 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 11, No. 1, January 2004, pp. 66-74 The Prevalence Of Diastolic Dysfunction In Patients With Hypertension Referred For Echocardiographic Assessment of Left Ventricular Function Abdul Latif Mohamed, Jun Yong, Jamil Masiyati, Lee Lim, Sze Chec Tee International Medical University, Clinical School, Seremban
70300, Negeri Sembilan,
Malaysia
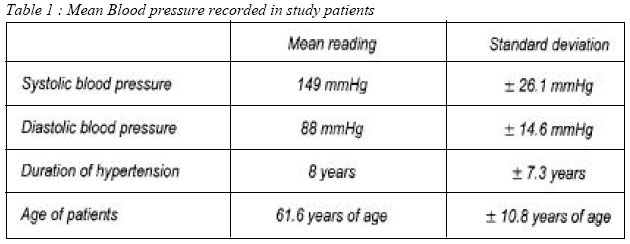
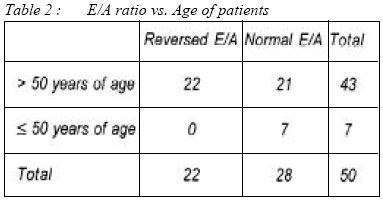
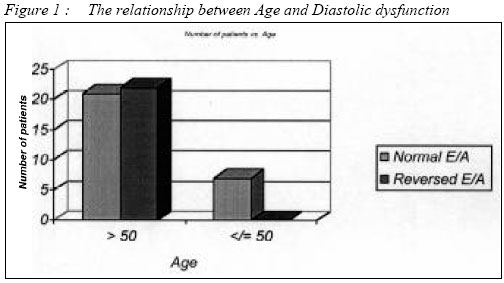
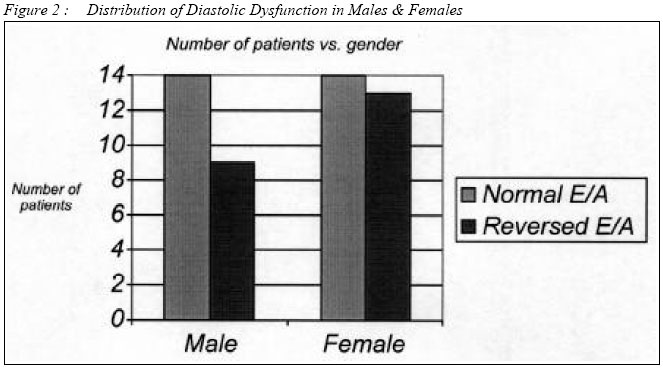
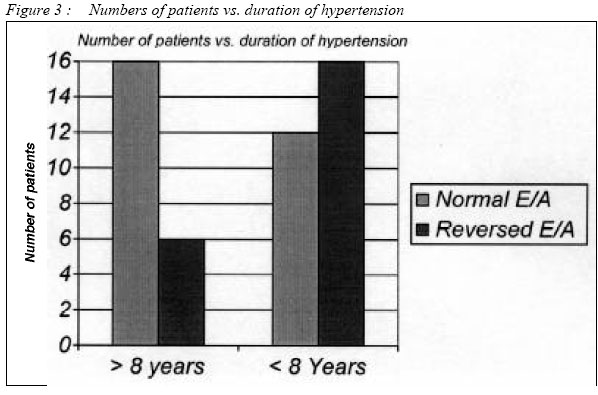
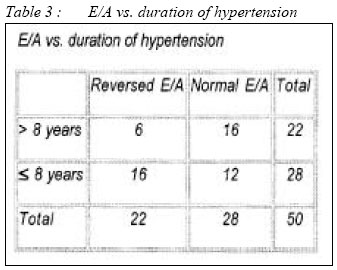
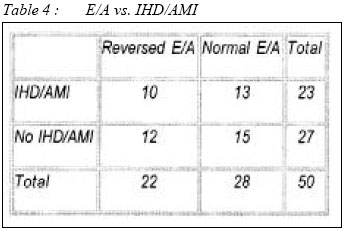
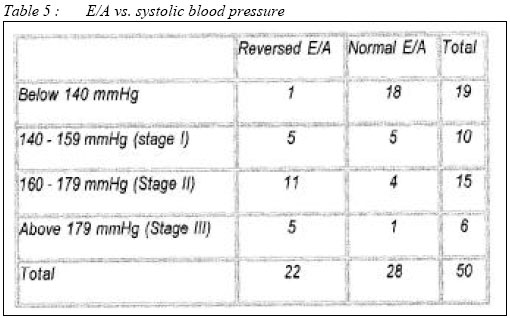
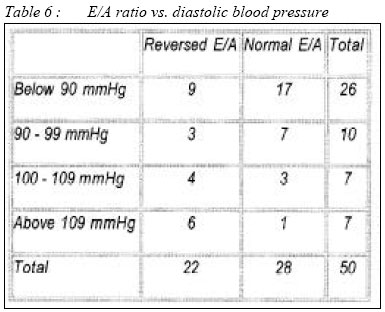
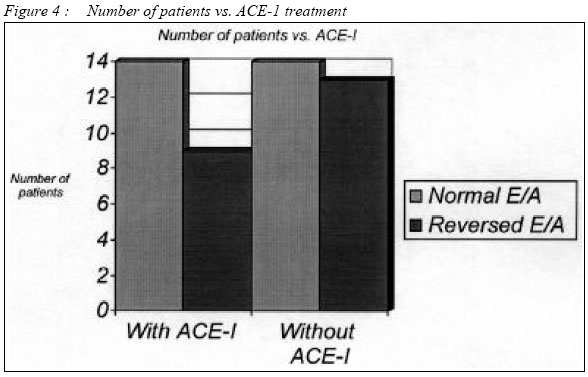
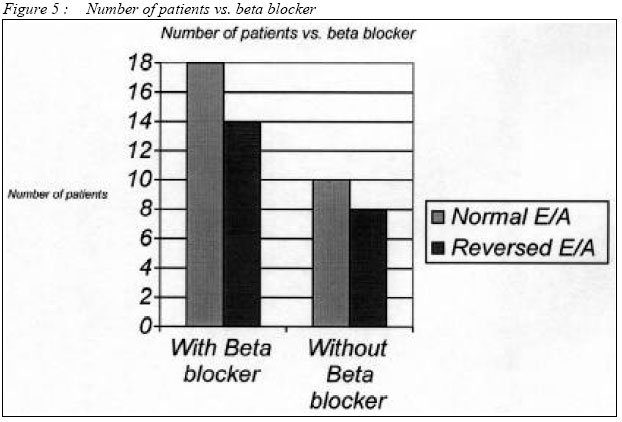
Submitted-10.5.2003 Code Number: mj04008 Hypertension is the major cause of congestive cardiac failure all over the world. It is under diagnosed and achievement of optimal therapy is difficult and costly. Diastolic dysfunction is an early poor prognostic factor in hypertension and is a reversible condition. Early detection and treatment is necessary to avoid cardiac complications. The objective of this study was to assess the occurrence of diastolic dysfunction in hypertensive patients referred for echocardiograph assessment of left ventricular function in a secondary hospital. It was also designed to determine whether contributing factors such as age, gender, systolic and diastolic pressure, duration of hypertension, previous myocardial infarct or ischemic heart disease and choice of anti-hypertensive drugs influence the development of diastolic dysfunction in these hypertensive patients. The analysis of diastolic dysfunction was based on the E/A ratio using Doppler echocardiogram. All of the patients were recruited from the Echocardiography Unit, Department of Medicine, Seremban General Hospital. Fifty patients with history of hypertension were selected for the study. Out of These 22 patients (44%) were found to have diastolic dysfunction; 39.1% of male patients (9 out of 23) and 48.1% of female patients (13 out of 27). Other contributing factors of diastolic dysfunction were found in patients : (a) with more than 8 years history of hypertension (12%) (b) with history of pre-existing IHD/AMI (20%), (c) stages II - III of systolic hypertension based on 6th Joint National Committee recommendation (73%) (d) on ACE-inhibitor (18%) and (e) on Beta-blocker (28%) In conclusion, the study had demonstrated that the duration of hypertension, both systolic and diastolic blood pressure and age of patients are important prognostic indicators in predicting the development of diastolic dysfunction in hypertensive patients. Key words : Diastolic Dysfunction, Echocardiography, Hypertension Introduction Hypertension is found to be prevalent in 24% of the Malaysian population according to the second Malaysian Health & Morbidity Survey. It is one of the commonest cause of congestive cardiac failure which is among the highest cause of mortality in Malaysia. It is therefore important to identify early risk factors in hypertension that would indicate the onset of cardiac failure. The use of echocardiography in identifying diastolic dysfunction in hypertension is probably underutilized in many secondary centers. It would be a very useful tool in guiding therapy of hypertension and help optimize cost and compliance as well as