 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 11, No. 2, July 2004, pp. 26-33 ORIGINAL ARTICLE PSYCHOMETRIC EVALUATION OF THE MEDICAL OUTCOME STUDY (MOS) SOCIAL SUPPORT SURVEY AMONG MALAY POSTPARTUM WOMEN IN KEDAH , NORTH WEST OF PENINSULAR MALAYSIA Wan Mohd Rushidi Wan Mahmud*, Amir Awang**, Mahmood Nazar Mohamed** *Department of Psychiatry, School of Medical Sciences, Universiti Sains Malaysia,
Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Submitted-12.5.2003, Code Number: mj04017 ABSTRACT The Malay version of the Medical Outcome Study (MOS) Social Support Survey was validated among a sample of postpartum Malay women attending selected health centers in Kedah, North West of Peninsular Malaysia. 215 women between 4 to 12 weeks postpartum were recruited for the validation study. They were given questionnaires on socio-demography, the Malay-versions of the MOS Social Support Survey, Edinburgh Postnatal Depression Scale (EPDS) and the 21-items Beck Depression Inventory-II (BDI-II). 30 of the women, who were bilingual, were also given the original English version of the instrument. A week later, these women were again given the Malay version of the MOS Social Support Survey. The scale displayed good internal consistency (Cronbach’s alpha = 0.93), parallel form reliability (0.98) and test-retest reliability (0.97) (Spearman’s rho; p<0.01). The negative correlations of the overall support index (total social support measure) with the Malay versions of EPDS and BDI-II confirmed its validity. Extraction method of the 19 items (item 2 to item 20) from the MOS Social Support Survey using principle axis factoring with direct oblimin rotation converged into 3 dimensions of functional social support (informational, affectionate / positive social interaction and instrumental support) with reliability coefficients of 0.91, 0.83 and 0.75 respectively. The overall support index also displayed low but significant correlations with item 1 which represents a single measure of structural social support in the instrument (p <0.01). The Malay version of the MOS Social Support Survey demonstrated good psychometric properties in measuring social support among a sample of Malay postpartum Malay women attending selected health centers in Kedah, North West of Peninsular Malaysia and it could be used as a simple instrument in primary care settings. Key words : MOS Social Support Survey; validation, psychometric properties Introduction Postpartum depression is one of the most serious but often neglected complications of puerperium (1). Approximately 13% of women experience this crippling mood disorder during the first year after delivery (2). It has been described as a dangerous thief that robs women of precious time together with their infants (3) and wreaks havoc not only on the mothers themselves but their entire families (4). Accurate estimates of the rates and risk factors for postpartum depression are therefore central for the scientific and clinical understanding of psychiatric disturbance during the puerperium, as well as for planning of mental health services for childbearing women and their families (2). The postpartum period is naturally characterized by dynamic changes in a woman’s mental and physical health. This transition to motherhood ushers in many life changes and adjustments as well as new patterns, responsibilities and routines (4). In order to cope with these changes, parents of infants often rely on support of kin and non-kin social networks to