 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 11, No. 2, July 2004, pp. 52-58 ORIGINAL ARTICLE MEDICATION ERRORS AMONG GERIATRICS AT THE OUTPATIENT PHARMACY IN A TEACHING HOSPITAL IN KELANTAN Dellemin Che Abdullah, Noor Shufiza Ibrahim, Mohamed Izham Mohamed Ibrahim* Hospital Universiti Sains Malaysia, Universiti Sains Malaysia, Health Campus,
16150 Kubang Kerian, Kelantan, Malaysia. *School of Pharmaceutical Sciences,
Universiti Sains
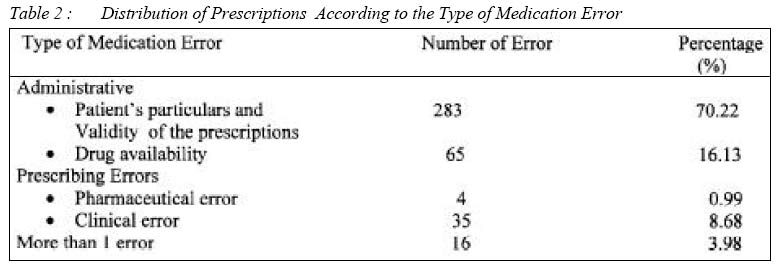
Malaysia, Pulau Pinang, Malaysia Submitted-18-2-2003, Code Number: mj04020 ABSTRACT The main aim of this study was to determine the medication errors among geriatrics at the outpatient pharmacy in a teaching hospital in Kelantan and the strategies to minimize the prevalence. A retrospective study was conducted that involved screening of prescription for a one-month period (March 2001). Only 15.35% (1601 prescription) of a total 10,429 prescriptions were for geriatrics. The prescriptions that were found to have medication errors was 403. Therefore, the prevalence of medication errors per day was approximately 20 cases. Generally, the errors between both genders were found to be comparable and to be the highest for Malays and at the age of 60-64 years old. Administrative errors was recorded to be the highest which included patient’s particulars and validity of the prescriptions (70.22%) and drugs that available in HUSM (16.13%). Whereas the total of prescribing errors were low. Under prescribing errors were pharmaceutical error (0.99%) and clinical error (8.68%). Sixteen cases or 3.98% had more than 1 error. The highest prevalence went to geriatrics who received more than nine drugs (32.16%), geriatrics with more than 3 clinical diagnosis (10.06%), geriatrics who visited specialist clinics (37.52%) and treated by the specialists ( 31.07%). The estimated cost for the 403 medication errors in March was RM9,327 or RM301 per day that included the cost of drugs and humanistic cost. The projected cost of medication errors per year was RM 111,924. In conclusion, it is very clear that the role of pharmacist is very great in preventing and minimizing the medication errors beside the needs of correct prescription writing and other strategies by all of the heath care components. Key words : medication errors, geriatrics, prescription screening, pharmacists, strategies to minimize Introduction Drug therapy in the health care system is not static but is a dynamic process. The introduction of new drugs in the market not only makes the therapy more sophisticated but also become complicated. However, this situation sometimes may lead to several problems in medication. Medication problem is potentially tragic and costly in both human and economic terms, for patients and professionals alike. Some will cause death to the patients. Statistics from a 1998 Journal of the American Medical Association reported that, approximately 106,000 deaths occur annually from medication, making adverse drug reaction (ADRs) the number 4 to 6 leading cause of death in the United States; and over 2 million serious ADRs (defined as requiring hospitalization or causing permanently disability or death) occurs each year(1). In health care setting, there are many problems regarding drugs administration which includes administering the wrong drug, strength of the drug, or drug dose, confusion over “look-alike” and “sound- alike” drugs, incorrect routes of administration, miscalculations, misuse of medical equipment, as well as errors in prescribing and transcription. Report in the professional literature and lay press highlighted the humanistic and economic impact of medication problems. Medication problems can lead to patient morbidity or mortality, and because drugs are used so frequently, the number of preventable injuries are substantial (2). The American Hospital Association lists some common types of medication problems such as incomplete patient information, unavailable drug information, miscommunication of drug orders, which can involve poor handwriting, confusion between drugs with similar names, misuse of zeroes and decimal points, confusion of metric and other dosing units, inappropriate abbreviations, lack of appropriate labeling as a drug is prepared and repackaged into smaller units, environmental factors, such as lighting, heat, noise, and interruptions that can distract health professionals from their medical tasks (3). On the other hand, medication errors represent only one of the many types of medication related problems. The potential for adverse drug