target objectively to reverse early complications. Diastolic dysfunction is a common complication of chronically elevated blood pressure. Hypertension as a cause of congestive heart failure frequently is under-recognized, partly because, at the time the heart failure develops, the left ventricle at the stage of diastolic dysfunction is unable to generate the high blood pressure, thus obscuring the etiology of the heart failure. The prevalence of asymptomatic diastolic dysfunction in patients with hypertension and without left ventricular hypertrophy may be as high as 33% (1). Chronically elevated afterload and resulting left ventricular hypertrophy can adversely affect both the active early relaxation phase (E) and late compliance phase of ventricular diastole (A). Diastolic dysfunction in hypertension is common. It is usually, but not invariably, accompanied by left ventricular hypertrophy. By definition, E/A ratio is the ratio of peak early diastolic filling velocity to peak filling velocity of atrial contraction in the mitral flow velocity pattern. The late phase is of course dependent upon atrial contraction and therefore is absent in atrial fibrillation (2). With this in mind, we utilized the E/A ratio, measured with pulsed wave doppler, in the assessment of left ventricular function in hypertensive patient. Characteristically, when diastolic dysfunction is present, a greater portion of end-diastolic volume is the result of late filling rather than early filling. Therefore, the E/A ratio is reduced in diastolic dysfunction. Our aims apart from establishing the occurrence of diastolic dysfunction in hypertensive patients, were also to identify other factors that may be associated with diastolic dysfunction such as age, gender, systolic and diastolic pressure, duration of hypertension, previous myocardial infarct or ischemic heart disease and choice of anti-hypertensive drugs. Methodology Types of research We utilized both qualitative and quantitative research methods including interviews, data analysis. The study was based on a cross-sectional study design. Recruitment of sample This retrospective study was conducted in the echocardiography unit of Seremban General Hospital. Between December 2001 and April 2002, we managed to enroll 50 consecutive primary hypertensive patients whom were scheduled to undergo echocardiography for cardiac assessment. Consent was taken before we obtained their health information. This study was approved by the local ethics committee Primary data Echocardiograph was done by a single operator using the Toshiba power vision® echocardiography machine. Echocardiograph measures of E/A using pulsed Doppler technique at the level of the tip of the mitral valve leaflets were used to assess the presence or absence of left ventricular diastolic dysfunction. The threshold of <1.0 was being used as an indication of reversed E/A ratio. Blood pressure was measured using Accuson mercury sphygmomanometer after 5 minutes of rest and sitting position. Average of 3 blood pressure readings were taken as representing "clinic blood pressure". This was done just prior to echocardiograph measurement. Interviews and questionnaires We measured the following categories of factors that might be associated with diastolic dysfunction in hypertensive patient: age, gender, duration of hypertension, history of previous myocardial infarction or ischemic heart disease and anti-hypertensive medications. Duration of hypertension was taken as