 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
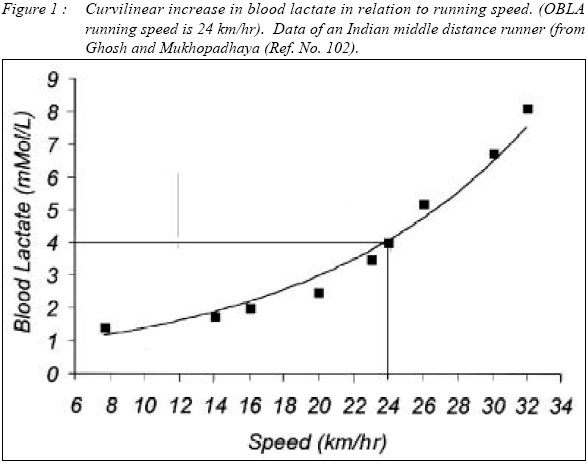
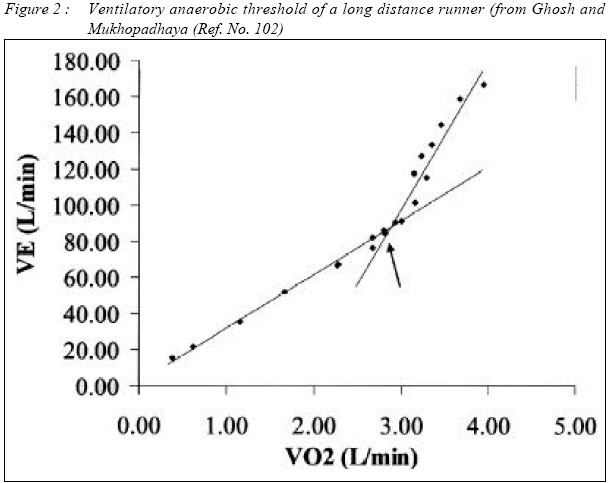
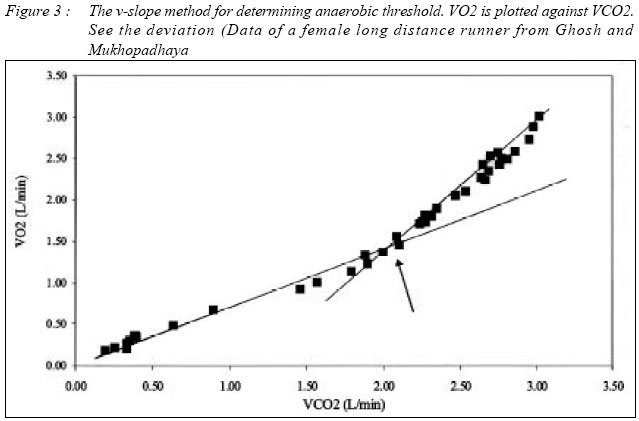
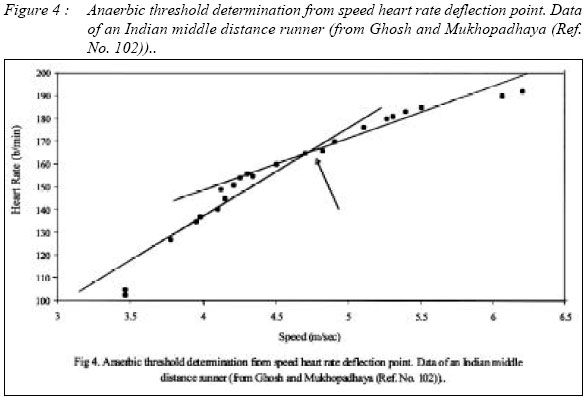
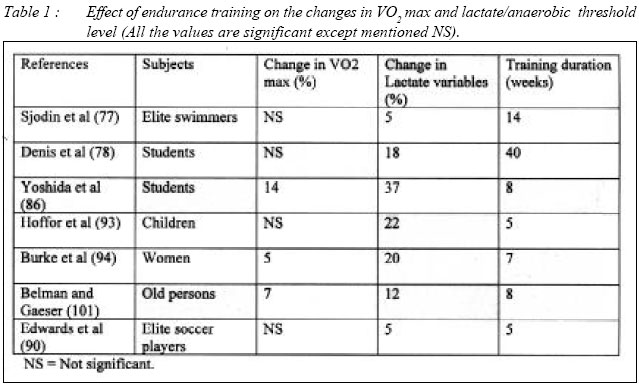
Malaysian Journal of Medical Sciences, Vol. 11, No. 1, January 2004, pp. 24-36 REVIEW ARTICLE Anaerobic Threshold: Its Concept and Role in Endurance Sport Asok Kumar Ghosh Sports Science Unit, School of Medical Sciences, Universiti Sains Malaysia 16150 Kubang Kerian, Kelantan, Malaysia Correspondence : Assoc. Prof. Dr. Asok Kumar Ghosh, BSc. (Hons), M.Sc., PhD. Sports Science Unit, School of Medical Sciences, Universiti Sains Malaysia, health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Code Number: mj04003 aerobic to anaerobic transition intensity is one of the most significant physiological variable in endurance sports. Scientists have explained the term in various ways, like, Lactate Threshold, Ventilatory Anaerobic Threshold, Onset of Blood Lactate Accumulation, Onset of Plasma Lactate Accumulation, Heart Rate Deflection Point and Maximum Lactate Steady State. But all of these have great role both in monitoring training schedule and in determining sports performance. Individuals endowed with the possibility to obtain a high oxygen uptake need to complement with rigorous training program in order to achieve maximal performance. If they engage in endurance events, they must also develop the ability to sustain a high fractional utilization of their maximal oxygen uptake (%VO2 max) and become physiologically efficient in performing their activity. Anaerobic threshold is highly correlated to the distance running performance as compared to maximum aerobic capacity or VO2max, because sustaining a high fractional utilization of the VO2max for a long time delays the metabolic acidosis. Training at or little above the anaerobic threshold intensity improves both the aerobic capacity and anaerobic threshold level. Anaerobic Threshold can also be determined from the speed-heart rate relationship in the field situation, without undergoing sophisticated laboratory techniques. However, controversies also exist among scientists regarding its role in high performance sports. Key words : Anaerobic, Lactate, Heart Rate, Deflection Point, Ventilatory, Threshold, Acumulation. Introduction Recent decades have witnessed a remarkable expansion of the application of scientific principles to sports and exercise. Application of science to sports are especially evident in the field of physiology; indeed sports practitioners are quick to realize the importance of acquiring basic physiological knowledge that can produce better effect. Exercise physiology has for many years been a respected field in its own right. Exercise has conventionally been used as a medium for perturbing physiological systems to ascertain how they behaved under stress. Exercise physiologists have further established the ceilings in human physiological responses and the factors that limit performances in various conditions. Physical performance in various competitive sports events depends largely on the integrated status of the different physiological mechanisms of the individual i.e. the state of health and capacity for physiological responses to meet the challenges of the competitive situation, apart from the technique, tactics and skill. Optimum level of performance depends on the development of these responses through training. Therefore, the main purpose of physiological research is to evaluate and monitor the training schedule effectively. The most important physiological factor for high performance in marathon is to possess a high aerobic capacity or VO2 max. An elite marathoner exhibits a high VO2 max (more than 80 ml/kg/min), similarly the VO2 max is an important parameter of middle and long distance runners, road cyclists, long distance swimmers (70-80 ml/kg/min) and team game players (60-70 ml/kg/min), whereas, the sprinters exhibits a comparatively lower VO2 max (45-55 ml/kg/min) [1]. In long term endurance events, oxidative phosphorylation plays the dominant role and thus the maximum oxygen uptake (VO2 max) or aerobic capacity becomes one of the major determining factors in high performance sports. VO2 max is restricted to only the individuals' cardiorespiratory capacity relating the O2 uptake, transport and utilization. Not only in marathon but also in all other sports events of long duration activity, whether it is a continuous type or non-continuous type, VO2 max plays the key role. Maximal oxygen intake may be the most physiologically significant and most commonly measured parameter in the physiological assessment of well-trained athletes. For this reason a linear correlation has been observed by various exercise physiologist between VO2 max and distance running performance, where the correlation coefficient varies from 0.52 to 0.98 (2-11). A high aerobic power (VO2 max) is an advantage in endurance sports, but to sustain a high fraction of VO2 max for a long time is more important (6-8). Anaerobic Threshold Concept Individuals endowed with the possibility to obtain a high oxygen uptake need to complement with rigorous training program in order to achieve maximal performance. If they engage in endurance events they must also develop the ability to sustain a high fractional utilization of their maximal oxygen uptake (%VO2 max) and become physiologically efficient in performing their activity (6, 8, 12). This hypothesis is the concept of anaerobic threshold or lactate threshold or aerobic to anaerobic transition point. During exercise of increasing intensity there is a rise of blood lactate concentration and this response was first reported half a century ago (13-14). Concept of anaerobic threshold/lactate threshold was introduced in order to define the point when metabolic acidosis and also the associated changes in gas exchange in the lungs, occur during exercise (15). To explain it in another way, during incremental exercise, at a certain intensity, there is nonlinear steep increase in ventilation, known as ventilatory anaerobic threshold (16), a non linear increase in blood lactate concentration, known as lactate threshold (16), a non linear increase in CO2 production, an increase in end tidal oxygen, an increase in CO2 production (15), an arterial lactate level of 4 mM/L, known as onset of blood lactate accumulation (OBLA) [17], and an abrupt increase of FEO2 (expired O2 fraction) [18]. All these points are collectively labeled as Anaerobic Threshold (AT). It is evidenced that ventilatory anaerobic threshold is directly related to and also caused by blood lactate threshold (15-19). It has been observed that individuals with similar VO2 max have variability in endurance capacity and that highly trained athletes perform at a high percentage of their VO2 max with minimum lactate accumulation (20-21). Furthermore, trained athletes accumulate less lactate than untrained athletes at a given submaximal workload. This concept has prompted the consideration of anaerobic threshold as a determinant of physiological fitness. While the appearance of lactate in blood during exercise is the result of an increased glycogenolysis, it is important to recognize that its concentration is, at any time, the result of a balance between the rate of production and removal (22). Nevertheless, during exercise of increasing intensity, the rise in blood lactate concentration is an indication of increase in glycogen metabolism. This increase in blood lactate has been interpreted as a reflection of the onset of hypoxia in skeletal muscles and the exercise intensity at which anaerobic metabolism complements the regeneration of ATP by aerobic metabolism has been called the Anaerobic Threshold (22). Lactate Threshold Concept Different scientists with the same objective to determine the aerobic and anaerobic transition point, of an exercising individual, adopt different methodologies. Production of lactate in the muscle increase curvilinearly with increasing work load (23-24) or with percentage utilization of VO2 max. The level at which abrupt increase in blood lactate is observed has been described as individual's lactate threshold (Fig 1). Numerous scientists emphasized that blood lactate concentration is the net result of lactate production or appearance in the muscle and its removal from the muscle (25-28). Thus the rise in blood lactate may not necessarily indicate the abrupt increase in lactate production by the exercising muscle, due to simultaneous removal process. Increased lactate production could have occurred much earlier but may not have increased the blood lactate concentration because of increased removal. It is well known that non-exercising muscle, the liver, the kidney and the heart can mobilize lactate (29-32), from the main stream for further biochemical degradation. Some reports (33, 34) however indicate that during the work rate below 50-60% of maximum oxygen uptake, muscle lactate does not increase, since the appearance and disappearance rate of lactate becomes almost equal. This supports the fact that initial increase in blood lactate concentration reflects that appearance rate of lactate in the blood is higher than the disappearance rate. Many investigators have suggested that together with lactate, hydrogen ions are generated (15, 35, 36). Due to its low pK (3.9) lactic acid is presumed to dissociate after its formation, thereby generating hydrogen ion (15, 36). The hydrogen ion thus produced may elevate CO2 through carbonic acid bicarbonate buffer system and alter homeostasis (15, 22, 35, 38). Ventilatory Anaerobic Threshold Wassermann and Mcllory (37) and Reybrouck et al (38) postulated that alveolar ventilation is coupled to CO2 flow to the lungs, thus leading to maintain arterial isocapnia during moderate exercise. However, as the intensity of exercise increases hydrogen ion released from lactic acid can no longer be buffered by blood bicarbonate stores and thus metabolic acidosis results. This increase in hydrogen ion further stimulate ventilation by stimulating central as well as peripheral chemoreceptors resulting in further increase in ventilation. Thus the linearity of ventilation with changes of work load and oxygen utilization deviates at certain points which is named as ventilatory anaerobic threshold (Fig 2). In other words, during incremental, non-steady state exercise, a point is reached at which a subject's ventilation shows a non-linear increase and this is termed as ventilatory threshold. Ventilatory threshold is coincident with its hypothesized causative factor, a non-linear increase in blood lactate concentration termed as the lactate threshold (39). Several ventilatory parameters have since been utilised in assessing ventilatory threshold, among which are oxygen consumption (VO2) [40-42], pulmonary ventilation (VE) [18, 42-44], respiratory exchange ratio (RER) [18, 45], excretion of CO2 (VCO2) [19, 43], and the ratio of ventilation to oxygen consumption (VE / VO2) [46, 47] have been devised to evaluate this critical intensity. Most techniques rely on visual inspection of one or two specific parameters over time and / or velocity to identify the breakaway threshold. Methods have now been devised over tine and/or velocity to identify the breakaway threshold. Beaver et al (19) utilised a computerised regression analysis of the VCO2 versus VO2 slope (Fig 3) collected during progressive intensity exercise (V-slope method). Although no significant difference existed between the VO2 at ventilatory threshold computed by the V-slope method and visual inspection. The V-slope method could more reliably determine ventilatory threshold. Orr et al (48) performed a computerised 3-segment regression analysis to locate the intersection point of the segments in the VE vs. VO2 plot. Their computerised method also correlated highly (r = 0.95) with visual inspection methods with a difference of 0.05 L / min between VO2 at AT determined by computer and by visual inspection. The ability of gas exchange variables to detect the onset of lactic acidosis was investigated by Hollman (16) and Wassermann and Mcllory (37). Since this time, numerous studies have investigated the ability of specific respiratory measures in