 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
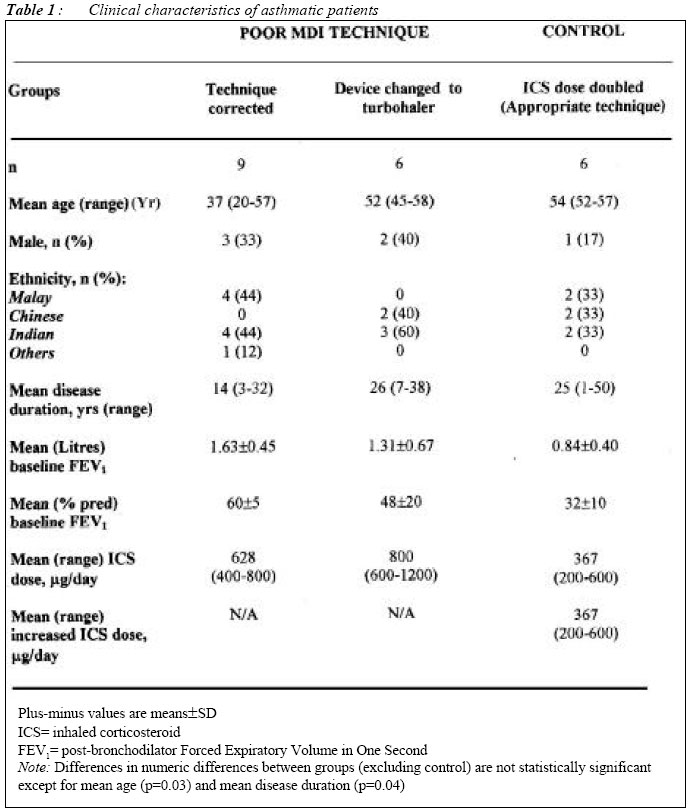
Malaysian Journal of Medical Sciences, Vol. 11, No. 1, January 2004, pp. 60-65 Correcting Metered-Dose Inhaler Technique Vs Switching to Turbohaler in Asthmatic Patients - a Study on "Real-Life Effectiveness Li-Cher Loh, Pek Ngor Teh IMU Lung Research, Department of Medicine,
International Medical University, Clinical School, Seremban
70300, Negeri Sembilan,
Malaysia
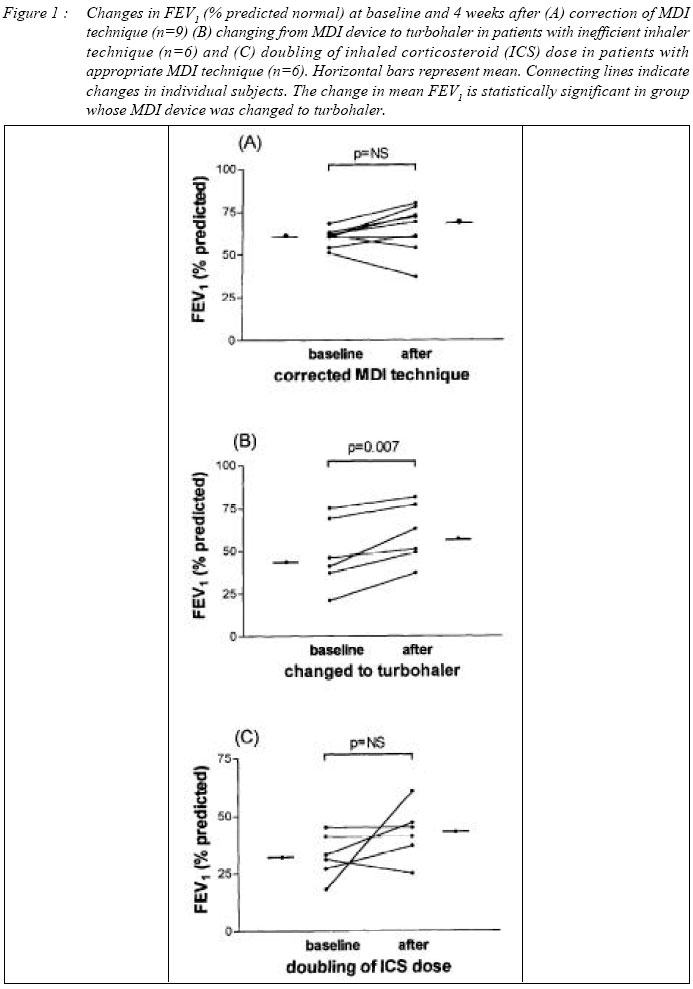
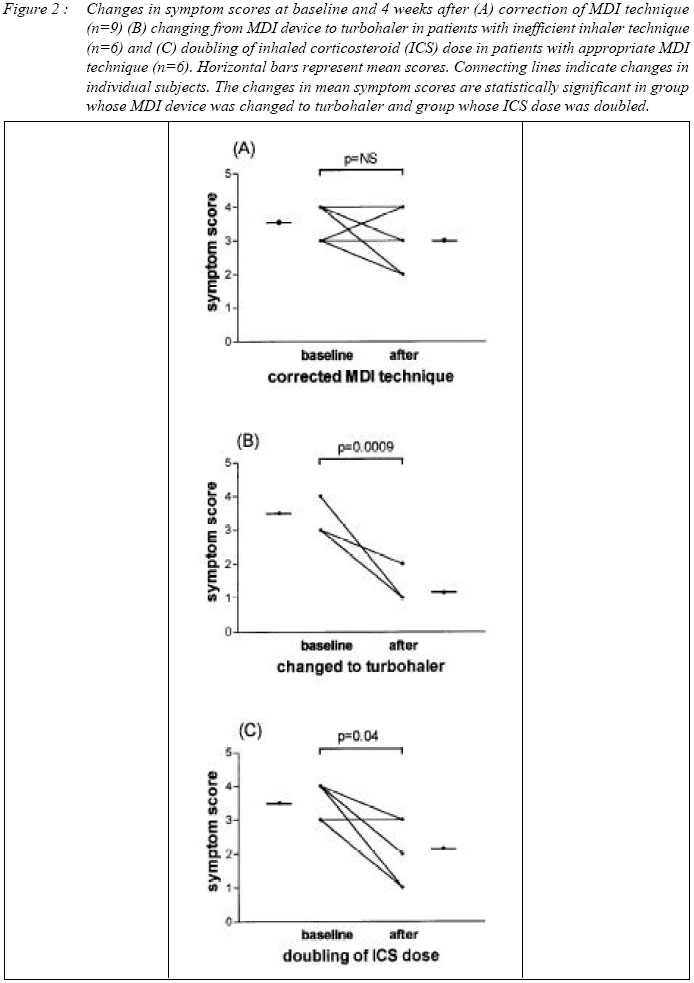
Submitted-10.5.2003, Code Number: mj04007 In practice, asthmatic patients whose metered-dose inhaler (MDI) technique is inefficient are either corrected or changed to dry powder breath-actuated or spacer device that is easier to handle. Based on `real life clinic circumstances', we studied 15 symptomatic asthmatic patients whose MDI techniques were inefficient that either received correction in their technique (n=9) or were changed to turbohaler (n=6). For comparison, we also studied a similar group of symptomatic asthmatic patients (n=6) with appropriate MDI techniques that were treated by doubling of inhaled corticosteroid (ICS) dose. After 4 weeks, FEV1 and symptom scores in the turbohaler group was significantly improved from baseline but not in the corrected MDI group. The group whose ICS dose was doubled also showed significant improvement in symptom scores but not in FEV1. We question the benefit gained by correcting MDI technique in some asthmatic patients compared to that of switching over to more user-friendly devices such as turbohaler. In our study, the improvement observed with turbohaler appears to be more than a mere doubling of drug delivery to the lungs and may relate to the recognized greater consistency of drug delivery by turbohaler compared to MDI device. Key words : Asthma, metered-dose inhaler, turbohaler Introduction Meter-dose inhaler (MDI) as a means of delivering anti-asthma medication has been available in Malaysia for the past 30 years. The device is relatively cheap compared to the newer dry-powdered inhaler devices and remains popular among healthcare providers and patients (1, 2). However, difficulty in correctly handling the MDI device among many patients is well-documented (3-5) and this problem can seriously compromise the optimal delivery of medication dose in treating asthma. In a local population of Malaysian asthmatic patients, we recently reported that as high as 42% did not handle the MDI device correctly (6). In this study of patients followed up in the medical outpatient clinic, we investigated the `real-life' effectiveness of correcting MDI techniques compared to switching to dry-powdered device, turbohaler, in inefficient MDI handlers who continued to have asthmatic symptoms. Since lung deposition from turbohaler is doubled that of MDI (7, 8),we included a similar group of asthmatic patients who correctly handled the device but whose inhaled corticosteroids (ICS) dose was doubled for control of asthma symptoms for comparison with the turbohaler group. Patients and Methods Patients Twenty four physician-diagnosed asthmatic patients with inefficient MDI techniques and 6 with appropriate MDI techniques were recruited from the study population of our earlier study (6). Our criteria of deciding on appropriate or inefficient MDI techniques have been previously described. Briefly, the techniques was