the period from the diagnosis of hypertension until the time of assessment. In this study, the duration of hypertension ranges from 2 months to 30 years. We also included 5 newly diagnosed hypertensive patients. Occurrence of ischaemic heart disease prior to the time of assessment with diagnosis by history from the case notes, positive stress test and/or electrocardiogram changes. Statistics Result of continuous data were presented as mean ± standard deviation. Chi-square analysis were performed on dichotomous categorised data to analyse the associations. Presence or absence of E/A reversal in echocardiograph assessments in each subgroup was the main parameter assessed statistically. Results Patient Demography We collected a total number of 50 patients over a period of 5 months. Out of these, 23 were males and 27 were females, which represents 46% and 54% respectively. 28 patients (56%) were found to have normal E/A ratio while another 22 patients (44%) had reversed E/A ratio. Table 1 shows the mean of the reading in different parameters and the standard deviation for each parameter. In this study population, the duration of hypertension ranged from 2 months to 30 years. We also included 5 newly diagnosed hypertensive patients. Individual analysis 1. Age From the total 50 patients that we have collected, 43 (86%) were patients older than 50 years old while 7 (14%) patients were younger than 50. In the data collected, 22 patients (44%) developed reversed E/A and the remaining 28 (56%) were found to be normal. Of those who were older than 50, 48.8% (21 out of 43) had normal E/A ratio and 51.2% (22 out of 43) had reversed E/A ratio. For those who were equal or younger than 50 years of age, 100% (7 out of 7) had normal E/A ratio. None of them had E/A reversal. The distribution of data was found to be statistically significant, with p < 0.025. (Table 2 and Figure 1) 2. Gender Out of the 23 male patients (46%), 9 of them (39.1%) developed reversed E/A while the remaining 14 (60.9%) had normal E/A ratio. Of the 27 female patients (54%), 13 of them (48.1%) had reversed E/A on echocardiogram while the remaining 14 (51.9%) were shown to be normal. The distribution was not significant in this study. Gender was not shown to be an independent factor in the development of diastolic dysfunction. (Figure 2) 3. Duration of hypertension From the total of 50 patients recruited, 22 patients, or 44% had history of hypertension for more than 8 years, while the remaining 28, or 56% had less or equal to 8 years history of hypertension. Of the 22 patients who had more than 8 years history of hypertension, 6 of them (27%) were noted to have developed diastolic dysfunction, while the remaining 16 (73%) showed normal E/A ratio on echocardiogram. Another 28 patients had had equal or less than 8 years history of hypertension, 16 (57.1%) had reversed E/A ratio, and the remaining 12 (42.9%) were normal. The duration of hypertension was shown to be an independent predictor of diastolic dysfunction (p < 0.05). (figure 3 and table 3) 4. History of previous myocardial infarction or ischemic heart disease From the total of 50 patients recruited, 23 patients, or 46% of them had a history of either ischemic heart disease (IHD) or acute myocardial infarction (AMI), while the remaining 27 or 54% did not give a history of IHD or AMI. Of those with a past history of IHD/AMI, 13 of them (56.5%) did not show abnormality in echocardiogram while the remaining 10 (43.5%) had diastolic