events and medication errors is a reality. They occur in all parts of the medication use system, of which prescribing and administration reportedly account for a majority of the errors(4) Medication error is defined as any preventable event that may cause or lead to inappropriate medication use or patient harm, while the medication is in the control of the health care professional, patient, or consumer. Such events may be related to professional practice, health care products, procedures, and systems, including: prescribing; order communication; product labeling, packaging, and nomenclature; compounding; dispensing; distribution; administration; education; monitoring; and use (5) Medication error is not a new problem faced by the healthcare team. In fact, studies by Leape and colleagues reported 3.7% of hospitalized patients experienced clinically significant adverse events, with drug complications reported as the most common single type of adverse event (19%) (6,7). Henri Manasse, Executive Vice President of the American Society for Health-System Pharmacists, forecasted over a decade ago that drug-related morbidity and mortality or “drug misadventure,”represented very serious medical problem and deserved consideration as an issue of public policy (8,9). Johnson and Bootman further analyzed the scope of the medication-related problem. They reported that the number of drug-related hospital admissions ranges from 3.5 million to 8.8 million annually, which corresponds to a hospitalization rate of 11.3% to 28.2% (10,11). Medication errors can be classified as two main types, prescribing errors and medication administration errors In addition to under treatment, other medication-related problems which occur in geriatrics could involve improper medication selection, too much or too little medication, failure to receive medication, adverse drug reactions, drug interactions, and medication use with no indication (12) Two studies conducted in New York and in Colorado and Utah (13). The 1991 New York study reported that adverse events due to medical errors occurred in 3.7% of hospitalized patients, with 13.6% of the adverse events actually leading to death. In the Colorado and Utah study, adverse events occurred in 2.9% of hospitalizations, with 8.8% of these resulting in death. Extrapolation of these data implies that between 44,000 and 98,000 patients die each year as a result of medical errors, with an estimated overall cost to society of between $17 billion and $29 billion (14). Therefore, this study was done to determine the prevalence of medication errors among geriatrics in Hospital Universiti Sains Malaysia. As a part of economic aspect, the expenditure loss due to medication errors would be evaluated. Finally, this study will identify the strategies to minimize the medication errors. The study was conducted retrospectively at the outpatient pharmacy department of Hospital Universiti Sains Malaysia, Kelantan. All the prescriptions for the one-month period (March 2001) were audited and prescriptions that involved geriatric patients were selected and screened. All the data were collected using a form. The cost of drugs that been involved in this mediation errors was calculated. Drug errors were discussed with the doctor in charge. One-month study was done due to time limitation. Results Demographic Data In March 2001, 10,429 prescriptions were screened at the outpatient pharmacy (from various clinics) and from that amount 1,601(15.35%) are for geriatrics. About 403(25.17%) from the whole geriatrics prescriptions had medication errors. Therefore, the prevalence of medication errors that can be generated from this data was 25.17% which was approximately 20 cases per day excluding public holidays. This study showed that the prevalence of medication errors occurred was almost equal between male and female patients while based on race, Indian patients recorded the highest prevalence. Patients at the age 60 to 64 years old had also showed the highest case of having medication errors (Table1) Medication Errors DataMedication errors were divided into 2 categories (Table 2). The first category was problem in administrative that could be divided into two aspects. The first aspect that contributed 70.22% of the total medication errors was regarding patient’s particulars and validity of the prescriptions that involved miswriting either one or more of the particulars like, patient’s name, registration number, date, age, gender, weight/height, ward/clinic, diagnosis and prescriber’s signature (Table 3) Another aspect was