 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 10, No. 2, July 2003, pp. 76-83 AMBULATORY BLOOD PRESSURE MONITORING PROFILE AS A USEFUL PROGNOSTIC TOOL IN PATIENTS WITH PRIMARY HYPERTENSION A. L. Mohamed, E Katiman*, J Abu Hassan* International Medical University Clinical School, Seremban, *Klinik
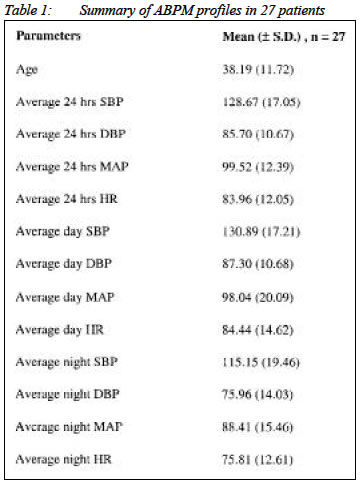
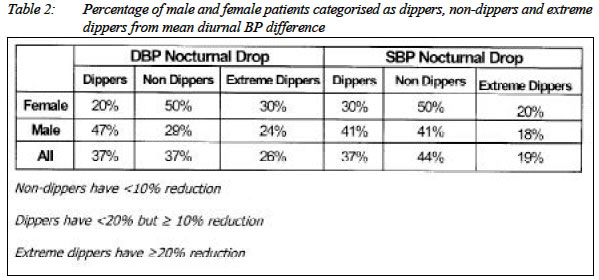
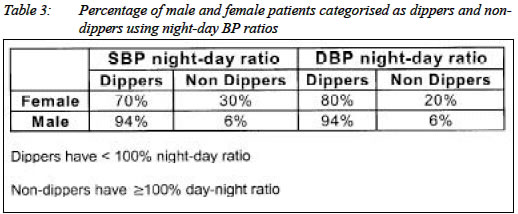
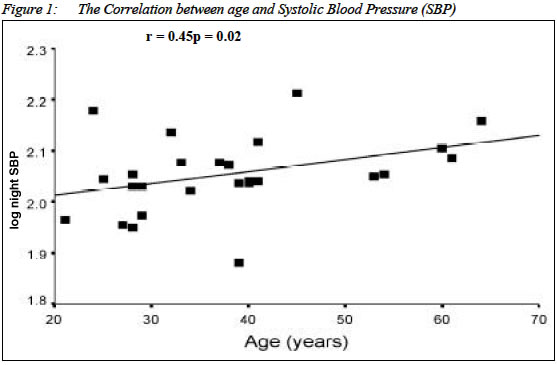
Pakar AzZahrah, Bandar Baru Bangi Submitted-11.5.2003, Code Number: mj03026 Ambulatory blood pressure monitoring (ABPM) devices are increasingly being used in the assessment of hypertension. The purpose of the study was to investigate patient's diurnal BP variation and to further determine the differences of BP readings between male and female patients and the effects of age in patients who attended the clinic with essential hypertension. In addition, evidence of relationship between the parameters recorded by 24-hour ABPM was also investigated. This study was conducted in an outpatient specialist clinic. Two indices were used to demonstrate the diurnal BP variation. Firstly, the diurnal systolic blood pressure (SBP) and diastolic blood pressure (DBP) variations which were calculated as night/day BP ratio for SBP and DBP respectively. Anyone scoring less than 100% were categorised as dippers. Secondly, nocturnal falls in SBP and DBP were calculated as (awake SBP-sleep SBP)/awake SBP x 100 and (awake DBP-sleep DBP)/awake DBP x 100 respectively. The results showed that there was no significant difference in the mean BP between male and female patients. In general, the study sample were categorised as dippers and non dippers. There were more male dippers than female dippers. Finally correlation analysis revealed that age is related to SBP variables whilst night HR showed positive correlation with night time BP. It is concluded that ABPM was shown to be a useful tool to analyse the variation and prevalence of cardiovascular risk markers in hypertensive patients and can easily be done in an outpatient set-up. Key words : hypertension, ambulatory blood pressure monitoring, diurnal blood pressure variation INTRODUCTION Over the past years, ambulatory blood pressure monitoring (ABPM) devices are increasingly used in the assessment of hypertension. One important indication for the use of ABPM is to exclude white coat hypertension, which affects 15-30% of the general population. This technique is also helpful in the diagnosis of patients with borderline hypertension, in looking at the efficacy of antihypertensive treatment1 and identifying nocturnal hypertension. Studies showing its value in diagnosing and treating hypertension in the pregnant (2) and elderly (3) patients have also been highlighted. Realising the popularity of ABPM, the British Hypertension Society has produced its own recommendation on the use and interpretation of ambulatory measurement (4). Although there has been much debate about its use over the conventional sphygmomanometer, there is now a firm evidence of its prognostic value in predicting cardiovascular outcome (5). ABPM is advantageous such that it allows multiple measurements throughout the day and night that can be plotted to represent the blood pressure profile later on. In practice, this is useful in governing decisions especially when ambulatory measurement has permitted a number of phenomena in hypertension to be identified. The trend now sees not only the well-developed countries struggling to combat hypertension but also in other parts of the world including developing countries like Malaysia. A recent national survey (The Malaysian Health and Morbidity Survey II) indicated 24% of the population is hypertensive. This finding has risen for the past several years mainly due to changes in lifestyle. The distribution of hypertension in the Malaysian community shows that the Malays which forms the majority of the Malaysian citizen, have the highest risk of getting high blood pressure compared to the Malaysian Chinese and to a lesser extent in the Indians. Therefore, the use of ABPM is as important in Malaysia as well as in other regions where hypertension is prevalent. The use of ABPM in Malaysia is mainly confiled to the main public hospitals in major cities. Usually patients who have their ambulatory measurements are those who have been referred from the hypertensive outpatient clinic. However with the