dysfunction based on the reversed E/A ratio on echocardiogram. When compared with patients who do not have a past history of IHD/AMI, 15 patients (55.6%) did not have diastolic dysfunction while the remaining 12 (44.4%) were detected by the echocardiogram to have diastolic dysfunction. The difference was not statistically significant (p = 1). (Table 4) 5. Systolic and diastolic blood pressure From the data collected, 19 patients (38%) were within the `normal' or well controlled blood pressure range, 10 of them (20%) had stage I systolic hypertension; another 15 (30%), had stage II systolic hypertension, while the remaining 6 patients (12%) had stage III systolic hypertension. Of those who developed reversed E/A ratio, 1 of them (4.5%) had `normal' blood pressure, 5 (22.7%) had stage I systolic hypertension, another 11 (50.0%) had stage II systolic hypertension and the remaining 5 (22.7%) had stage III systolic hypertension. Of those who had normal E/A ratio, 18 of them (64.3%) had normal range of blood pressure, while the remaining 10 (35.7%) had hypertension according to JNC VI criteria. The distribution was statistically significant, (p < 0.001). The stage of hypertension is shown as a predicting factor in the development of diastolic dysfunction in hypertensive patients. ( Table 5) In the analysis of diastolic blood pressure, 26 patients (52%) were within the `normal' diastolic blood pressure, while another 24 patients (48%) developed various stages of diastolic hypertension. 22 patients (44%) developed diastolic dysfunction as indicated by the reversal of E/A ratio on echocardiogram, while the remaining 28 patients (56%) had normal E/A ratio. The diastolic blood pressure also showed a significant relationship with the development of diastolic dysfunction (p = 0.024, t-test). (Table 6) 6. Treatment with ACE inhibitor From the total 50 patients that we had collected, 23 patients (46%) were on ACE inhibitors as the only or one of the anti-hypertensive agents while 27 patients (54%) were not on any ACE inhibitors Of those who were on ACE inhibitors, 60.9% (14 out of 23) had normal E/A ratio and 39.1% (9 out of 23) had reversed E/A ratio. For those who were not on ACE inhibitors, 51.9% (14 out of 27) had normal E/A ratio while 48.1% (13 out of 27) had reversed E/A ratio. 39.1% (of patients on ACE inhibitors) developed reversed E/A ratio while E/A reversal was seen in 48.1% of those not on ACE inhibitors. There were no significant correlation between the groups although there was a trend in showing that patients taking ACE inhibitors had a lower incidence of diastolic dysfunction (figure 4) 7. Treatment with Beta-blockers From the total of 50 patients, 32 (64%) of them were on beta-blockers while the remaining 18 (36%) were not. Of those on beta-blockers, 56.2% (18 out of 32) had normal E/A ratio and 43.8% (14 out of 32) had reversed E/A ratio. Of those not on beta-blockers, 55.6% (10 out of 18) had normal E/A ratio while 44.4% (8 out of 18) had reversed E/A ratio. 