 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 11, No. 1, January 2004, pp. 75-80 The incidence of post-operative deep vein thrombosis in general
surgical patients of Hospital Universiti Sains Malaysia
Myint Tun, Ibrahim Lutfi Shuaib*, Mahayidin Muhamad*, Abdul Hamid Mat Sain and Anas Sjahroeddin Ressang Departments of Surgery and *Departments of Radiology
School of Medical Sciences, Universiti Sains Malaysia, Health
Campus
16150 Kubang Kerian, Kelantan, Malaysia
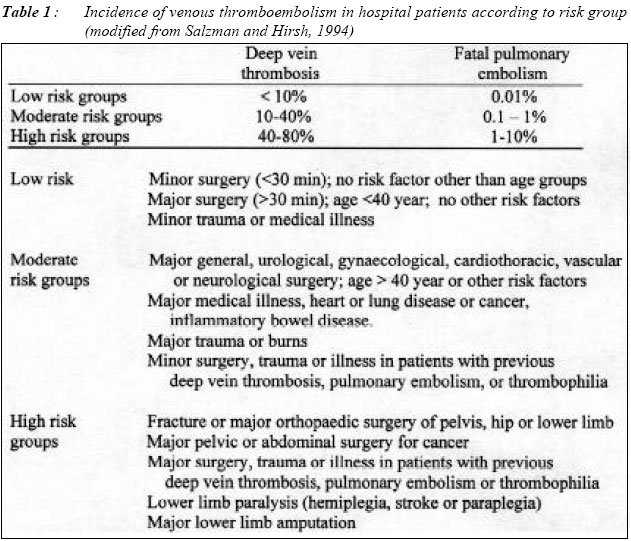
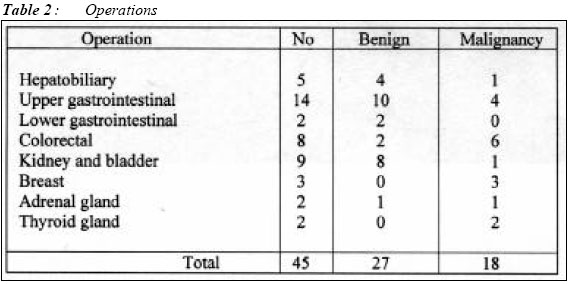
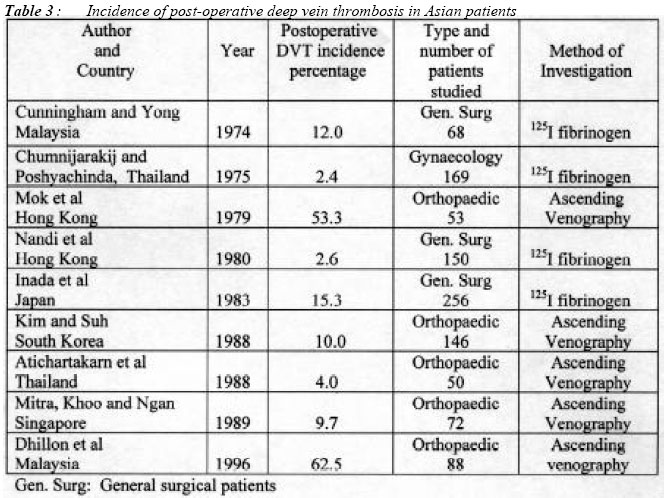
Submitted-10.5.2003 Code Number: mj04009 The incidence of deep vein thrombosis is believed to be rare in Asians. During recent years, a few reports have appeared with high incidence in orthopaedic patients comparable to Western studies. This study was carried out to find out the incidence of post-operative deep vein thrombosis (DVT) after major surgical procedures in general surgical patients in an Asian population. In a prospective study of 45 consecutive Asian patients after major general surgery, colour-flow duplex scan of the legs as an initial screening was done twice within two weeks. Mean age of the patients was 54 years 5 months and 87% of patients were included in the moderate and high risk group for deep vein thrombosis. Ascending venography was used to confirm deep vein thrombosis on patients with equivocal or positive results from colour flow duplex scan. One patient showed positive evidence of post-operative deep vein thrombosis on colour flow duplex scan which was further confirmed by ascending venography; giving an incidence of 2.2%. The incidence of post-operative deep vein thrombosis in general surgical patients is lower than the Western studies. Key words : deep vein thrombosis, post-operative, Asians Introduction Apparent rarity of post-operative deep vein thrombosis and pulmonary embolism in Asians was first reported by Tinckler in 1964 (1). Very few literature and clinical studies are available regarding this problem in Asian population. Study on general surgical patients from 1974 to 1983 revealed a low incidence of postoperative deep vein thrombosis in Malaysia, Hong Kong and Japan (2,3,4). Conflicting results of high incidence in orthopaedic patients comparable to Western figures were also reported from Hong Kong and Malaysia (5,6). This study was carried out in Malaysia with a population of three major ethnic groups as Malay, Chinese and Indian. This well controlled prospective study was done on the post-operative general surgical patients majority of whom were in the group of moderate and high risk to deep vein thrombosis. The study was aimed to determine the incidence of post-operative deep vein thrombosis in general surgical patients of our general population. Since the past few years, ultrasound technology with real time imaging using high resolution duplex ultrasound machines have appeared for detailed visualisation of DVT. Since 1987 several manufacturers have incorporated software that converts the Doppler signals from moving erythrocytes into a coloured real-time image, so called colour-flow Doppler or colour duplex scan. With this addition of colour Doppler to the gray-scale imaging, colour duplex scan has become the primary modality, as a reliable noninvasive method of choice, for initial evaluation and quick recognition of normal and abnormal flow states including those in calf veins (7). This study used the colour duplex ultrasound as a primary screening and evaluation procedure followed by ascending venography for final evaluation on positive and equivocal cases. Patients and Methods This hospital based prospective study from September 1998 to February 2001 included patients aged 25 years and above who underwent major surgery in the general surgical unit of the Hospital Universiti Sains Malaysia. Criteria for inclusion included mastectomy, thyroidectomy, block dissection of the neck, thoracotomy for oesophageal surgery and all laparotomies including those for perforated