growing popularity of private health care, more people are accsible to specialist services and hence, to refer for further investigation such as ambulatory blood pressure measurement. This study will look upon the ambulatory blood pressure profiles recorded in a private outpatient specialist clinic, AzZahrah Medical Specialist Clinic. The main aim is to explore the diurnal BP variation in subjects with essential hypertension and to determine the differences of ABPM readings between male and female patients. In addition, any evidence of relationship between the parameters recorded by the 24 hour ABPM will also be investigated. Methodology Population Studied Twenty-seven patients were assessed over 5 months of the study period. They were identified as having mild to moderate essential hypertension and those who underwent ambulatory blood pressure measurement. 17 of them were male and 10 were female with their age ranges between 21 to 64 years old (mean 38.19 ± 11.7). The main indications for an ABPM were to rule out white coat hypertension and for determining the effectiveness of anti-hypertensive therapy. ABPM measurement ABPM was performed on 27 consecutive patients from mid October 2001 to mid February 2002. The data obtained for each study were transferred into standard computer analysis software, MAPASAV PLUS version 1.0. The following parameters available from MAPASAV PLUS 1.0 were analysed : average 24-hour systolic blood pressure (24 SBP), average 24-hour diastolic blood pressure (24 DBP), average 24-hour mean arterial pressure (24 MAP), average 24-hour heart rate (24 HR), daytime systolic blood pressure (day SBP), daytime diastolic blood pressure (day DBP), daytime mean arterial pressure (day MAP), daytime heart rate (day HR), night systolic blood pressure (night SBP), night diastolic blood pressure (night DBP), night mean arterial pressure (night MAP) and night heart rate (night HR). All measurements were taken every 30 minutes within the 24 hours of ABPM. Daytime blood pressures were defined as the mean BP from the time the patient awake until bedtime. Night blood pressures were defined as the mean BP taken between the times the patient went to bed until awakening time. Day and Night Blood Pressures Variation Mean daytime and night time ABPM readings were analysed to determine diurnal BP variation and any evidence of nocturnal BP falls, known as "dipping". Two indices were used to demonstrate the diurnal BP variation. Firstly, the diurnal SBP and DBP variations were calculated as night/day BP ratio for SBP and DBP respectively (expressed as percentage)6. Those who had a night-day ratio of less than 100% were categorised as dippers whilst scoring 100% or more were grouped as "non- dippers" (absent of nocturnal BP falls). Secondly, the nocturnal falls in SBP and DBP were calculated as (awake SBP-sleep SBP)/awake SBP x 100 and (awake DBP-sleep DBP)/awake DBP x 100 respectively7. Dippers were defined as having <20% but > 10% reduction, non-dippers were defined as having <10% reduction while extreme dippers were signified as having >20% nocturnal BP reduction. Statistical Analysis Statistical analysis was performed using SPSS for Windows Version 10.0. Student's t-tests was used to compare the means of the parameters recorded in ABPM between male and female patients. Correlation matrix was introduced to test the presence of relationship among the continuous variables measured in ABPM. Linear regression analysis and Spearman's Rank Coefficient were performed to assess the type of association and strength of correlation in the associated variables. A p value of < 0.05 or 95% confidence limit was considered as significant. RESULTS Demographic data A summary of the ABPM profiles is illustrated in the Table 1. The table shows 27 subjects, 17 men and 10 women who were involved in the study with mean age of 38.1 ± SD 11.7 years. All had presented with a history of essential hypertension. The mean successful reading determined by the ABPM study was 46 readings throughout the period of study and an average of 6 readings at night was obtained. The patients' average 24 hours SBP and DBP were 128.7 ± SD 17.1 mmHg and 85.7 ± SD 10.7 mmHg respectively. The average 24 hours HR was 84.0 ± SD 12.1 beats per minute while the average 24 hours MAP was 99.52 ± SD 12.39 mmHg. Mean differences in male and female patients In males and females, there were no striking difference in terms of the mean age; mean