43.8% of those taking beta-blockers developed reversed E/A ratio while this happens in 44.4% of patients not on beta-blockers (p = 1, not significant). The retrospective use of beta blockers in treating hypertension did not have a strong correlation with diastolic dysfunction in the group of study patients. (figure 5) Discussion Age Based on the result of our study, we found out that age was one of the factors that contribute to the development of diastolic dysfunction. Previous studies have shown that as a person ages, the heart experiences a number of changes such as increases in vascular intimal thickness, vascular thickness, ventricular wall thickness and decreased cardiovascular reserved that may affect diastolic dysfunction (3). Age has been shown to have a linear inverse porportion relationship with E/A ratio and diastolic dysfunction in general. Gender This study showed that gender had no significant association with the development of diastolic dysfunction in hypertensive patients. It is not clear what accounts for the differences in cardiovascular disease between the sexes (4). Differences between the sexes are apparent with respect to risk factors, disease manifestations, physicians' management decisions and patient outcomes. Men and women share many risk factors, but their relative importance varies by sex. Disparities in the prevalence of smoking, hypertension, and elevated serum cholesterol in men and women were thought to account for the differences, whereas others suggest that susceptibility to risk factors or the severity or frequency of the disease in men accounted for the increased incidence of heart disease compared with younger women. Women may have protective factors beyond that conferred by estrogen that have not yet been recognized. Duration of hypertension The duration of hypertension seemed to play a role in the development of diastolic dysfunction. Looking at the data, one may find it peculiar to have patients with less than 8 years history of hypertension have higher incidence of developing diastolic dysfunction (Refer interpretation of results). This may contradict the fact that patients with longer history of hypertension tend to have higher incidence of diastolic dysfunction (5). This may be due to the small sample of the patient population, which does not really reflect the true values, as shown in other larger scale study. But, another important issue raised in this finding is, since the patient had already developed diastolic dysfunction with a history of hypertension of less than 8 years, it is essential for the physician to detect the early changes in the heart of hypertensive patients in order for early intervention and prevent late complication of diastolic dysfunction. History of previous Ischemic Heart Disease/Acute Myocardial Infarction In this study, the history of having ischemic heart disease or acute myocardial infarction does not serve as a predictor of development of diastolic dysfunction. It was shown that the development of diastolic dysfunction does not depend on pre-existing IHD or previous AMI. Blood pressure Based on Framingham study, blood pressure is a consistent predictor of the development congestive heart failure (6). In fact, there is a strong and graded association between blood pressure and the incidence of major coronary heart disease manifestations, congestive heart failure, stroke and total mortality (7). From the result of our study, we found out that both systolic and diastolic blood pressure are significant factors that lead to diastolic dysfunction, which is a fore player of development of congestive heart failure. We observed that systolic blood pressure was more strongly associated with diastolic dysfunction than was diastolic blood pressure (8). ACE Inhibitor and Beta blocker as the drug of treatment There are no large-scale, placebo-controlled trials evaluating the efficacy of therapy in diastolic congestive heart failure, as there