis Univariate and multivariate analyses were applied to determine the prevalence of H. pylori infection in the sampled population, the difference in prevalence among the ethnic groups and factors influencing H. pylori infection. Chi-square and independent t tests were applied in univariate analysis. Multiple logistic regression was used to determine influencing factors for this infection. Adjusted odds ratio with 95% confidence interval and its corresponding p-value were applied. RESULTS A total of 400 pathology reports of endoscoped subjects were studied, of whom 265 were male (male: female ratio 2.3:1). The mean age was 54.4 years with a range of 2 years to 97 years. The ethnic composition of the group was as follows: Malay 256 (64% of subjects); Chinese 112 (28%); Indian 21 (5.2%) and `other races' 11(2.8%). The `other races' category composed of ten Thais and one Caucasian. The overall prevalence of Helicobacter pylori infection among endoscoped patients was 13.5% (54/400). The prevalence among the races were as follows: Malay 6.6% (17/256); Chinese 24.1% (27/112); Indian 28.6% (6/21); other races 36.4% (4/11). The Caucasian was negative for H. pylori. Using univariate analysis, there was no significant difference in gender and mean age between H. pylori positive and negative subjects (table 1). However there was significant difference of H. pylori infection among the various ethnic groups and this was further substantiated with multivariate analysis (table 2). Chinese had 4.5 times higher odds of being infected with H. pylori (OR 4.46, 95% CI 2.32-8.60) while Indians had about 5.5 times (OR 5.67, 95% CI 1.93-16.34) and `other races' about 8 times (OR 8.03, 95% CI 2.14-30.16) higher odds of being infected. The overall prevalence of gastritis was 62% (248/400). Twenty two percent of patients with gastritis were positive for H. pylori. All H. pylori infected subjects had evidence of histological gastritis. DISCUSSION Epidemiological studies have documented great differences in the prevalence of Helicobacter pylori infection in different populations and ethnic groups. This variability is likely to be related to differences in environmental, bacterial and host factors. Seroepidemiological studies and endoscopic surveys in Malaysia and Singapore report an overall high prevalence rate of H. pylori infection between 26-60% (1-5). In contrast, North Eastern Peninsular Malaysia has an unusually low prevalence rate of about 5% in the general population and 13-15% among endoscoped dyspeptic patients (6,7). Patterns and distribution of H. pylori infection among different ethnic groups living in the same country is interesting and may provide valuable insights into the possible modes of transmission of the organism. There are three major races in Malaysia and Singapore namely Malays, Chinese and Indians. Various studies done in both countries have consistently shown a higher prevalence of H. pylori infection among non-Malays compared to Malays (1-6). A 49% prevalence of H. pylori infection was recorded among dyspeptic Malaysians in an urban area in the west coast of the peninsular, with prevalence of 16.4% in the Malays, 48.5% in Chinese and 61.8% in Indians (1). Our study conducted in North Eastern Peninsular Malaysia showed an overall H. pylori infection prevalence rate of 13.5% with the highest prevalence among Indians (28.6%) followed by Chinese (24.1%) and Malay 6.6%. The low overall prevalence validates a previous study done in the same population (6). This may be attributed to the predominantly Malay population of this North Eastern state. The similar difference in prevalence among the various ethnic groups is reflected in asymptomatic Malaysian children (3). In our study it was interesting to note that Thai patients had a much higher prevalence of 40% notwithstanding the small number of patients in this group. The reason for racial differences in H. pylori infection rates is unclear. Transmissibility of H. pylori is still debatable but generally, oral-oral and oral-fecal routes are thought to be the main modes of spread. Most infections are acquired in childhood (8,9). The increased risk of infection in Indians, Chinese and Thais may be due to different socio-cultural practices peculiar to each race. Communal eating habits allow close personal contact and this is practised in many Asian communities. Religious rituals and diet are among other factors that should be studied. Another strong plausible explanation as to the wide difference in infection rates among the races is the inherent genetic predisposition that plays a role in host-bacteria interaction. This needs to be investigated. Low socioeconomic status associated with high-density living and inferior hygienic conditions is thought to play a major role in transmission of the organism (8,9). The socioeconomic status was not detailed in our study though it is generally considered that the population in this North Eastern region is poorer and more rural compared to the west coast of the peninsular. Though urbanization and overcrowding may contribute to transmission and perpetuation of H. pylori infection, this would be reflected uniformly among the races. However, this is not depicted in the racial differences in infection rates seen in both urban and rural areas. Gender and age did not prove to be significant risk factors for H. pylori infection in our study, in contrast to another study that showed these variables to be independent risk factors (1). Study of gastric biopsies showed that only 22% of histologically diagnosed gastritis cases were associated with H. pylori infection. All H. pylori-infected subjects had histological gastritis. The limitations of the study include insufficient details of the patients with regards to indication for endoscopy and drugs consumed. The prevalence of duodenal and gastric ulcers was not determined as information on pathology request forms was often incomplete. Histological gastritis was not classified according to an international classification as this was a retrospective study and several pathologists were involved in reporting the slides. Furthermore a report pertaining to this aspect and conducted in the same geographical area has already been published (7). In conclusion there is a significant and consistent difference in H pylori infection prevalence rates among the various ethnic groups in Malaysia, being highest in Indians followed by Chinese and unusually low in Malays. The reasons for this is uncertain and various cultural and genetic factors need to be studied to further help understand the epidemiology and transmission of this infection. Acknowledgement This work was supported by the Universiti Sains Malaysia incentive research grant USM/PPSP/Ger. Peny.(6). REFERENCES
Copyright 2003 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj03024t2.jpg] [mj03024t1.jpg] |
| |||||||||

{kind=link}
{kind=link}