 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 11, No. 1, January 2004, pp. 52-59 Physical and Mental Health Problems of the Elderly in a Rural Community of Sepang, Selangor Sherina Mohd Sidik, Lekhraj Rampal, Mustaqim Afifi Unit of Family Medicine, Department of Community Health,
Faculty of Medicine and Health Sciences, Universiti Putra Malaysia,
43400 Serdang, Selangor, Malaysia
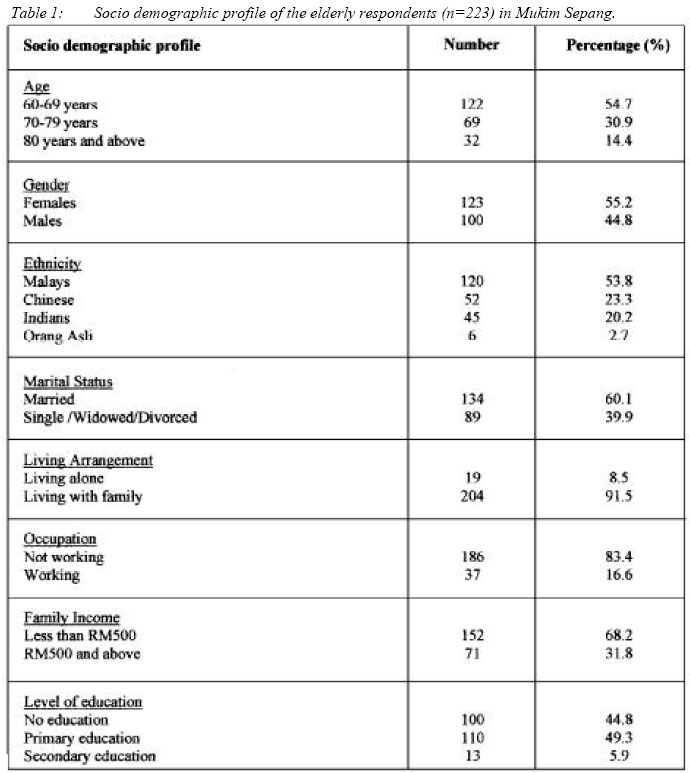
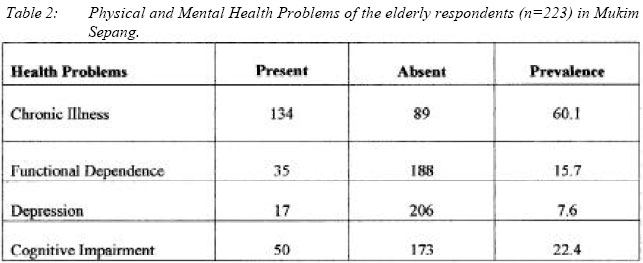
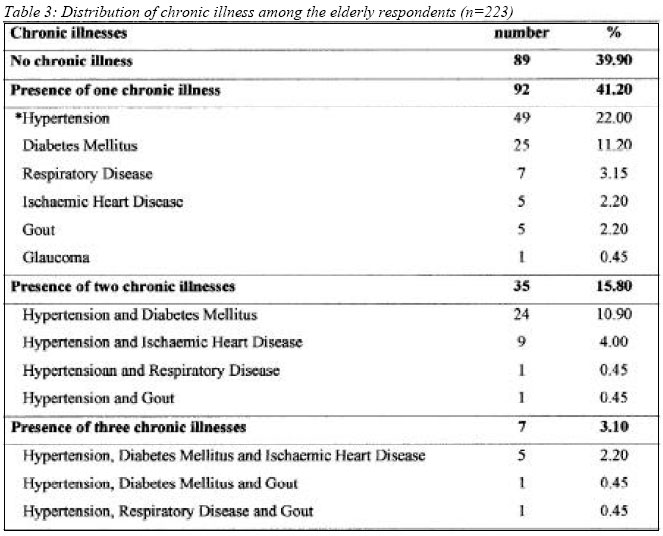
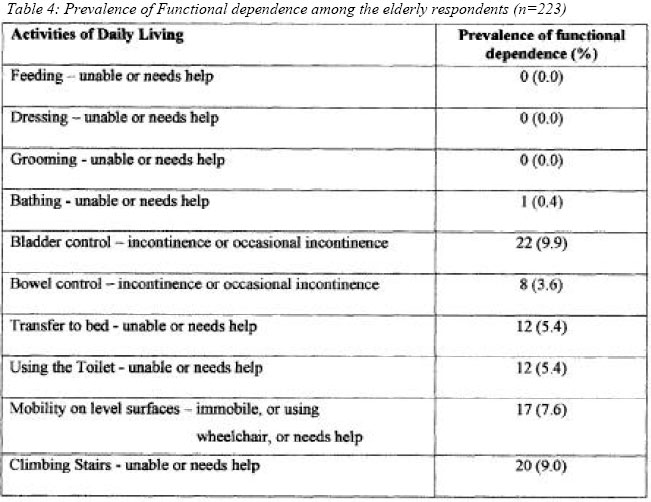
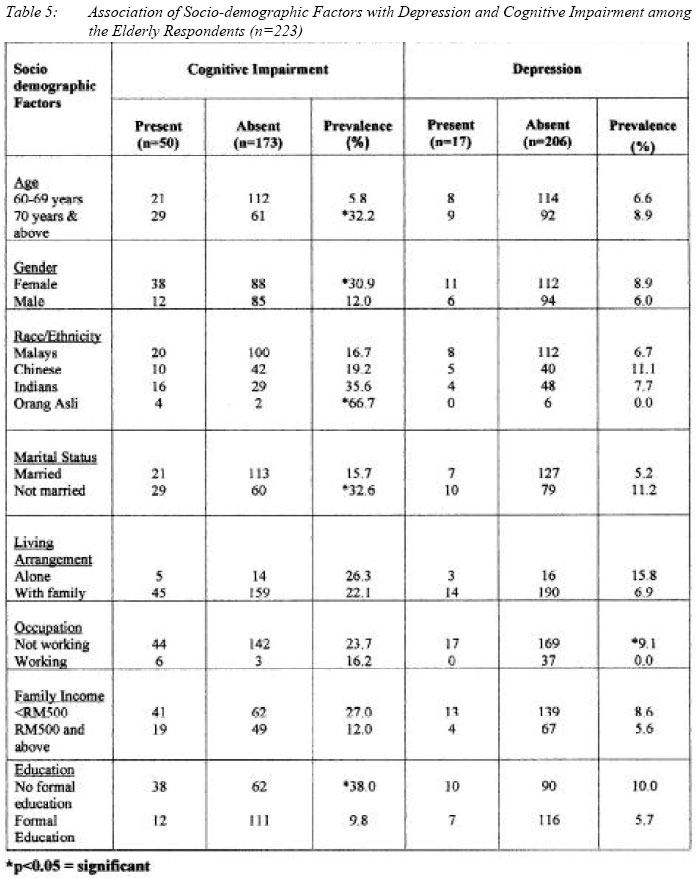
Submitted-11.8.2003 Code Number: mj04006 The prevalence of aging population is increasing not only in developed countries, but also in developing countries like Malaysia. The aim of this study was: (1) to determine the prevalence of physical and mental health problems, and (2) to determine the association of these health problems with socio demographic factors among the elderly in a rural community in Sepang, Selangor. A cross sectional study design was used. Five out of nine villages were selected via random sampling. The elderly in the selected villages were interviewed using a pre-tested structured questionnaire which included the GDS-30, ECAQ and Barthel Index. Out of 263 elderly residents (6.2% of the total population), 223 agreed to participate in the study giving a response rate of 84.8%. The mean age of the respondents was 69.7 + 6.8 years with a median of 68 years. The prevalence of physical health problems such as chronic illness and functional dependence were 60.1% and 15.7%, respectively. While the prevalence of mental health problems such as depression and cognitive impairment were 7.6% and 22.4%, respectively. Among the health problems studied, depression was found to be significantly associated with unemployment (p<0.05), where as cognitive impairment was significantly associated with age, gender, ethnicity, marital status and level of education (p<0.05). Key words : Elderly, Physical-health-problems, Mental-health-problems, Rural-community Introduction The ageing of the world's population is a global phenomenon with extensive economic and social consequences. The ratio of the elderly population (60 years and older) is now 1 in 10. By the year 2050, the ratio would have increased up to 1 in 5. This older population will continue to age and currently, people aged 80 years and older represent 11% of the population aged 60 and above. By 2050, those over 80 will represent 27% of this older population (1). The tempo of ageing is expected to be more rapid in developing nations. Because of this, developing nations will have less time than their developed counterparts to adapt to the consequences of population ageing (2). In the year 1997, the Malaysian population aged 60 years and above was approximated to be 1 million. In the year 2000, this particular group has increased to 1.5 million and will further increase to 4 million by the year 2025 (3). Ageing of a population is a matter of great concern for the health sector. The elderly are, on the whole less healthy than the non-elderly. Among the elderly, increasing age is associated with higher morbidity and higher use of health services (number of visits to doctors and hospitalizations) (4). A study among Malaysian elderly indicated that the elderly in rural areas expressed more need for health services and experienced greater financial hardship than in urban areas (5). In anticipation of