varying degrees (5). Availability of social support includes economic, household, or psychological support and this so-called social support system acts as a coping resource in providing both emotional support and task-oriented assistance to the new mothers (6) Social support is a multidimensional construct and the diversity of its measures is matched by the diversity of conceptualizations concerning its ingredients (7). In the area of child rearing, evidence shows that three categories of support are crucial namely affectionate, instrumental, and informational support (8). Affectionate support involves providing empathy, care and trust, whereas instrumental support includes providing the mothers with help with infant/ child care and household tasks. Informational support on the other hand consists of providing information that a mother can use with tasks of infant/child care, self-care and personal and environmental problems. Significant relationship between social support and postpartum depression has been clearly demonstrated in perinatal research. O’Hara and Swain (2) in their meta-analyses of more than 59 studies for example, indicated that social support was a strong negative predictor of postpartum depression. Similarly Beck also found significant association between them. Using r as the effect size indicator (9), the relationship between postpartum depression and social support was in the range of moderate effect size (with mean r ranging from 0.36 to 0.41) (10). Such findings confirmed the results of her earlier meta-analyses (11). In addition, while conducting a systematic review of published scientific literature on postpartum depression, researchers observed that lack of social support is one of the confirmed risk factors of the disorder with agreement from approximately 75% of reported studies (12) In Malaysia, although the area of perinatal research is still at its infancy, social support has already been depicted as an important predictor of postpartum depression. Roziah (13) for example, attested that overwhelming family support during the postpartum period is one of the key factors in protecting Malay women against postpartum depression. This view is shared by a few others (14, 15, 16) but the lack of a user friendly, reliable, general and convenient index of social support was the primary barrier for objective research. None of the previous local studies employed validated instruments and majority relied on simple questions in determining the existence or non existence of such support (17). Medical Outcome Study (MOS) Social Support Survey is one of the most popularly used instruments available in measuring social support (18). It is a brief, multidimensional, self-administered scale initially developed for patients with chronic illnesses (18) but later has been translated, validated and used successfully in perinatal research among Asian Chinese population (19). It covers both structural and functional support and consists of 2 main parts (17). Part 1 (question 1) is a single item structural indicator of social support. It measures the number of close friends and relatives available to the respondents. Part 2 which consists of questions 2 to 20 has 19 items measuring four categories of social support namely (a) informational (b) instrumental (c) positive social interactions (d) affectionate support. The main objective of this study therefore is to evaluate the psychometric performance of the Malay version of MOS Social Support Survey among