assessing the degree of anaerobiosis. Davis et al (18) investigated the validity of AT detection through nonlinear increase in VE and VCO2 and abrupt increase in the fractional concentration of O2 (FEO2). No significant difference was observed between the estimation of AT from these gas exchange variables and blood lactate concentration. On average, AT occurred at 59.8 + 7.4% VO2 max and 59.7 + 7.1 % VO2 max for respiratory gas exchange and blood lactate methods, respectively. Furthermore, a correlation of 0.95 was observed after plotting %VO2 max scores for gas exchange AT versus blood lactate AT methods. Caiozzo et al (49) also examined the correlation between gas exchange and blood lactate methods for determination of AT. Comparisons were made for using nonlinear increase in VE or VCO2 , an abrupt increase in respiratory exchange ratio (RER), an increase in VE / VO2 without a concomitant increase in VE / VCO2 and the systematic increase in blood lactate concentration. All gas exchange methods except RER significantly correlated with blood lactate method in ability to detect the AT. Similar methods have been produced by Reinhard et al (50) who observed a significant correlation between the VO2 at lactate threshold and the VO2 at ventilatory threshold, as determined through the ventilatory equivalent for oxygen. In describing the differencesof muscle fiber type and the occurrence of both lactate and ventilatory threshold, Aunola and Rusko (51) found no significant difference in the occurrence between lactate threshold and ventilatory threshold when expressed in terms of %VO2 max. Several lines of evidence have recently been presented which refute the theory that ventilatory and lactate threshold are casually linked. Most studies examining this theory compare the ventilatory response during exercise in individuals with normal and elevated blood lactate concentrations. These studies suggest that the elevated blood lactate concentrations had no significant effect on ventilation during the progressive intensity exercise. Neary et al. (52) examined lactate and ventilatory thresholds under normal conditions and under glycogen depleted and / or previously exercised states. No significant changes in ventilatory threshold resulted under experimental conditions, therefore suggesting that plasma lactate accumulation was not responsible for the threshold-like responses in ventilation. Cecca et al (53) performed a similar investigation where subjects performed incremental exercise under normal and acidic conditions. Although subjects began the experimental progressive intensity exercise with a mean blood lactate concentration of 9.8 mM/L, ventilation did not significantly differ at each power output from normal conditions. Again, the elevated blood lactate concentration did not alter the pattern of ventilation during the progressive intensity test. Heart Rate Deflection Point and Anaerobic Threshold The heart rate deflection point (HRDP) is a deviation point at the linear relationship between heart rate and work load is evinced during progressive incremental exercise testing (Fig 4). The HRDP is reported to be coincident with the anaerobic threshold. In 1982, Conconi and colleagues suggested that this phenomenon could be used as a noninvasive method to assess the anaerobic threshold (54). These researchers developed a field test to assess the HRDP, which has become popularised as the `Conconi test'. Concepts used to define and assess the anaerobic threshold as well as methodological procedures used to determine the HRDP are diverse in the literature and have contributed to controversy surrounding the HRDP concept (55). Although the HRDP may be assessed in either field or laboratory settings, the degree of HR deflection is highly dependent upon the type of protocol used. The validity of HRDP to assess the anaerobic threshold is uncertain, although a high degree of relationship exists between HRDP and the second lactate turnpoint (lactate threshold). Conconi et al. (54) reported a noninvasive field test for anaerobic threshold (AT) based upon an observed deviation from the linear heart rate (HR)—running velocity (RV) relationship at high RV (HR deviation). While the validity of the Conconi test has been debated (56, 57), the reliability of the Conconi test has never been independently assessed in athletes performing the protocol outlined by Conconi. In a study by Jones and Doust (58), the reliability of the Conconi test in 15 well-trained male distance runners was evaluated twice within a 4-8 day period. The results indicated that 6 subjects demonstrated HR deviation in both Conconi tests, 5 subjects demonstrated HR deviation in only one test, and in 4 subjects' deviation could not be demonstrated in either test. They concluded that failure to determine a reproducible HR deviation by subjective assessment in 9 of 15 subjects makes the Conconi test unsuitable for reliable evaluation of AT. Vachon et al (59) designed 4 test protocols, like, 1) a treadmill test for maximal O2 uptake, 2) a Conconi test on a 400-m track with speeds increasing approximately 0.5 km/h every 200 m, 3) a continuous treadmill run with speeds increasing 0.5 km/h every minute, and 4) a continuous LT treadmill test in which 3-min stages were used, to see whether the HR deflection point accurately predicts lactate threshold (LT). In this study, all subjects demonstrated HR deflection on the track, but only one-half of the subjects showed HR deflection on the treadmill. The researchers concluded that the HR deflection point was not an accurate predictor of LT. Petit et al (60) examined the relationship between ventilatory threshold (Tvent) determined from a laboratory test and heart rate deflection (HRd) from the Conconi test, to validate a mathematical model (MM) that evaluates the Conconi test and predicts 10-km race time. These researchers found a significant relationships between velocity at Tvent and HRd (r = .95, p < .01), and predicted times from each method (r = .96, p < .01). Hoffman et al (61) investigated 227 young subjects, using the method of Conconi et al. (54) and observed 85.9% of the subjects showed