assessed by a single chest physician (LCL) on the three crucial steps of adequate lip closure around mouthpiece, coordinated hand-month inspiration following expiration and breath-holding of at least 5 seconds. The techniques was considered as inefficient if any one of the three steps was not carried out optimally. The reason for choosing these three steps alone was based on the belief that the other steps such as removing cap before inhaling, taking one inhalation each time, were easily rectifiable compared to the three steps. Other inclusion criteria were on-going asthmatic symptoms (symptom score >3) inadequately controlled by the currently prescribed medications and had been using MDI device for at least one year. All patients recruited were taking regular, ICS. Study Design Clinical details including duration of asthma, post-bronchodilator FEV1 and the duration of MDI used, were obtained from all subjects. Wherever possible, this information was validated from hospital medical notes. In an open fashion, taking into consideration individual preference and correctability of inhaler technique, those whose technique was poor were treated by correction of inhaler technique or a change to turbohaler device while leaving the dose of ICS unescalated. After 4 weeks, the same physician reassessed all subjects. The outcome measures were changes in FEV1 and symptom scores at four weeks. In the control group whose MDI technique was appropriate, inhaled CS dose was doubled and similar assessment carried out at 4 weeks. All other anti-asthma medications, if any, were kept unchanged over this study period. Symptom scores Patients' asthmatic symptoms were asked by the single investigator during the study visits and graded from score 1 to 4. Score I indicates that patient is hardly aware of his/her asthmatic symptoms over the last 3 days. Score 2 indicates that patient is aware of his /her asthmatic symptoms but not bothered by them in his/her daily activities. Score 3 indicates that patient is bothered by his/her asthmatic symptoms during his/her daily activities. Score 4 indicates that the daily activities of the patient are hindered by his/her asthmatic symptoms. This symptom scoring is a validated method used in a large-scale asthma study (9). Statistical analysis Descriptive statistics were used to study patients' clinical characteristics and statistical differences in numeric variables between groups were studied using unpaired t test. Changes in mean FEV1 and symptom score at baseline and after intervention were tested for significance using paired t tests (two-tailed) as they approximate Gaussian distribution. P value of less than 0.05 was considered as statistically significant. All analysis were performed using PrismGraph, Statistical Package Version 8. Results The mean age and disease duration are significantly greater in the turbohaler group compared to the MDI group. All other asthma-related variables i.e. mean FEV1 and ICS daily dose are comparable [Table 1]. The mean change in FEV1 (% predicted normal) is statistically significant in the turbohaler group [mean difference (95% CI)= -11.58 (-18.39 to -4.77) p=0.007] but not so in the MDI group [-4.88 (-12.68 to 2.89) p=0.18] or the control group whose ICS dose was doubled [-10.13 (-28.60 to 8.33); p=0.21] [Figure 1]. The mean change in symptom scores are statistically significant in the turbohaler group [2.33 (1.47 to 