a sample of Malay postpartum women attending selected health centers in Kedah, North West of Peninsular Malaysia. MethodologyStage I The English version of MOS Social Support Survey was translated into Malay by a group of schoolteachers who were bilingual (Malay and English). Another group consisting of primary care doctors, all well versed in both languages then back translated the Malay version following the usual back-translation technique (20). The finalized version was later pilot tested among 30 postpartum women attending 2 health centers (Bakar Bata Health Center and Jalan Putra Health Center) in Alor Setar, Kedah, North West of Peninsular Malaysia. It was found to be acceptable and no revision was required. In addition, a psychiatrist, a physician, and two medical practitioners also reviewed the instrument to ensure satisfactory face, content, semantic, criterion and conceptual equivalence of the translated instrument as outlined by Flaherty et al (21). Stage II215 Malay postpartum women attending the three selected health centers (Bakar Bata, Jalan Putra and Pendang Health Centers) between the months of May to October 2002 were approached for the validation study. Those who agreed to participate in the study were given the following questionnaires:
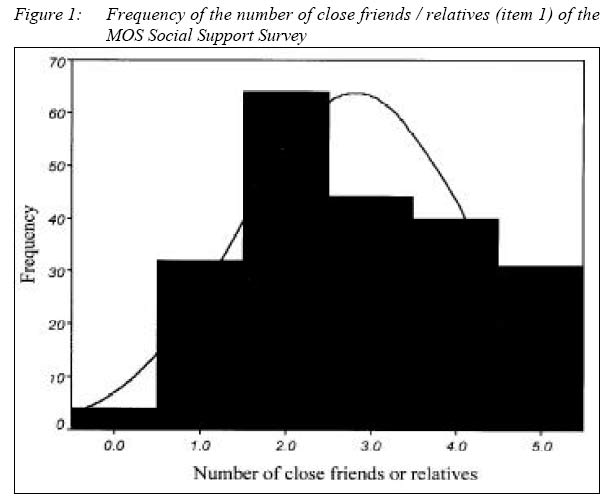
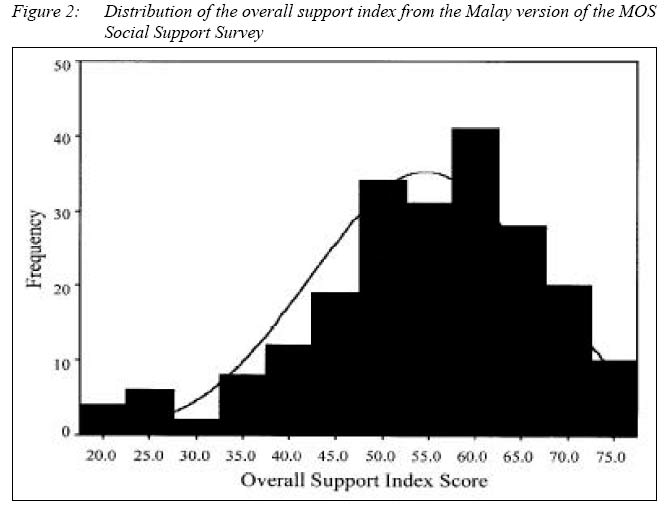
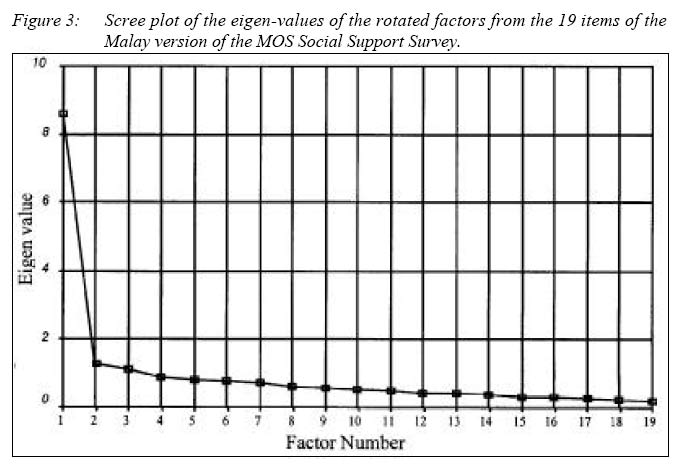
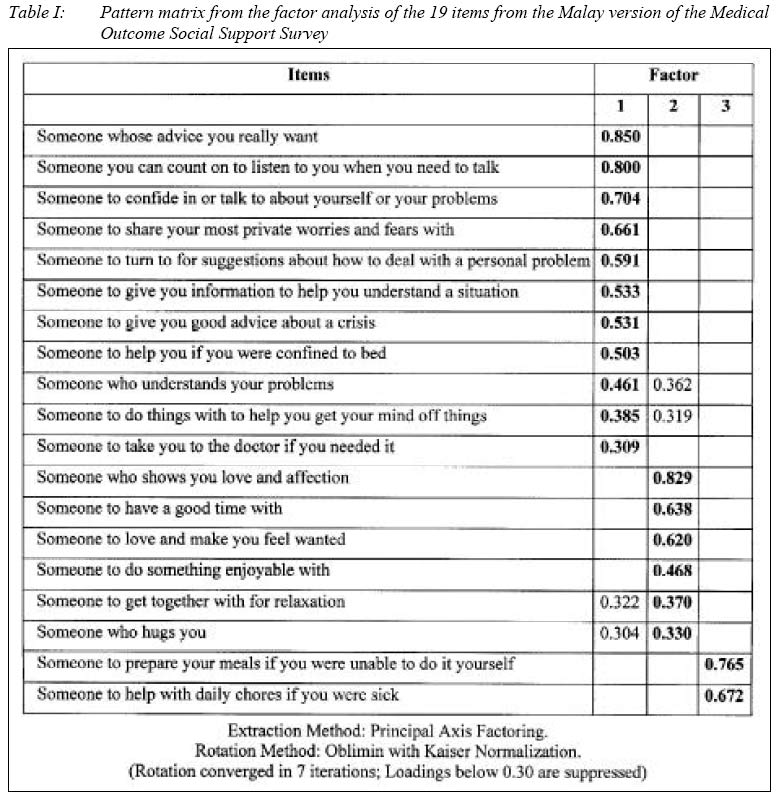
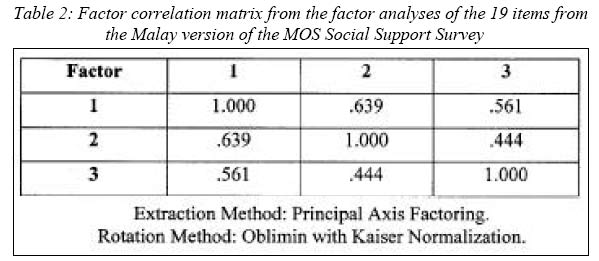
Thirty the participants who were bilingual were also given the English version of the MOS Social Support Survey immediately after the initial assessment. One week later, these women were again contacted and requested to complete the Malay version of the instrument (1 week after the initial interview). Statistical analysesThe results were analyzed using the Statistical Package for Social Sciences version 10.05. ResultsAll 215 Malay women who were approached gave informed consent to participate in the study. All of them were married with a mean age of 29.6 years (standard deviation = 6.19) and median duration postpartum of 42 days (interquartile range = 32 –60). 67.4% were educated at least at SPM level (13 years of school education). All of them were married with a median number of 3 children between them (interquartile range = 2 –4). The median duration of marriage was 6 years (interquartile range = 3 –10). Part 1Item 1 is the single item measure of structural support. The median number of close friends and relatives available for the participants was 3 (interquartile range = 2 –4). Four women (1.9%) indicated that they did not have anyone whom they could feel at ease with and can talk to about what is on their mind. The maximum number of close friends or relatives recorded was 5 in this study accounting for about 14.4% of the participants. Graphic display of the distribution is shown in figure I. Part 2Responses to the 19 functional support items in this study were skewed (figure II) towards the positive end of the distribution (i.e. more frequent availability of support when needed) similar to the findings from the original validation (18). The median score was 56 (inter-quartile range = 48 –64). a) Reliability The instrument showed good internal consistency (Cronbach’s alpha coefficient = 0.93) and split half reliability (unequal length Spearman Brown = 0.91). The alphas for part one (10 items) and part 2 (9 items) were 0.87 and 0.88 respectively. The test-retest reliability measured at time 1 and time 