are in systolic congestive heart failure. It is also clear that medications routinely used in the treatment of systolic dysfunction may have neutral or harmful effects in diastolic dysfunction (9). The goal of drug therapy in diastolic dysfunction is to reduce symptoms by lowering the elevated filling pressures (that is to reduce LV hypertrophy) without significantly reducing cardiac output. Therefore, rate control and maintenance of atrioventricular synchrony and sinus rhythm are crucial. Since diastole is shortened much more than systole as the heart rate increases, slowing down the heart rate allows more time for ventricular filling. Beta-blockers may improve diastolic filling by reducing heart rate. They also relieve myocardial ischemia and cause regression of left ventricular hypertrophy (9, 10). However, owing to the negative inotropic effect, it might cause a reduction in cardiac output. Although using ACE inhibitors in patients with systolic dysfunction is beneficial, their role in patients with normal ejection fractions is less clear. ACE inhibitors reduce afterload, hence controlling the blood pressure and reversing left ventricular hypertrophy. This benefits patients with diastolic dysfunction (11). At the same time, ACE inhibitors also prevent myocardial fibrosis by reducing the amount of angiotensin II (angiotensin II is known to induce myocyte hypertrophy and fibrosis and impair myocyte relaxation) in the heart (9). No significant difference in outcome was noted for patients taking either beta-blocker or ACE inhibitor as far as E/A ratio is concerned. However, the small sample size in this study may not reflect the true picture. More studies are needed before conclusions can be made concerning the use of ACE inhibitors and beta-blockers in patients with diastolic dysfunction. This is because both drugs contribute in reversing left ventricular hypertrophy, yet it is not clear if regression of left ventricular hypertrophy is related to long-term improvement in diastolic function of the left ventricle. Limitations of study We only used one method of assessing left ventricular diastolic function, the E/A ratio of the transmitral pulsed Doppler signal. This ratio is widely regarded as being both insensitive and non-specific as a measure of heart failure, especially when the threshold of 1.0 is used (12). Current guidelines use far more stringent criteria for abnormality (13). In subjects aged over 50 diastolic dysfunction should be considered only if the E/A ratio is <0.5 and associated with an E deceleration time of >280 ms. Another important limitation is that we only had data on a relatively small number of hypertensive patients. A larger scale study should be conducted carefully under strict control before a more definitive conclusion can be drawn. The study may not reflect the true population of hypertensive patients in Malaysia because patients that do not require echocardiography were excluded from the data collection. Acknowledgement We would like to thank Mr. Chiang for his assistance in acquiring the echocardiographs and enlisting patients for us, also nursing staff in the echocardiography unit, Hospital Seremban. Reference:
The following images related to this document are available:Photo images[mj04008t5.jpg] [mj04008t6.jpg] [mj04008t1.jpg] [mj04008f2.jpg] [mj04008t3.jpg] [mj04008f3.jpg] [mj04008f4.jpg] [mj04008f1.jpg] [mj04008t2.jpg] [mj04008t4.jpg] [mj04008f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}