Malaysia heading towards an aging nation, health care providers need to be alert and informed of the special needs of the elderly (6). With the increase in elderly population, a country's health spending also increases. The escalation in health care cost may be contained by improving preventive care, and utilizing family and community support as an alternative to hospitalization whenever suitable (7). Besides availability of social support, the ability of the elderly to live independently in the community is also influenced by their health status and functional capabilities. The aim of this study was: (1) to determine the prevalence of physical and mental health problems, and (2) to determine the association of these health problems with sociodemographic factors among the elderly in a rural community in Sepang, Selangor. Materials and Methods This cross sectional study was conducted from 17th June to 25th July 2002 in the rural community of Mukim Sepang. Mukim Sepang covers an area of 20,441 hectares with a population of 7598. Five out of nine villages were randomly selected. All elderly in the selected villages were interviewed. Elderly who refused to participate and those who had significant communication problems were excluded from the study. The socio economic factors included in this study were age, gender, ethnicity, marital status, educational level, living arrangement, occupation and family income. In this study, health problems among the elderly were divided into physical and mental problems. Chronic illness and functional dependence were selected to represent physical health problems, whereas depression and cognitive impairment were selected to represent mental health problems. Selection of these health problems were made based on their common occurrence among the elderly population. Hypertension, Diabetes Mellitus, Respiratory Disease (Bronchial Asthma and Chronic Obstructive Pulmonary Disease), Ischaemic Heart Disease, Osteoarthritis and Gout were selected to represent chronic illnesses. These diseases were detected through the questionnaires administered in the study. Functional dependence was assessed using the Barthel's Index (BI). The BI consists of 10 questions measuring basic Activities of Daily Living (ADL). Functional dependence in basic ADL implies that the elderly respondent needs assistance in one or more of their ADL (8). The Geriatric Depression Scale (GDS) consisting of 30 questions was used to screen for depression. The total scores range from 0 to 30. Based on the GDS guidelines, a cut off score of more than 10 was used to identify depression (9). The Elderly Cognitive Assessment Questionnaire (ECAQ) was used to screen for cognitive impairment among the elderly respondents. The ECAQ consists of 10 items grouped under 3 categories: memory (3 items), orientation (6 items) and memory recall (1 item). Each item has a weightage of one mark for correct response. Respondents with scores of 5 and below were identified as having cognitive impairment (10). Data was analysed using Statistical Package for Social Sciences version 10.0. Association between factors was considered to be statistically significant at p < 0.05. Results There were 4241 residents in the four villages and one small town studied. Out of these 4241 residents, 263 (6.2%) were 60 years old and above. Out of these 263 elderly residents, 223 agreed to participate in the study giving a response rate of 84.8%. The mean age of the respondents was 69.7 + 6.8 