difference in average 24 hours SBP, DBP, MAP and HR; mean difference in average daytime SBP, DBP, MAP and HR; and mean difference in average night time SBP, DBP, MAP and HR (refer Table 2). However, male patients had a slightly higher result in all the BP measurements with an exception to the average night time DBP when the female patients' reading exceeded the males'. The corresponding records for the average 24 hours SBP/DBP for males were 130.59 ± SD 14.49 mmHg / 86.24 ± SD 8.04 mmHg and 125.40 ± SD 21.15 mmHg / 84.80 ± SD 14.57 mmHg in females. Analysis using student's t-tests did not show any significant difference in all the parameters measured by ABPM between male and female patients. The Student's t-test outcome for age between male and female patients was similarly shown to be insignificant (t = 0.072, p = 0.943). Thus, regardless of the gender difference, the male and female patients in the study seemed to have comparable ABPM parameters. Nocturnal BP drop and variation of night-day BP ratio Two indices were used in illustrating the differences between day and night BP or in demonstrating the nocturnal BP drop. In the first index, the mean nocturnal drop expressed in percentage for the SBP and DBP was 12.03 ± 9.63% and 12.99 ± 11.63% respectively. Thus in general, the 27 patients were categorised as dippers because they quantitatively achieved > 10% but < 20% nocturnal BP drop. On the other hand, calculation of the SBP and DBP night-day ratios produced 87.97 ± 9.63% and 87.01 ± 11.63% respectively. Consistent with the first result they were similarly classified as dippers for having < 100% night-day ratio. Furthermore, in examining the DBP nocturnal drop; 37% of the total of 27 patients were dippers and the same percent equally applies for non-dippers. The remaining 26% patients were in the additional group called extreme dippers. For the nocturnal fall in SBP, the percentage for dippers, non-dippers and extreme dippers were 37%, 44% and 19% respectively (Table 2). Interestingly, using this index, the extreme dippers group were more common in females compared to males. Table 2 also shows that 50% of females were non-dippers for both SBP and DBP. In contrast, the percentage was lower for males, only 29% have absent nocturnal DBP fall and 41% males have absent SBP fall. Table 2 shows the results of BP variations calculated using the night-day BP ratios. Using the night-day ratio, the extreme dipper category was excluded. In this case, extreme dippers were generally called dippers. Therefore, there were more overall dippers calculated using this index in SBP and DBP as compared to the other methode of calculation. Nonetheless, consistent with the previous result, the majority of dippers were males compared to females. The rest of the summary for SBP and DBP night-day ratios is shown in Table 3. Linear regression and correlation analysis Linear regression analysis revealed there was an association between the following parameters : age and 24 hours SBP (r = 0.475, P = 0.012); age and average day SBP (r = 0.447, p = 0.019); age and average night SBP (r = 0.449, p = 0.019); night HR and average night SBP (r = 0.408, p = 0.035); and night HR and average night DBP (r = 0.511, p = 0.006). In short, there were weak but significant correlations between age and SBP in general and between night HR and night BP. There were no significant correlations observed in the other variables. Figure 1 illustrate these positive correlations: DISCUSSION ABPM devices are increasingly used in the management of hypertensive patients. They allow a better understanding of blood pressure fluctuations over 24-hour periods compared to simple clinical measurements. In this way, variety of patterns that can be used as an indicator towards various blood pressure states can be identified. With the help of ABPM, it is also possible to distinguish the differential status of dippers and non-dippers. This clinical study found that the technique has been useful in detecting patients with a white coat effect. This is an important issue since white coat hypertension has been postulated to be a precursor to hypertension and cardiovascular dysfunction (8,9). In the present study, it was found that the patients' average age was approximately 38 years old. In fact, the frequency age for patients involved in the study was within the range of late 20s and 30s years of age. This suggests that those involved in the study were relatively