 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 10, No. 2, July 2003, pp. 87-90 ROTAVIRUS - A RETROSPECTIVE STUDY OF INCIDENCE AT THE HOSPITAL UNIVERSITI SAINS MALAYSIA (HUSM) C.M. Mat Ludin, J. Md.Radzi , and A.Maimunah Department of Microbiology and Parasitology, School
of Medical Sciences, Universiti Sains Malaysia, Health Campus, 16150 Kubang
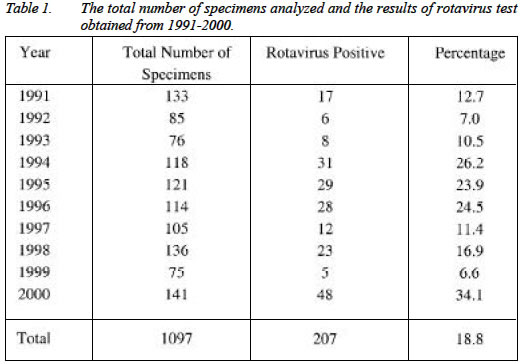
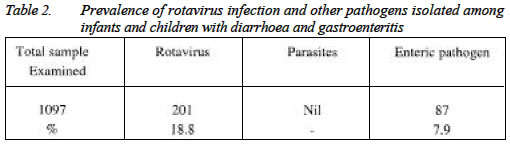
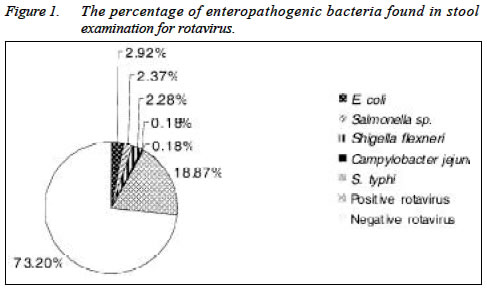
Kerian, Kelantan, Malaysia Submitted-22.12.2002, Code Number: mj03028 The present study, analyzes data from 1991 to 2000 for rotavirus infection among children with diarrhoea and acute gastroenteritis admitted to the Hospital Universiti Sains Malaysia (HUSM). The Latex Slide Agglutination Test was used for the detection of rotavirus antigens. Out of 1097 stool samples tested, 207 samples or 18.8 % were found to be positive for rotavirus. The infection occurred most frequently in infants and young children from 6 months to 2 years of age. The infection was recorded highest in the year of 2000 - 48 cases (34.1%) and the lowest in 1999 - 5 cases (6.6%). Stool examination and cultures from the rotavirus positive samples revealed no parasites and enteropathogenic bacteria. These observations suggested that rotavirus could still remain as an important agent causing diarrhoea and gastroenteritis in young children admitted to HUSM. Key words : Rotavirus, gastroenteritis, latex agglutination INTRODUCTION Rotavirus infection is a major cause of severe diarrhoea in infants and young children all over the world. Although, the infection is no longer a major cause of childhood death in Malaysia, it remains a major cause of morbidity in infants and young children. It is most severe in children between the ages of 6 months and 2 years. It is generally accepted that neonatal rotavirus infections are without symptoms. This is probably due to the presence of maternal antibody protection (5). Two viral surface proteins, P and G, are thought to be immunologically important since they induce type-specific neutralising antibodies. Many different variants have been described, but in Europe, Asia and the USA most strains belong to the genotype p (4) G2 or combinations of P (8) with G1, 3, or 4.1 (5). It is notable that many candidate rotavirus vaccines are based on the G1-4 strains. Rotavirus infection may be highly contagious. Children and adults can become infected on coming into direct contact with the virus that are in the feces of an infected child and then passing on those viruses to the mouth (fecal-oral transmission). Resistance to physical inactivation (along with the large number of viral particles shed in feces) may contribute to the efficient transmission of the human rotaviruses. However, the source of infection in infants and neonate - those not normally in contact with other infants and young children with gastroenteritis, is not well documented. It is most likely that infection is acquired from an older sibling or parents with sub clinical infection (2). The aim of this study is to estimate the prevalence of rotavirus gastroenteritis in HUSM and other pathogens associated with this infection. METHODOLOGY This is a retrospective analysis of all stool samples of children admitted to the HUSM over the last 10 years suspected of having rotavirus infection. In this study, the rotavirus was detected by examining the stool specimen using commercial kit "Serobact Rotavirus Latex Slide Agglutination Test" Medvet Science PTY LTD, Australia for the detection of rotavirus antigens. When a stool extract was mixed with the test latex reagent any rotavirus antigens present will react with the sensitizing antibodies, resulting in visible agglutination of the latex particles. In each test, positive and negative control samples were also included. The stool samples were also examined and cultured in an appropriate media such as MacConkey, DCA and CCDA for the present of enteropathogenic bacteria and parasites. RESULTS The total number of specimens analysed and the results of rotavirus test obtained for each year within a 10 years of period are shown in table 1. Out of the 1097 stool samples studied, 207 or 18.8% were found to be positive for rotavirus, 7.93% for enteric pathogen and negative for parasites as shown in table 2. The enteropathogenic bacteria isolated were Salmonella sp. (2.37%), Shigella flexneri (2.28%), Escherichia coli (3.92%), Campylobacter jejuni (0.18%) and Salmonella typhi (0.18%) as shown in pie chart in figure 1. Stool examination and cultures from the rotavirus positive revealed no parasites and enteropathogenic bacteria. All the patients with rotavirus positive were children aged under 2. The disease was prevalent in both sexes and in all races. The rotavirus infection among children with diarrhoea and gastroenteritis was recorded highest in the year 2000, (48 cases - 34.1%) and the lowest infection was recorded in 1999, (5 cases - 6.6%) as shown in table 1. DISCUSSION Rotavirus organism seems to be a virus of significance in infant and young children with diarrhoea and gastroenteritis in HUSM. Although only 18.8% of the children's with diarrhoea and gastroenteritis in our study shed rotavirus in their feces, nevertheless these findings support previous observations