years with a median of 68 years. Mean age of the females was higher (70.3 + 8.2) than the males (68.9 + 7.2). However, this difference in the mean age was not statistically significant (Mann-Whitney test = 5560, z = 1.4, p > 0.05). Fifty-five point two percent (55.2%) of the respondents were females. There was a much higher percentage of females (84.5%) compared to males (15.5%) among the widowed. The socio-demographic profile of the elderly respondents are shown in Table 1, whereas Table 2 shows the prevalence of each health problem of the elderly respondents. Chronic Illness One hundred thirty four of the respondents (60.1%) were diagnosed to have chronic illness such as hypertension, diabetes mellitus, ischaemic heart disease, bronchial asthma or gout. Some of them had a combination of two or three illnesses (Table 3). The rest (39.9%) were healthy except for some minor ailments. No socio demographic factors were found to be associated with chronic illness among the elderly respondents. Functional Dependence Thirty-five (15.7%) of the respondents were dependent in at least one function of the ADL. The most common problem identified was urinary incontinence (9.9%). However, none of the respondents were dependent in feeding, dressing and grooming (Table 4). Geriatric Depression Scale (GDS) Score The mean GDS score was 4.34 ± SD 3.76 and the median score was 3.00. The scores ranged from 0 to 27. Based on the GDS scores, 17 of the respondents were found to have depression. Therefore, the prevalence of depression among the elderly in Mukim Sepang was 7.6%. In this study, only unemployment was found to be significantly associated with depression among the elderly (p=0.04) (Table 5). Elderly Cognitive Assessment questionnaire (ECAQ) scores The mean ECAQ score was 7.65 + 0.156 and the median score was 8.00. The scores ranged from 3 to 10. Based on the ECAQ scores, 50 (22.4%) out of 223 respondents had scores of 5 or less. The study shows that the prevalence of cognitive impairment among the elderly in Mukim Sepang was 22.4%. Cognitive impairment among the elderly was significantly associated with age, gender, ethnicity, marital status and level of education (Table 5). Discussion Socio demographic Profile The results of this study showed that there were a higher percentage of females compared to males among the elderly respondents. There was also a much higher percentage of widowhood among the females compared to males. These findings could be due to the comparatively higher longevity of life in females. Malaysian population data indicates that the average life span for females (75.5 years) is longer than males (70.6 years) (11). This study also found that the mean age of the females was higher (70.3 + 8.2) than the males (68.9 + 7.2). Widowed females are also less likely than males to remarry (12). The findings of this study corresponded to that of the national survey(11) and an earlier study on ageing in Malaysia (12). As expected, a high proportion of elderly people live with their families. This finding corresponded to another study in Malaysia which found that 90% of the elderly respondents in rural communities lived with their families (5). It has been well documented that elderly people in developing countries such as Malaysia are more likely to be living in multi-generation households, than elderly in developed countries (5, 13). Nearly half of the elderly respondents had received no education. This corresponded to a study among