a "regular" deflection, 6.2% showed no deflection at all, and 7.9% showed even an inverted deflection of the heart rate performance curve (HRPC). Among all the endurance athletes, the Conconi test was observed not to be very relevant for determining anaerobic threshold of rowers (62). Ballazin et al (63) observed that the speed and heart rate of deflection values assigned visually by observers were compared to the values obtained through mathematical analysis of the tests by computer. Straight-line equations, correlation coefficients (r), and technical errors of measurement (TEM) obtained by comparing visually determined data to those determined through mathematical analysis were calculated for each observer. Differences were found between the observer-assigned and computer-determined results for both speed and heart rate of deflection. The study highlighted that visual analysis provides information that is very similar to that obtained through computer analysis and the accuracy of the visually obtained information varies according to the observer's experience. Endurance Performance and Anaerobic Threshold In the exercising human, maximal oxygen uptake (VO2max) is limited by the ability of the cardiorespiratory system to deliver oxygen to the exercising muscles. This is shown by three major lines of evidence: 1) when oxygen delivery is altered (by blood doping, hypoxia, or beta-blockade), VO2 max changes accordingly; 2) the increase in VO2 max with training results primarily from an increase in maximal cardiac output (not an increase in the a-v O2 difference); and 3) when a small muscle mass is overperfused during exercise, it has an extremely high capacity for consuming oxygen. Thus, O2 delivery, not skeletal muscle O2 extraction, is viewed as the primary limiting factor for VO2max in exercising humans. Metabolic adaptations in skeletal muscle are, however, critical for improving submaximal endurance performance. Endurance training causes an increase in mitochondrial enzyme activities, which improves performance by enhancing fat oxidation and decreasing lactic acid accumulation at a given VO2. VO2max is an important variable that sets the upper limit for endurance performance (an athlete cannot operate above 100% VO2max, for extended periods). Running economy and fractional utilization of VO2max also affect endurance performance. The speed at lactate threshold (LT) integrates all three of these variables and is the best physiological predictor of distance running performance (64). Several attempts have been made to predict endurance ability of the athletes, particularly in continuous events like long distance running. Farrell et al (65) reviewed that the anaerobic threshold yielded highest correlation (r = 0.98) with marathon running performance. Kumagai et al (66) observed a higher correlation between 5000 and 10,000 meters running performance and lactate threshold (r = 0.95 and 0.84) than between running performances with the VO2 max (r = 0.65 and 0.67). Sjodin and Jacob (67); Karlsson and Jacob (68) related 4mM/L (OBLA) lactate to endurance performance and reported a high correlation between them (r = 0.96). It is very much evident from the earlier observation that in elite runners, the onset of blood lactate accumulation (OBLA) occurred at a higher running speed (65, 69, 70). Besides continuous events, the importance of anaerobic threshold in non-continuous intermittent games has also been discussed (40, 71, 72). Yoshida et al (73) observed the relationships between running velocity (v) in a 3000-m race and various physiological parameters. The parameters measured among 57 female distance runners during a treadmill running test were v at the lactate threshold (v-Tlac), oxygen uptake (VO2) at the lactate threshold (VO2 at Tlac), v at the onset of blood lactate accumulation (v-OBLA), VO2 at OBLA, running economy (steady-state VO2 at a standard v of 4 m s-1), maximal oxygen uptake (VO2 max) and v at VO2 max (v-VO2 max). The v-OBLA revealed highest correlation with v over 3000-m race (r = 0.78, P < 0.001), followed by the same with v-Tlac (r = 0.77, P < 0.001). Although v-VO2 max was strongly correlated with v over 3000 m (r = 0.75, P < 0.001), further analysis by stepwise multiple regression indicated that a combination of v-OBLA, VO2 at Tlac and v-Tlac could account for 73.2% of the variability in v over 3000 m, whereas v-OBLA on its own explained only 61.5%. Blood lactate variables can account for a reasonably large part of the variance in v over 3000 m. Even, v-VO2 max can be used as a non-invasive predictor of distance running performance. LT appears consistent with the ventilatory threshold (VT) described by the V slope method (19). Hence, LT and VT may be independent of each other, but there is a link between ventilatory changes and cellular events. It may be suggested that any point consistently used from the lactate concentration curve during exercise may be used as a performance index (56) in long duration continuous events. Training and Anaerobic Threshold Training also has different effects on blood lactate concentration and ventilatory threshold. Three weeks of cycling endurance training reduces blood lactate concentration without affecting the ventilatory threshold (74). The type of training programme also affects the dissociation between blood lactate threshold and ventilatory threshold. Interval training can increase the time to both blood lactate threshold and ventilatory threshold, but endurance training can delay the onset of venous blood lactate threshold, showing less effect on ventilatory threshold. In fact, there was not a significant correlation (r = 0.13) in the time of onset of the two variables between any of the above different training protocols (75). Simon et al (76) demonstrated that in sedentary males, ventilatory threshold (51% of VO2 max) occurred significantly before blood lactate threshold (62% VO2 max), whereas, in trained males the onset of ventilatory threshold (66% VO2 max) was not different from blood lactate threshold (69% of VO2 max). Furthermore, Denis et al, (78) investigated the effect of a 40 week endurance training