young hypertensive patients. Although this is the case, managing hypertension and prevention of hypertension as a risk factor to cardiovascular disease in the younger population is essential and should be emphasised. Further investigations such as biochemical studies, chest X-ray and ECG could be helpful in assessing the potential cardiovascular risks in these patients. In a study conducted in South Africa where the subjects were all medical students aged 21 years, abnormal BP pattern was demonstrated in young black participants (10). Thus, the study has further strengthened information that risk factors leading to cardiovascular disease are apparent at an early age and hence necessities prevention regardless of the age. Compliance with medication, effectiveness of therapy and good hypertension management are among the principles needed in monitoring BP. These principles are reflected in the results achieved in the group studied. Even though the 27 patients could be considered as "young" hypertensives, their mean average 24 hours SBP and DBP were in a good range (128.67/85.70 mmHg), implying these patients had a reasonably well-controlled blood pressures. These results may also be used to indicate optimum control of patients under follow-up in the clinic set-up, which can be used as an audit tool. As control of blood pressure, demonstrated in the infamous "rule of halves" are usually found in only 12.5 % of the total hypertensive patients; ABPM is recommended to be used as a method of assessment in clinic set-up to determine the control of blood pressure in the follow-up of hypertensives patients. The present study revealed that most patients were categorised as dippers. This is in keeping with the fact that in general, the patients had good BP control. Being a dipper is good because non-dippers in hypertensives patients. carry an increased risk of cardiovascular disease. Many studies have found that those who exhibit absent of nocturnal BP fall are associated with increased rates of damage to target organs and have increase risk of stroke (7,11,12,13). In addition, those who are called non-dippers have different response to antihypertensive treatment than dippers such that they are more difficult to treat (14). Nonetheless, despite the `true' absent of BP fall, patient's factor must be considered first before categorising them as non-dippers. Factor such as whether or not they are compliant with medication resulting in poor BP control may be a simple fact why they show diminished effect of nocturnal BP drop. It is essential to consider this first rather than jumping to the conclusion that a patient is resistant to therapy. Application of the night-day ratio showed that there was a higher percentage of dippers calculated, (85% in SBP and 89% in DBP) compared to the values given in the nocturnal BP reduction index (56% in SBP and 63% in DBP). The former result was obtained by including the extreme dippers category in the dippers group. To check whether there is any significant difference in both results it would have been worthwhile to study the percentile distribution of both results. According to Verdechchia P et al. the decline in the daytime BP level by more than 10% in defining dippers as opposed to non-dippers are practical (7). In the acquisition of this index, the additional group category known as extreme dippers has also been widely used to describe circadian BP patterns in many other research (15,16). This provides a useful baseline in describing patients who have marked nocturnal BP fall. In contrast, Staessen et al in a large international database study suggested that using the night-day ratio was more preferable for characterising dippers as opposed to non-dippers because the ratio depends less on BP level than on the nocturnal fall in BP (6). Although there is no right or wrong answer, for this study, the most practical way to demonstrate BP diurnal pattern is probably by using the night-day ratio since the size of the sample is insufficient to significantly demonstrate the presence of dippers, non-dippers and extreme dippers. Nevertheless, to resolved the confusion of this issue further studies are needed to standardise the definition of dipping and non-dipping. In highlighting the extreme dippers category, the corresponding percentage of patients categorised as extreme dippers was greater in females (20% for SBP; 30% for DBP) compared to males. Although they were grouped