3.19); p=0.0009] and control group whose ICS dose was doubled [1.33 (0.06 to 2.60); p=0.04] while the change in the MDI group is not statistically significant [0.55 (-0.22 to 1.33); p=0.13] [Figure 2]. Discussion Following our previous larger study on the technical use of MDI device by asthmatic patients, we followed up a small group of these patients with inefficient MDI technique who were managed as in `real life clinic circumstances' by either correction of MDI technique or by switching to a dry-powdered breath-actuated device, turbohaler. At 4 weeks, FEV1 and symptoms were significantly improved in the group whose MDI devices were changed to turbohaler, but not in the group whose intervention was to correct the MDI technique. As commonly practiced, correction of MDI technique is the next move in a patient whose MDI technique is clearly inefficient. If the patient continues to have difficulty in correctly handling the MDI device, it is then advisable to switch to a more `straightforward' device such as a dry powdered or MDI facilitated by spacer device. The results of our `real life' study challenge the effectiveness of correcting MDI technique in some asthmatic patients considered as `teachable', let alone those who require constant reinforcement on the correct way of handling MDI device. Since there is no objective measurement of drug deposition into the lung in our study, it is not possible to ascertain the degree of drug delivery that has been improved by correction of MDI technique. Nevertheless their trend towards improvement in FEV1 and symptoms indicated that there is some improvement in drug delivery but is clearly small compared to significant improvement observed in the turbohaler group. The control group whose patients' ICS dose was doubled is added for comparison with turbohaler group, since use of turbohaler device effectively doubled the delivery of ICS. The degree of improvement is smaller than that of turbohaler group, indicating that doubling of ICS dose alone is not sufficient to explain to benefit brought about by switching to turbohaler and lend support to the idea that the reduction of intersubject and intrasubject variability when using turbohaler compared to MDI is clinically important (7, 8). To our knowledge, there has been no study comparing the `real life' effectiveness of correcting MDI technique with switching to dry powder device such as turbohaler. This is understandable considering the difficulty of establishing comparable study cohorts in standard drug efficacy study protocol (10) and perhaps, lack of interest to study such issues nature by pharmaceutical firms. Our resort to `real life clinic circumstances' as a means of studying the `real life' effectiveness is practical and provide early evidence that can pave the way foward a larger study, either to validate or refute our present conclusion that the benefit of correcting MDI technique in seemingly `teachable' asthmatic patients is small and that greater consideration should be given for switching to dry powder breath-actuated devices. Acknowledgements The authors are grateful to the Chest Clinic nurses for carrying out the lung function tests on study subjects. This study was not supported in any way by pharmaceutical firms. References
Copyright 2004 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj04007t1.jpg] [mj04007f2.jpg] [mj04007f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}