Malaysian elderly in rural communities by Shahar (2001). In her study, Shahar explained that the low percentage of educated elderly was due to the lack of educational opportunities, particularly in rural areas before Independence in 1957 (5). Inspite of their low educational level, more than half of the respondents in this study were pensioners and 16.6% were still employed. However, majority of them had total family income of less than RM500 per month. This income level corresponded to the Malaysian mean per capita income of RM537.40 per month. The poverty line level in Malaysia is RM212 per month (14). Chronic Illness The prevalence of chronic illness among the elderly respondents was high (60.1%). This finding corresponded to other studies, which found that 50- 60% of the elderly had chronic illnesses(5, 15). The most prevalent chronic illness in this study was hypertension (22.0%), followed by diabetes mellitus (11.3%). Most of the elderly with chronic illness had only one illness, with a smaller percentage having a combination of 2 or 3 illnesses. In the study by Shahar, the major chronic illness reported among the elderly were joint pains (45.0%), followed by hypertension (22.9%) and respiratory problems (15.1%).5 Another study among the elderly in Hong Kong found that the most common chronic illness were rheumatism (34.2%) and hypertension (32.2%).15 In this study, there was probably an under reporting of joint pains as the respondents were only asked to report on diagnosed chronic illness. Joint pains were classified as "symptoms" and not as "diagnosed chronic illness" in this study. There was no association between chronic illness and any socio demographic factor in this study. This is probably because chronic illness can affect any elderly regardless of their social status and background. Functional Dependence The Barthel's Index (BI) measures the basic capacity of persons to care for themselves by assessing their activities of daily living (ADL) (8). This study showed that the 15.7% of elderly were dependent in at least one activity of ADL. Salleha (16). also reported that 15.1% of the elderly had problems in one or more ADL functions. However, the prevalence of functional dependence among elderly in Mukim Sepang was lower than that reported by Chan et al (8). in Singapore (17.0%). The most common functional dependence in this study was urinary incontinence (9.9%). This finding corresponded to a rural elderly survey in Banting, Malaysia where 9.1% of the elderly had urinary incontinence (17). A study among the elderly in Singapore also found that the most common functional dependence was urinary incontinence (14.5%) (8). Depression Studies have shown that depression affects 8% to 20% of elderly in the community (18). The prevalence of depression among the elderly in the community in this study was 7.6%. Two local studies on depression among the elderly carried out in primary health care clinics showed higher prevalence of 14% and 18%(19, 20). The higher prevalence of depression in these studies is probably due to the higher underlying morbidity of elderly attending primary health care clinics. In this study, the prevalence of depression was found to be significantly higher among the elderly respondents who were unemployed. A study on socio-cultural factors in late onset depression in India also found that there was an increased rate of depression among the elderly who were unemployed. It was explained that unemployment was