programme on ventilatory and lactate thresholds and lactate threshold at 4 mM/L. In comparing the changes over the 40 week period, the threshold level changes by 10, 15 and 18% respectively. All correlations between the 3 threshold intensities over the 40 week period show significance with a ventilatory and lactate threshold correlation of r = 0.79 (p<0.001) [Table 1]. This gives further evidence that the threshold prescribed by ventilatory parameters (departure from linearity in VE ) and lactate measures (onset of and abrupt increase in blood lactate) are associated and causally linked. In long term high intensity exercise the concentration of muscle glycogen may be a limiting factor (79, 80). Exercise just below the AT will result in a much slower depletion of muscle glycogen reserves than exercise above AT level and would therefore be tolerable for much longer period of time. On the other hand, Boyd et al (81) demonstrated that elevation in blood lactate concentration inhibits lipolysis in exercising man and thus force obligatory carbohydrate utilization. This indicate that the training at AT level is suitable for endurance athletes. Training at or near anaerobic threshold level result in change in muscle ultrastructure (82), capilarization (83), oxidative capacity (84) and substrate utilization (85). The benefit which results from the physiological adaptations to anaerobic training include decrease in O2 cost for ventilation, the lactate accumulation and depletion of glycogen at a given power output. The end result is the rise in the intensity of efforts that can be sustained aerobically. In endurance sports, it has been suggested that AT might be a better indicator of aerobic endurance than VO2 max, as AT may change without changes in VO2 max (87, 88). Several studies have demonstrated that in the general population, aerobic training often improves the exercise intensity corresponding to anaerobic threshold without a concomitant increase in VO2max (88, 89). In team events, like soccer, training at lactate threshold (LT) and ventilatory anaerobic threshold (VT) improved the anaerobic threshold level, while the VO2max remained unchanged (90). VO2 at LT as well as at VT was also improved. There was no significant difference in VO2max. VO2max is a less sensitive indicator to changes in training status in professional soccer players than either LT or VT (90). OBLA has been widely used to identify changes in training state, however, it's use has been criticised due to variability between subjects (91) and also because it may be a result of not only muscle anaerobisis, but also a decreased total lactate clearance or increased lactate production in specific muscles (92). VO2max may provide a useful indicator of the aerobic capacity of the athlete, but it's use is limited in the ongoing process of monitoring changes in training state. Submaximal LT or VT may identify changes in aerobic conditioning. The effects of the of five week interval training on metabolic parameters at maximal work and at the anaerobic threshold in 11 year old children have been studied, using interval work at 25 and 50% above the anaerobic threshold (93). Following training, the children increased their anaerobic threshold (expressed as %VO2max) significantly (P < 0.05), by 22%, while oxygen uptake (VO2, l/min) was increased by 19%, but the difference was not significant (P greater than 0.05). Burke et al (94) observed that a 7 week high intensity aerobic interval-training programme (at 80%, 90% and 95% VO2max) can produce significant changes in VO2max, lactate threshold and ventilatory anaerobic threshold and these changes appear to be independent of the length of the work interval. Training at 80% VO2max for 9 weeks duration can increase the anaerobic threshold level significantly. Even a similar duration of detraining can deteriorate the same (95). Training at little above anaerobic threshold level is more effective in improving the lactate threshold VO2 than training at anaerobic threshold level (96). Interval training involves repeated short to long bouts of high intensity exercise (at or little above lactate threshold intensity) combined with active or passive recovery periods. Interval training was first described by Reindell and Roskamm and was popularised in the 1950s by the Olympic champion, Emil Zatopek (97). The most important aspect is to assess the velocity or running speed at this lactate threshold level, rather than the VO2 at LT. The middle and long distance runners often use this technique to train at velocities close to their own specific competition velocity. In fact, trainers have used specific velocities from 800 to 5000m to calibrate interval training without taking into account physiological markers (97). However, in off season training camps, it is better to refer to the velocities associated with particular physiological responses in the range from lactate threshold to the absolute maximal velocity. The range of velocities used in a race must be taken into consideration, since even world records are also not run at a constant pace. It is better for a middle or long distance runner to possess a high VO2max, but the velocity of running at VO2max (v-VO2 max) is the first criterion (98, 99), while velocity at lactate threshold can also not be underestimated (100). Conclusions The present review has highlighted the importance and role of anaerobic threshold in endurance sports. Physiological terms like, individual anaerobic threshold, lactate threshold, ventilatory anaerobic threshold, heart rate deflection point, onset of plasma lactate accumulation, onset of blood lactate accumulation, maximum lactate steady state, denote the aerobic to anaerobic transition level, where lactate appearance in the blood from muscle is equal to the disappearance rate of lactate from the blood. This intensity is highly correlated with distance running performance and even training at or a little above this intensity is effective in improvement of anaerobic threshold not only in elite athletes, but also in sedentary population. Above this intensity, the appearance rate of lactate from the muscle to the blood exceeds the disappearance rate of lactate from the blood to the muscle. Both the continuous and interval type of physical training at anaerobic threshold intensity have beneficial effect on improvement of not only VO2 max but also on the anaerobic threshold level. A field method of assessing the anaerobic threshold is available and can be done from heart rate deflection point in speed-heart rate relationship with accuracy either by visual method or by computer programming. References 1. Saltin,B. and Astrand, P.O. Maximal oxygen uptake in ahletes. J. Appl. Physil., 1967; 23: 353-358. 