2 (one week after the initial evaluation) showed remarkable stability [test-retest reliability coefficient: Spearman’s rho = 0.97 (2 tailed); p < 0.01]. The instrument also displayed good parallel form reliability (measured by administering the English and Malay versions of the same instrument). The reliability coefficient [Spearman’s rho (2 tailed)] between the two versions administered at time 1 was 0.98 (p<0.01). b) Factor analysisThe Bartlett’s test of sphericity was significant (p< 0.01) and the Kaiser-Meyer-Olkin measure of sampling adequacy for the 19 items scale of the MOS Social Support Survey was 0.92, which Kaiser (24) reported as marvelous. Therefore it is appropriate to proceed to factor analysis. Principle axis factoring with direct oblimin rotation was then conducted on the 19 items and examination of the initial statistics revealed 3 factors could be extracted (eigenvalues > 1.00). These three factors accounted for 50.7% of the variance. The scree plot graphically displayed the eigen-values of each factor and suggested that there was one predominant factor (figure III). The oblique rotation provided a far more interpretable solution than varimax rotation. Based on this rotation, two matrices were produced, a pattern matrix and a structure matrix. The difference between the high and low loadings was far more apparent in the pattern matrix so this matrix was interpreted (table I). The latter also had fewer complex variables and simpler structure. Factor 1 comprised of 11 items with factor loadings ranging from 0.31 to 0.85. Factor 2 comprised of 6 items with loadings ranging from 0.33 to 0.83. Finally factor 3 comprised of 3 items with factor loadings ranging from 0.68 to 0.77. The factor correlation matrix indicated the relationships between these factors (table II) and all factors appeared to be moderately correlated. As mentioned before, the scree-plot (figure III) confirmed the dominance of a single factor represented by 11 items. They represented a conceptually distinct aspect of social support equivalent to the original validation, namely the informational support. The next six items corresponded to a combination of two factors from the original validation namely the affectionate support and positive social interaction. Instrumental support was represented in the final subscale consisting of only two items. Internal consistencies (Cronbach’s alphas) for each of the subscales (informational support, affectionate support / positive social interaction and instrumental support) were 0.91, 0.83 and 0.75 respectively. It should be noted that two items (someone to help if confined to the bed and someone to take to the doctor), which displayed high factor loadings in the instrumental support subscale in the original validation, had higher loadings on the informational support subscale in this study. Furthermore item 14 (someone to do things with to help you get your mind off things), which did not discriminate well in the latter, also have significant loading on the same subscale in this study. c) ValidityTable III presents the Spearman’s correlations between the functional social support measures, the single item measure of structural support and the participants’respective scores on the Malay versions of the BDI-II (22) and EPDS (23). There was also a low but significant correlation between the single item measure of structural support with the overall support index (0.21) (p<0.01). Depression scores of the postpartum women on the Malay