appendicitis, appendicular abscess and obstructed abdominal hernia. All operations were performed under general anaesthesia with an operating time of more than one hour. The patients did not have any form of DVT prophylaxis as this was not the practice in our general surgical unit. The study was approved by the Medical and Ethical Committee of the Hospital Universiti Sains Malaysia. Informed consent was obtained from each patient after the nature of the study was explained. A completed protocol of each patient included demographic details, nature of the operation, duration of surgery, type of anaesthesia and risk factors. After surgery, the patients were observed daily for clinical evidence of deep vein thrombosis such as leg and ankle swelling, Homan's sign, prominent superficial veins, skin discolouration and fever. The HDI 3500 ATL, USA model colour duplex ultrasound machine was used for the primary evaluation of deep vein thrombosis. On post-operative day 3 to day 7, duplex ultrasound scan of both lower limbs was done by the two Consultant Radiologists (ILS and MM) blinded to each other's findings. Duplex ultrasound scans with same positive or negative reports by the two Radiologists were regarded as adequate scans. The scans were regarded as equivocal if the two Radiologists reported differently or any one of them was inconclusive. Urgent ascending venography was arranged for the patient with adequate positive scan and it was interpreted by consensus by the same two Radiologists. For further accuracy and detection of late onset deep vein thrombosis, patients with equivocal or negative results in first colour duplex scan proceeded to have a repeat scan of both lower limbs in the second week (day 8 to 14) of the post-operative period. Consensus negative reports by the two Radiologists blinded to each other's finding were regarded as true negative for deep vein thrombosis. Bilateral ascending venogram was arranged for patients with consensus positive and equivocal repeat scans in the second week. The result of ascending venogram was again decided by consensus from the same two Radiologists. The same two Consultant Radiologists conducted the scans throughout the whole study period. Results A total of 54 patients were studied. Seven patients had not completed the repeat colour duplex scan and two patients were scanned by only one Radiologist (MM) and were regarded as incomplete scans. These nine patients were rejected from the study. 45 patients, 23 men and 22 women completed the study. 40 were Malay and 5 were Chinese. The age range was 25-78 years with the mean age of 54 years 5 months. Thromboembolic risk factor assessment according to Salzman and Hirsh (8) on the study group of 45 patients showed 39 (87%) patients in the moderate and high risk groups (Table 1). The nature of operations performed is shown in Table 2. All operations were performed under general anaesthesia and the mean operating time (duration of operation) was 2 hours 35 minutes. Only one patient, a 67 year old Chinese man with advanced carcinoma of the sigmoid colon had positive scan for deep vein thrombosis on the third post-operative day. He also developed fever with swelling of the right leg and urgent bilateral ascending venogram showed deep vein thrombosis in the right peroneal vein. 44 patients were subjected to repeat colour duplex scans in the second week and consensus negative results for deep vein thrombosis were reported. The results showed that only one patient with post-operative deep vein thrombosis was detected by preliminary colour duplex scan and confirmed ascending venography. Discussion Thrombogenesis is a complex process and the incidence of deep vein thrombosis varies in different parts of the world for reasons that are not well understood. Complex pathogenesis of venous thrombosis involves the interaction of acquired risk factors with several genetic predispositions, including antithrombin III, protein C, protein S, heparin cofactor II deficiencies, all as a group known as thrombophilias. Silent deep vein thrombosis and