2. Astrand, P.O. and Saltin, B. Maximal oxygen uptake and heart rate in various types of muscular activity. J. Appl. Physiol. 1961; 16: 977-981. 3. Costill, D.L.: The relationship between selected physiological variables and distance running performance, J.Sports Med. Phys. Fit. 1967; 7: 61-66. 4. Cooper, K. H.: Correlation between field and treadmill testing as a means for assessing maximal oxygen intake. J.A.M.A. 1968; 203: 135-138. 5. Doolittle, T. L. and Bigbee, R. The twelve min. run walk: a test of cardiovascular fitness of adolescent boys. Res. Q. Exerc.Sport. 1968; 39: 491-495. 6. Costill, D.L., Thomasos, H., and Roberts, E. Fractional utilization of the aerobic capacity during distance running. Med. Sci. Sports. 1973; 5(4): 248-252. 7. Daniels, J.T., Yarbrough, R.A. and Foster, C. Changes in VO2 max and running performance with training. Eur J Appl Physiol, 1978; 39: 249-252. 8. Conley, D.L.and Krahenbuhl, G.S. Running economy and distance running performance of highly trained athletes. Med.Sci.Sports Exerc. 1980; 12: 357-360. 9. Sjodin, B. and Svedenhah, J. Applied physiology of marathon running. Sports Med., 1985; 2: 83-87. 10. Londeree, B.R. Use of laboratory test results with long distance runners. Sports Med. 1986; 3: 201-203. 11. Ghosh, A. K., Ahuja A. and Khanna G. L.. Distance run as a predictor of aerobic endurance (VO2 max) of sportsmen - Ind. J. Med.Res. 1987; 86: 680-684. 12. Hagberg, J. & Coyle, E.F. Physiological determinants of endurance performance as studied in competitive racewalkers. Med. & Sci. Sports Exer. 1983; 15: 287 - 289. 13. Owles, W.H. Alterations in the lactate content of blood as a result of light exercise and associated changes in the CO2 combining power of the blood and the alveolar CO2 pressure. J. Physiol, 1930; 69: 214-237. 14. Bang, O. The lactate content of blood during and after muscular exercise in man. Scand. Arch. Physiol. 1936; 74: 51-82. 15. Wassermann, K., Whipp, B.J., Koyal, S.N., and Beaver, W.L. Anaerobic threshold and respiratory gas exchange during exercise, J. Appl. Physiol. 1973, 35: 236-239. 16. Hollman, W. The relationship between pH, lactic acid, potassium in arterial blood and venous blood, (PoW) and pulse frequency during increasing spirometric work in endurance-trained and untrained persons. Pan-American Congress for Sports Medicine, Chicago, 1959. 17. Yoshida, T., Chida M, Ichioka M, Suda Y. Blood lactate parameters related to aerobic capacity and endurance performance. Eur.J.Appl.Physiol., 1987; 7-11. 18. Davis, J.A., Vodak, P., Wilmore, J., Vodak, J., Kurtz, P.: Anaerobic threshold and maximal aerobic power for three modes of exercise. J. Appl. Physiol. 1976; 41: 544-550. 19. Beaver, W.L., Wassermann, K., Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl.Physiol. 1986; 60: 2020-2027. 20. Withers, R.T., Sherman,W.M. and Miller,J.M. Specificity of the anaerobic threshold in endurance trained cyclists and runners. Eur. J. Appl. Physiol. Vol 1981; 47: 93-104. 21. Tanaka, K., Matsura, Y., Matsuzaka, A., Hirakoba, K. and Kumagai, S. A longitudinal assessment of anaerobic threshold and distance running performance. Med. Sci. Sports Exerc. 1984; 16: 278-281. 22. Brooks, G.A.: The lactate shuttle during exercise, evidence and possible control. In: Sports Science, J.Watkins, T.Reilly and L. Burwits, Eds., E and FN Spon Ltd, London, 1986; 69. 23. Wassermann, K., Whipp, B.J., and Davis, J. Respiratory physiology of exercise : metabolism, gas exchange and ventilatory control, In MTP International Review of Physiology- Respiratory Physiology lll, Vol 23, Widdicombe, Ed., Baltimore University Park, Baltimore, 1981; 149. 24. Karlsson, J. and Jacobs, I. Onset of blood lactate accumulation during muscular exercise as a theoretical concept. Int.J. Sports Med., 1982; 3: 190-193. 25. Holloszy, J.O.: Biochemical adaptations to exercise: aerobic metabolism. In Wilmore (Ed), Exerc. Sports Sci. Rev. New York, Academic Press, 1973; 1: 45-72. 26. Donovan, C.M. and Brooks, G.A. Endurance training affects lactate clearance, not lactate production. Am. J. Physiol. 1983; 244: E83-E92. 27. Green, H.J., Hughson, R.L., Orr, G.W., Ranney, D.A.: Anaerobic threshold, blood lactate and muscle metabolism in progressive exercise. J.Appl. Physiol. 1983; 54: 1032- 1038. 28. Chirtel, S.J., Barbee, R.W. and Stainsby, W.N. Net O2, CO2, lactate and acid exchanges by muscle during progressive working concentrations, J.Appl.Physiol, 1984, 56: 161-165. 29. Essen, B., Pernow, B,, Gollnick, P.D. and Saltin, B. Muscle glycogen content and lactate uptake in exercising muscles, In: Metabolic adaptations to prolonged physical exercise, H. Howald and J.R. Poortmans, Eds. Basel, Birkhauser, 1975; 130. 30. Wahren, J., Hagenfeld, L. and Felig, P. Glucose and free fatty acid utilization in exercise. studies in normal and diabetic man, Isr. J. Med. Sci. 1975; 11: 551-554. 31. Yudkin, J. and Cohen, R.D. The contribution of a kidney to the removal of a lactic acid load under normal and acidotic conditions in the conscious state. Clin. Sci. Mol. Biol. 1975; 48: 121-124. 32. Welch, H. G.: Substrate utilization in muscle adaptation to physical effort . In : Exercise testing and exercise training in coronary heart decease, J.P. Naughton and H.K. Hellerstein, Eds., New york, Academic Press, 1973; 193. 33. Knuttgen, H.G. and Saltin, B. Muscle metabolites and oxygen uptake in short term sub-maximal exercise in man, J. Appl. Physiol. 1972; 32: 690-695. 34. Jorfeldt, L.A., Juhein-Dannfeldt, and Karlsson, J. Lactate release in relation to tissue lactate in human skeletal muscles during exercise. J. Appl. Physiol. 