versions of BDI-II (22) and EPDS (23) showed negative correlations with the social support measures (i.e. the higher the social support measures, the lower the depression scores). All these correlations were again significant at p < 0.01. Summary and DiscussionThe above data suggest that the MOS Social Support Survey is a useful instrument for measuring social support among recently delivered Malay women attending selected health centers in Kedah, North West of Peninsular Malaysia. It measures the most essential aspects of social support, the perceived availability, if needed of the various component of functional support; and appears to be easy to understand and administer among Malay postpartum women. Overall, the psychometric performance of the instrument is quite impressive both in terms of reliability and validity. The internal consistency was high (Cronbach alpha = 0.93) indicating a high level of homogeneity among items in the scale. Parallel form reliability was also high (Spearman’s rho = 0.98; p < 0.01). In addition, test-retest reliability coefficient assessed after 1-week interval was 0.97 demonstrating its remarkable stability. The validity of the instrument was demonstrated through the significant negative correlations between overall support index of the instrument and all its components (informational, affectionate / positive social interactions and instrumental support) to two validated measures of depression among the same population in Malaysia, namely the BDI-II (22) and EPDS (23). Such findings correspond to the earlier results from various studies on the relationship between social support and postpartum depression (2, 9, 10). Factor analyses of 19 items from the MOS Social Support Survey generated 3 dimensions as opposed to 4 in the original validation (18). The affectionate support and positive social interaction components converged into one dimension of functional support in this study. 2 items formerly from instrumental support dimension and item 14 which did not discriminate well in the original validation (18) loaded significantly higher in the informational support factor. Only 2 items loaded highly on measures of instrumental support in this study namely someone to help prepare meals and someone to help with the daily chores. Confirmation of the reliability of the each of the subscales was provided by their high internal consistencies (Cronbach’s alphas), which were 0.91, 0.83 and 0.75 for informational, affectionate / positive social interaction and instrumental support respectively. Overall the Malay version of MOS Social Support Survey displayed good psychometric performance in measuring social support among recently delivered Malay women attending selected health centers in Kedah, North West of Peninsular Malaysia. It has good reliability and validity and able to detect and measure all the main components of social support so crucial in child rearing namely the affective, instrumental and informational support (8). This scale could therefore be used as a simple screening instrument particularly in primary care settings. AcknowledgementsWe would like to thank the women who participated in this study and all the staff from Bakar Bata, Jalan Putra and Pendang Health Centers for their cooperation and assistance. References
© Copyright 2004 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj04017t2.jpg] [mj04017f1.jpg] [mj04017t3.jpg] [mj04017f2.jpg] [mj04017t1.jpg] [mj04017f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}