consequent fatal pulmonary embolism is still a constant threat to post-operative patients in developed countries of the Western hemisphere. Autopsy proven pulmonary embolism has continued to be a major cause of death. In a United Kingdom study, Sandler and Martin found that 9% of patients admitted to a general hospital died and 10% of these deaths (0.9% of all admissions) were due to pulmonary embolism that originated from the deep veins of the lower limb (9). This study was done in Hospital Universiti Sains Malaysia situated in Kelantan State, on the east coast of Malaysia, where major ethnic group is Malay followed by Chinese, Siamese (Thai) and Indian, thus reflecting a true representation of an Asian population. This study on 45 patients with one positive deep vein thrombosis (2.2%) shows the low incidence of post-operative deep vein thrombosis among our population. The result of the present study compared to other Asian studies is shown in Table 3. The incidence of post-operative deep vein thrombosis in general surgical patients reported in Western studies varies from 33% to 35% (10,11). On the contrary, results of low incidence 2.6% to 15.3% were reported by three Asian studies on using 125I fibrinogen technique (2,3,4). In 1974 in a study from University of Malaya, Cunningham and Yong mentioned that 6 of the 8 general surgical patients who developed deep vein thrombosis suffered from malignant disease as a selected group with high risk to DVT(2). Low incidence of post-operative thromboembolism was reported by autopsy review from Singapore as early as 1968 by Hwang (12). Incidence of post-operative deep vein thrombosis was reported from Thailand as 2.4% on gynaecological patients (13). High incidence of thromboembolism in Asian patients 53.3% to 62.5% comparable to Western figures after hip and knee surgery was reported from Hong Kong and recently from Malaysia (5,6). Even among the orthopaedic patients, it is difficult to explain the low incidence of 4 to 10% after hip surgery in studies from Thailand, Singapore and South Korea (14,15,16). Although low incidence of post-operative deep vein thrombosis among the Asian patients is still contentious in orthopaedic surgical practice, review of various Asian studies shows uniformly low incidence in general surgical patients (Table 3). The cause of difference in incidence of deep vein thrombosis in Afro-Asians compared to Caucasians is still a matter of speculation. Fibrinolytic activity in blood is higher in Africans, Indians and Thais when compared to Western population (17,18,19). The different low nutritional Asian diet with high carbohydrate and low fat may result in change of intestinal bacterial flora activating the production of plasminogen activators from the intestine (20). Recently a hereditary abnormality in coagulation system characterised by poor anticoagulant response to activated protein C (APC) due to the presence of factor V Leiden was reported (21). Analysis of 3380 chromosomes from 24 populations showed allele frequency of 4.4% in Europeans, higher prevalence 7.0% in Greeks and total absence of this chromosome in south east Asians (22). This may partly explain the rarity of thromboembolic disease in Asian population. In conclusion this study shows a low 2.2% incidence of post-operative deep vein thrombosis in general surgical patients of Hospital Universiti Sains Malaysia. The result is comparable to other Asian studies on general surgical patients. This study supports our routine practice of withholding deep vein thrombosis prophylaxis in general surgical patients in Asian population except for a very select group of high risk patients. An attempt to detect the causative factor in this small but highly select group of individuals among Asians would be interesting. Acknowledgements Research project was supported by IRPA short term research grant 391/9636/1036 of Malaysia. References
Copyright 2004 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj04009t2.jpg] [mj04009t3.jpg] [mj04009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}