1978; 44: 350-355. 35. Whipp, B.J., and Mahler, M. Dynamics of pulmonary gas exchange during exercise. In: Pulmonary gas exchange, J.B., West (Ed), New York, Academic press, vol. ll, 1980; 33. 36. Davis, J.A.: Anaerobic threshold: review of the concept and directions for future research. Med. Sci. Sports and Exer. 1985; 17: 6-12. 37. Wassermann, K., Mcllory, M.B. Detecting the threshold of anaerobic mechanism in cardiac patients during exercise. Am. J. Card. 1964; 14: 844-859. 38. Reybrouck, T., Weymans, M., Stijns, H., Knops, K., van der Hauwaert, L. Ventilatory anaerobic threshold in healthy children. Eur. J. Appl. Physiol. 1985; 54: 278-284. 39. Walsh, M.L., Banister, E.W.: Possible mechanisms of anaerobic threshold : A review. Sports Med., 1988; 5: 269-302. 40. Bunc, V., Heller, J., Leso, J., Sprynarova, S., Zdanowicz, R. Ventilatory threshold in various groups of highly trained athletes. Int. J. Sports Med., 1987; 8: 275-280. 41. Ghosh, A.K., Ahuja, A., Khanna, G.L. and Puri,T.P.S.: Physiological variables of Indian national badminton players at anaerobic threshold level. World Badminton. 1987, 154: 10. 42. Haverty, M., Kenney, W.L., Hodgson, J.L. Lactate and gas exchange responses to incremental and steady state running. Br.J. Sports Med. 1988; 22: 51-54. 43. Rusko, H., Rahkila, P., Karvinen, E. Anaerobic threshold, skeletal muscles enzymes and fiber composition in young female cross country skiers. Acta Psychiatrica Scand. 1980; 108: 263-168. 44. Ghosh A. K., Mazumdar P., Goswami A. and Khanna G. L. Aerobic-anaerobic transition level of Indian middle and long distance runners. Ind. J. Med. Res. 1988; 88: 371-375. 45. Wassermann, K., Whipp, B.J. Exercise physiology in health and disease. Am. Rev. Resp. Dis. 1975; 112: 219-249. 46. Davies, C.T.M. and Thompson, N.W. Aerobic performance of female marathon and male ultramarathon athletes. Euro. J. Appl. Physiol. 1979; 41: 223-226. 47. Wassermann, K., Whipp, B.J., and Davis, J. Respiratory physiology of exercise : metabolism, gas exchange and ventilatory control, In MTP International Review of Physiology- Respiratory Physiology lll, Vol 23: Widdicombe(Ed), Baltimore University Park, Baltimore, 1981; 149, 48. Orr, G.W., Green, H.J., Hughson, R.L., Benett, G.W. A computer linear regression model to determine ventilatory anaerobic threshold. J. Appl. Physiol. 1982; 52: 1349-1352. 49. Caiozzo, V.J., Davis, J.A., Eliis, J.F., Azus, J.E., Vandagriff, R. A comparison of gas exchange indices used to detect the anaerobic threshold. J. Appl. Physiol. 1982; 53: 1184-1189. 50. Reinhard, U., Muller, P.H., Schmulling, R.M. Determination of anaerobic threshold by ventilation equivalent in normal individuals, Respiration, 1979; 38: 26-32. 51. Aunola, S. and Rusko, H. Aerobic and anaerobic thresholds determined from venous lactate or from ventilation and gas exchange in relation to muscle fiber composition. Int. J. Sports Med. 1986; 7: 161-166. 52. Neary, P.J., MacDougall, J.D.,Bachus, R., Wenger, H. A. The relationship between lactate and ventilatory thresholds: coincidental or casual effect? Eur. J. Appl. Physiol. 1985; 54: 104-108. 53. Cecca, M., MacDougall, D. Tsunoda, N. O'Hagan, F. The ventilatory threshold is not related to plasma lactate concentration. Med. Sci. Sports Exer. 1986; 18(suppl.2): 585. 54. Conconi, F., Ferrari, M., Ziglio, P.G, Droghetti, P, Codeca, L. Determination of anaerobic threshold by a non invasive field test in runners. J. Appl. Physiol. 1982; 52: 869-873. 55. Bodner M E, Rhodes E C. A review of the concept of the heart rate deflection point. Sports Med 2000; 30(1): 31-46. 56. Tokmakidis, S.P., Leger, L. and Pilianidis, T.C. Failure to obtain a unique threshold on the blood lactate concentration curve during exercise. Eur. J. Appl. Physiol. 1998; 77(4): 333-342. 57. Zacharogiannis, E. and Farrally, M. Ventilatory threshold, heart rate deflection point and middle distance running performance. J. Sports Med. Phys.Fit. 1993; 33: 337-347. 58. Jones, A and Doust, J Lack of reliability in Conconi's heart rate deflection point. Int. J. Sports Med. 1995; 16: 541-544. 59. Vachon, J., Bassett, D and Clark, S. Validity of the heart rate deflection as a predictor of lactate threshold during running. J. Appl. Physiol. 1999; 87: 452-459. 60. Petit, M., Nelson, C. and Rhodes, E. Comparison of a mathematical model to predict 10-km performance from the Conconi test and ventilatory threshold measurements. Canad. J. Appl. Physiol. 1997; 22: 562-572. 61. Hofmann,P., Pokan, R., Von Duvillard, S., Seibert, F., Zweiker, R., and Schmid, P. Heart rate performance curve during incremental cycle ergometer exercise in healthy young male subjects. Med. Sci. Sports Exer. 1997; 29: 762-768. 62. Bourgois, J. and Vrijens, J. (1998) The Conconi test:a controversial concept for the determination of the anaerobic threshold in young rowers. International Journal of Sports Medicine 19: 553-559. 63. Ballarin, E., Sudhues, U., Borsetto, C. Casoni, J., Grazzi, G., Guglielmi, C., Manfredinin, F., Mazzoni, G., and Conconi, F. (1996) Reproducibility of the Conconi Test: Test repeatability and observer variations. International Journal of Sports Medicine 17: 520-524. 64. Bassett D.R. Jr., Howley E.T. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med Sci Sports Exer. 2000; Jan 32(1), 70-84. 65. Farrel, P.A., Wilmore, J.H., Coyle, E.F., Billings, J.E. and Costill, D.L.: Plasma lactate accumulation and distance running performance. Med Sci Sports Exer. 1979; 11: 338-344. 66. Kumagai, S., Tanaka, K., Matsura, Y., Matsuzaka, A., Hirakoba, K. and Asano, K.: Relationship of the anaerobic threshold with the 5 km, 10 km and 10 mile races. Eur. J. Appl. Physiol. 1982; 49: 13-23. 67. Sjodin, B. and Jacobs, I.: Onset of blood lactate accumulation and marathon running performance. Int. J. Sports Med., 1981; 2: 23-25. 68. Karlsson, J. and Jacobs, I.: Onset of blood lactate accumulation during muscular exercise as a theoretical concept. Int. J. Sports Med., 1982; 3:190-194. 69. Maughan, R.J. and Leiper, J.B. Aerobic capacity and fractional utilization of aerobic capacity in elite and non-elite male and female marathon runners. Eur. J. Appl. Physiol. 