as extreme dippers, these patients would require strict BP examination regularly since extreme dippers have been postulated to have more marked effect in terms of having cerebrovascular damage than dippers and non-dippers (11,16). Nevertheless, there is yet no clear evidence influencing the dipper, non-dipper or extreme dipper status with gender. Although, numerous studies have been done in discovering the contributing factors leading to the affect of dipping and non-dipping phenomena, the exact mechanism that distinguishes the two remains uncertain. Furthermore in this study, linear regression analysis revealed a positive correlation between age and SBP variables. This is in keeping with the fact that in most cases BP tends to rise as we grow older. More precisely, in almost all populations, ageing is associated with a rise in systolic BP and fall in diastolic BP (17). This is due to the rigidity and loss of elasticity of large arteries due to ageing. Atherosclerosis further exaggerates the systolic peak in BP and the lack of elastic recoil in diastole reduces the diastolic pressure leading to an isolated systolic hypertension. It is now recognised that isolated systolic hypertension increases the risks of stroke and other medical conditions that treating high SBP in these patients is at least as beneficial as treating the younger patients with raised BP (18). Another result from the study exposed that night HR was found to be significantly related with night time systolic and diastolic BP. The relationship was stronger in night DBP than night SBP. Patients HR could have been affected by the disturbance made by the ambulatory cuff inflation and deflation during the measurements at night. In a study that analysed physical activity and its association with diurnal BP variations in asymptomatic adults who were neither normotensive nor mildly hypertensive, it was discovered that physical activity is one of the determinants of ambulatory BP and its diurnal variation (19). The study also found that physical activity is a predictor of HR and that sleep activity is also related to nocturnal BP dipping status. Therefore, it is interesting to know whether the patients studied did have a good sleep quality during the period of monitoring. It is not impossible if some patients studied had sleeping problems or perhaps sleep apnoea syndrome (20). The best way to identify this is to conduct sleep studies that can be assessed by polysomnography. Literature has suggested that BP variations may be associated with sleep quality, emotions as well as physical activity. One study made a report on the associations among depression, anxiety, awake physical activity, sleep quality and diurnal blood pressure variation in a non-psychiatric sample. It was found that depression is associated with abnormal diurnal pattern independent of physical activity in working men, whereas anxiety is associated with awake SBP and HR in women (21). In a different study that looked into the relationship of work stress and cardiovascular disease (22), the result showed night heart rate and vagal tone were independently associated with incidence of mild hypertension. This is consistent with the result of the present study that night HR correlates with night BP. Therefore by effective relaxation techniques, sleeping well at night and avoiding stress at work are among the things we can simply perform to possibly reduce the risk of hypertension and hence, cardiovascular disease. In conclusion, ABPM devices are beneficial in studies related to blood pressure measurements. The use of ABPM in hypertensives patients has facilitated doctors to decide the next plan of management. In the ABPM study conducted in AZIM, it has been demonstrated that the hypertensive patients were young and in general, they had good BP control. In addition, the study also illustrated that patients in general are dippers. Male and female patients showed no significant difference in the ABPM parameters. There were significant relationships between the patients' age and SBP and the patients' night HR with night BP. Although the sample size was small, this does not affect the results since clinical ABPM studies usually does not require big sample before it can be performed (23). REFERENCES
Copyright 2003 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj03026t3.jpg] [mj03026t1.jpg] [mj03026f1.jpg] [mj03026t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}