associated with low family income which was associated with depression (21). In Malaysia the elderly are generally less well off financially compared to the rest of the adult population due to their inability to earn (22). Unemployment gives rise to financial problems which cause the elderly to be dependent on others for financial support (21). Cognitive Impairment This study showed that the prevalence of cognitive impairment was 22.4% among the elderly respondents. This finding was consistent with an earlier study which identified that 24.0% of Malaysian elderly in urban settlements had cognitive impairment (23). In this study cognitive impairment was significantly higher among the elderly in the above 70 years age-group compared to those in the 60 to 69 age-group. Other studies have also shown a positive association between cognitive impairment and increasing age (23, 24). The prevalence of cognitive impairment among the elderly respondents was significantly higher in females compared to males in this study. This finding was similar to an earlier study where there was a female preponderance by 4 times in the presence of dementia among elderly in urban settlements in Malaysia (23). This study also found that the prevalence of cognitive impairment was higher among the elderly who were not married (either single, widowed or divorced) compared to those who were still married. The Zaragoza study also showed that the rate of cognitive impairment and dementia was higher among the elderly who were widowed compared to those who were still married (24). Cognitive impairment was also significantly higher among the elderly respondents with no education compared to those with education. Other studies also found that low education level was significantly associated with cognitive impairment and increased risk for dementia (9, 25). There is a hypothesis that education increases the brain cognitive reserve, and the bigger the reserve the more protection there is from dementia. There is also some evidence that mental stimulation can delay the onset of cognitive impairment (23, 25). In this study, cognitive impairment was found to be significantly associated with ethnicity, with the highest prevalence among the "Orang Asli" ethnic group. However, the proportion of this ethnic group in our study is too small. Conclusion As reflected in this study, health problems among the elderly are common. The health problems identified in this study were physical (chronic illness and functional dependence), as well as mental (depression and cognitive impairment). As Malaysia is heading towards an aging nation, health care providers need to be aware of these health problems among the elderly. The findings of this study can be used as a baseline for larger in-depth studies to identify factors significantly associated with these problems. As the ability of the elderly to continue living independently in the community is influenced by their health status, these factors need be addressed appropriately so that the associated health problems can be managed and reduced. Acknowledgement We would like to express our gratitude to Professor Dr Azhar Md Zain for all his help and support. We also thank the State Director of Health, Selangor for permission to publish our findings. References
Copyright 2004 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj04006t1.jpg] [mj04006t5.jpg] [mj04006t2.jpg] [mj04006t4.jpg] [mj04006t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}