1983; 52: 80-83. 70. Tanaka, K., Matsura, Y. Marathon performance, anaerobic threshold and onset of blood lactate accumulation. J. Appl. Physiol. 1984; 57: 640-643. 71. Ahuja A., Ghosh A.K., Goswami A., Mazumdar P., Khanna G.L. and Puri, T.P.S. Specific training and its effect on maximum aerobic capacity and ventilatory threshold of badminton players. Proceedings of Jakarta Coaching Seminar, Jakarta, Indonesian Badminton Association, 1989; 2-6. 72. Ghosh, A.K., Mazumdar, P., Goswami, A., Ahuja, A., Puri, T.P.S.: Heart rate and blood lactate response in competitive badminton. Ann Sports Medicine, 1990; 5: 85-88. 73. Yoshida T., Udo, M., Iwai K., Yamaguchi T. Physiological characteristics related to endurance running performance in female distance runners. J Sports Sci 1993; 11(1): 57-62. 74. Gaesser, G.A., Poole, D.C. Lactate and ventilatory thresholds: disparity in time course of adaptations to training. J. Appl.Physiol., 1986; 61: 999-1004. 75. Poole, D.C., Gaesser, G.A. Response of ventilatory and lactate threshold to continuous and interval training. J. Appl. Physiol., 1985; 58: 1115-1121. 76. Simon, J., Young, J.L., Blood, D.K., Segal, K.R., Case, R.B. Plasma lactate and ventilation thresholds in trained and untrained cyclists. J. Appl.Physiol., 1986; 60: 777-781. 77. Sjodin, B, Jacobs, I., and Svedenhag, J. Changes in onset of blood lactate accumulation (OBLA) and muscle enzymes after training at OBLA. Eur. J. Appl. Physiol. 1982; 49: 45-57. 78. Denis, C., Fouquet, R., Poty, P., Geyssant, A., Lacour, J.R. Effect of 40 weeks of endurance training on the anaerobic threshold. Int. J. Sports Med. 1982; 3: 208-214. 79. Saltin, B. and Hermansen, L. Glycogen stores and prolonged severe exercise. In G. Biix (Ed). Nutrition and physical activity, Almqvist & Wiksell, Uppsala, 1967; 2. 80. Karlsson, J. Lactate and phosphagen concentrations in working muscles of man with special reference to oxygen deficit at the onset of work, Acta.Physiol.Scand. 1971; Suppl, 358: 7. 81. Boyd, A.E., Giamber, S.R., Mager, M., and Lebovitz, H.E. Lactate inhibition of lypolysis in exercising man. Metabolism, 1974; 23: 531-534. 82. Gollnick, P.D., and King, D.W. Effect of exercise and training on mitochondria of rat skeletal muscle, Amer.J.Physiol, 1969; 216: 1502. 83. Andersen, P. and Henriksson, J. Capillary supply of the quadriceps femoris muscle of man: adaptive response to exercise. J.Physiol., London, 1977; 270: 677. 84. Holloszy, J.O. Effect of exercise on mitochrondrial oxygen uptake and respiratory enzyme activity in skeletal muscle. J.Biol. Chem. 1967; 242: 2278. 85. Hermansen, L., and Saltin, B. Blood lactate concentration during exercise at acute exposure to altitude, In: Exercise at altitude, R. Margaria, Ed. Dordrechit; Exerpta Medica Fdn, 1967; 48. 86. Yoshida T, Suda Y, Takeuchi N. Endurance training regimen based upon arterial blood lactate: effects on anaerobic threshold. Eur J Appl Physiol Occup Physiol 1982; 49(2): 223-230. 87. Allen, W.K., Seals, D.R., Hurley, B.F., Ehsani, A.A. and Hagberg, J.M. Lactate threshold and distance running performance in young and older endurance athletes. J. Appl. Physiol. 1985; 58: 1281-1284. 88. Bishop, D., Jenkins, D.G. and Mackinnon, L.T. The relationship between plasma lactate parameters, Wpeak and 1-h cycling performance in women. Med. Sci. Sports Exer. 1998; 30: 1270-1275. 89. Fouquet, R. and Poty, P. Effect of 40 weeks of endurance training on anaerobic threshold. Int. J. Sports Med. 1982; 3(4): 208-214. 90. Edwards A.M., Clark N., Macfadyen, A.M. Lactate and ventilatory thresholds reflect the training status of professional soccer players where maximum aerobic power is unchanged. J. Sports Sci. & Med. 2003; 2: 23 _ 29. 91. Coyle, E.F. Integration of the physiological factors determining endurance performance in athletes. Exer.& Sports Sci. Rev. 1995; 23: 25-31. 92. Hermansen, L. Lactate production during exercise. In: Muscle metabolism during exercise. Pernow, B., Saltin, B. Eds. New York: Plenum. 1971. 93. Hoffor A.S., Harrison A.C. and Kirk P.A. Anaerobic threshold alterations caused by interval training in 11-year-olds. J. Sports Med. Phys. Fit. 1990; 30(1): 53-56. 94. Burke J., Thayer R., and Belcamino M. Comparison of effects of two interval-training programmes on lactate and ventilatory thresholds. Br J Sports Med 1994; 28(1): 18-21. 95. Ready A.E. and Quinney H.A. Alterations in anaerobic threshold as the result of endurance training and detraining. Med Sci Sports Exerc 1982; 14(4), 292-296. 96. Henritze J., Weltman A., Schurrer R.L. and Barlow K. Effects of training at and above the lactate threshold on the lactate threshold and maximal oxygen uptake. Eur J Appl Physiol Occup Physiol 1985; 54(1): 84-88. 97. Billat L.V. Interval training for performance: a scientific and empirical practice. Special recommendations for middle- and long-distance running. Part I: aerobic interval training. Sports Med 2001; 31(1): 13-31. 98. Billat L.V. and Koralsztein J.P. Significance of the velocity at VO2max and time to exhaustion at this velocity. Sports Med 1996; 22(2): 90-108. 99. Billat L.V., Morton R.H., Blondel N., Berthoin S., Bocquet V., Koralsztein J.P., and Barstow T.J. Oxygen kinetics and modelling of time to exhaustion whilst running at various velocities at maximal oxygen uptake. Eur. J. Appl. Physiol. 2000; 82(3): 178-187. 100. Grant S., Craig I., Wilson J. and Aitchison T. The relationship between 3 km running performance and selected physiological variables. J Sports Sci 1997; 15(4): 403-410. 101. Belman M.J. and Gaesser G.A.. Exercise training below and above the lactate threshold in the elderly. Med Sci Sports Exerc 1991; 23(5): 562-568. 102. Ghosh, A.K. and Mukhopadhaya, S. Physiological profile of Indian elite middle and long distance runners. 2002. Unpublished data from Department of Exercise Physiology, Sports Authority of India, Faculty of Sports Sciences, National Institute of Sports, Patiala, India. Copyright 2004 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj04003f2.jpg] [mj04003t1.jpg] [mj04003f4.jpg] [mj04003f1.jpg] [mj04003f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}