that the disease is prevalent in infant and young children (2). Other etiologic agents accounting for a relatively small number of episodes of gastroenteritis was the enteropathogenic bacteria such as Escherichia coli, Salmonella spp. Shigella spp. and parasites of Cryptosporidium spp. Recently, there was a report on outbreak of rotaviruses that caused neonatal diarrhoea in a paediatric ward in the Netherlands. The genotype P (6) G9 rotavirus was the cause of the outbreak (5). This high attack rate may, in part, be due to the lack of protective antibodies in a high proportion of neonates, since P (6) G9 rotaviruses have not been previously found in the Netherlands and therefore mothers may not have been exposed to this genotype. In this study, the genotyping of the rotavirus grouping was not performed. Stool examination and cultures from the rotavirus positive samples revealed no parasites or enteropathogenic bacteria, suggesting that rotavirus could remain as an important agent in the causation of severe diarrhoea in young children admitted to HUSM. The infection was reported to be more severe in children between 6 months and 2 years of age, whereas neonatal rotavirus infections were generally accepted as symptom less, suggesting that it is probably due to maternal antibody protection (5-6). Rotavirus infections display a consistent pattern throughout the year but with slightly higher incident in year 2000, where 48 cases or 34.1% had been reported. While a lower infections rate was recorded in 1999 where 5 cases or 6.6% of rotavirus positive were reported. However, no rotavirus outbreaks were reported during the 10 years period of studies. In temperate countries, it shows seasonal pattern of infection. Classically, an outbreak occurs during the winter months, especially at the day-care centre and children hospitals (4). Rotaviruses appear to be transmitted by the fecal-oral route. Children and adults can be infected via direct contact with the viruses that are in the feces of an infected child and then passing on those viruses to the mouth. Resistance to physical inactivation (along with the large number of viral particles shed in feces) may contribute to the efficient transmission of the human rotavirus. The source of infection for the young infant who is normally not in contact with other infants and young children with gastroenteritis is not well documented. Infection is most likely acquired from an older sibling or parent with sub clinical infection or from environmental contamination such as nosocomial infection in hospital and nurseries. There has been speculation on the role of animals as a source of rotavirus infection to human (3). Because certain animal rotavirus share a neutralizing antigen with human rotavirus and some natural occurring animal rotavirus strains may infect humans. Nonetheless, this types of interspecies infection appear to be a rare event. The ability of rotavirus to survive on various surfaces under different conditions may also contribute to the rapid spread of these agents. However, relatively high humidity (~ 80%) results in a rapid loss in human rotavirus infectivity. Therefore, the incidence of rotavirus infection in HUSM (18.8%) is relatively low compared to those seen in temperate countries such as in the UK (52%) and Finland (49%) (Cook et, al.,1990). Effective disinfections of contaminated material and careful hand washing constitute important measures to contain rotavirus infection, especially in hospital and other institutional settings. The clinical manifestations of rotavirus illness are not sufficiently distinctive to permit diagnosis on this basis alone. Therefore, diagnosis requires detection of virus or viral antigen and / or demonstration of a serologic response. The epidemiologic pattern may provide additional information to aid in diagnosis, but laboratory confirmation is required. Various methods are available for the detection of rotavirus in stool specimens. The method of choice is the Latex Slide Agglutination Test since it is highly sensitive, specific, does not require specialized equipment and has a built-in control for non-specific reaction. Conclusion Although the incidence of rotavirus infection in HUSM is relatively low as compared to that of temperate countries, the viruses remain as an important agent in the causation of gastroenteritis and diarrhoea. Illness is most severe in children between 6 months and 2 years of age, whereas neonatal rotavirus infections are generally symptomless because of maternal antibody protection. It show seasonal pattern of infection in the temperate countries but not in a tropical setting. The Latex Slide Agglutination Test (commercial kit) is the method of choice for the detection of rotavirus antigen in fecal specimens because it is rapid, highly sensitive, specific and more convenient compared to ELISA and electron microscopy. The enteropathogenic bacteria is not frequently isolated in gastroenteritis associated with rotavirus infection. There are also cases showing concomitant infection by enteropathogenic bacteria in rotavirus gasteroenteritis, but these rarely occurred. REFERENCES
Copyright 2003 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj03028t1.jpg] [mj03028f1.jpg] [mj03028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}