drug availability in HUSM. Some drugs could not be dispensed that contributed 16.13% of the total medication errors were because of non-standard drugs not listed in HUSM formulary, drugs that were nil in stock either standard or sample and drugs that were restricted to be prescribed by the specialists only . Another category was prescribing errors which included pharmaceutical and clinical problems. Only 4 cases or 0.99% involved in pharmaceutical error which included dosage form, active ingredient, stability and appropriateness, as well as method and special techniques. While the clinical errors were, drug allergy, polypharmacy, drug-drug interactions, drug-disease interactions, inappropriate dose and interval, duplication of drugs, inapproriate drug regimens and no clear medical indication. Sixteen cases had more than 1 error either administrative errors only or prescribing errors only or both. Economic DataThe cost of drugs that involved in medication error was RM8,134. In order to determine the actual cost, the humanistic cost was also included. It consisted the total salary for pharmacists, pharmacy assistants and attendants which was RM30,900 per month and RM2.96 per prescription. Since only 403 prescriptions involved in medication error the humanistic cost that been included was RM1,193. Therefore, it brought to the actual cost of medication error up to RM9,327 in March and RM301 per day. If the percentage of medication error was assumed to be equal in all month, the extrapolated cost of medication error was RM111,865 per annum DiscussionIn this study, Malays geriatrics were recorded as the highest involved in medication error. However, the prevalence was highest among Indians since they are a minority race but the medication errors often occurred. Even though the highest percentage of medication errors are administrative errors, it should not be neglected. For example, patients’particulars are very important to ensure that the prescription belonged to the right person. Therefore, the medication would be dispensed to the patient indicated. Validity of the prescription is another important aspect to determine the prescriptions are written by the legal persons. This indicates a need for pharmacy and medical educators to further emphasize the importance of writing clear and complete prescriptions (15). In this study, miswriting the diagnosis as a part of administrative errors was reported as the most frequent (73.8% or 277 cases). Therefore, the screening processes were done by assuming the medication prescribed were indicated to the patients. However, before the medications were dispensed, the person who dispensed would asked the patients their problem or diseases in order to confirm either the medications prescribed matched or not to the patients. Part of prescribing error, miswriting the drug interval such as for tablet Metoprolol
100mg (no interval) and duration of the treatment like Tablet Erythromycin
Ethyl Succinate 400mg bd (without duration), become as one of the pharmaceutical
aspect that had the highest prevalence. Whereas, most of the clinical errors
involved drug over dose such as tablet Daonil® was prescribed more than
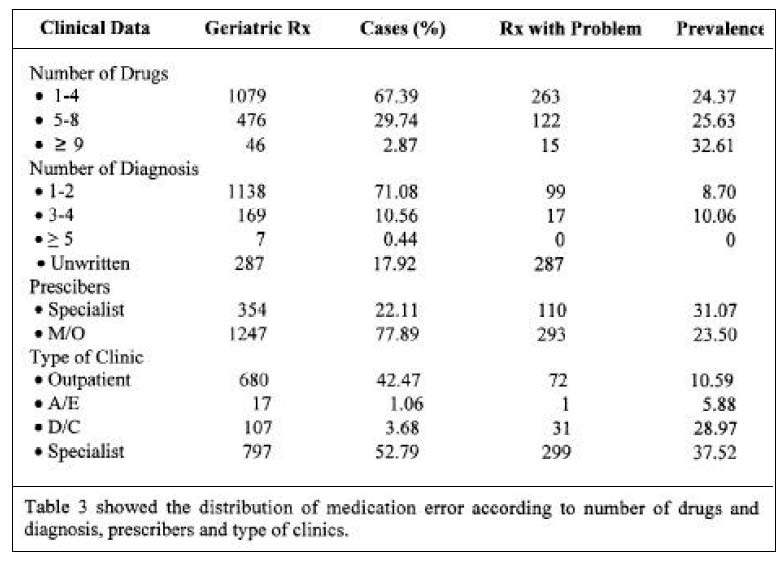
20mg per day ( 10 mg tds). The incidence of death and serious harm caused by mistakes and accidents in medication problem is unacceptable. The patients have their right to receive correct medical treatment. Thus, the responsibilities and the role of screening prescription by the pharmacists should not be denied and they should actively involve in identifying and resolving any medical errors. The number of drugs between 1-4 was the most prescribed. As the number of drugs increased, the potential for medication errors occur might also increase. Study showed that, geriatrics were likely to have more than one diagnosis and drug. This situation might lead to more complication to the geriatrics if medication errors occur. Probably medications are the single most important factor in improving the quality of life for geriatrics but this population remains vulnerable to medication error due to: (i) Physiological changes associated with aging as for vital organs like renal function; (ii) Higher incidences of multiple chronic diseases and conditions like hypertension, diabetis mellitus and chronic obstructive pulmonary disease; (iii) Greater consumption of prescription and over the counter medication. Medication errors still remain as the critical problem to handle. The healthcare team consist such as prescribers, pharmacists ,nurses and pharmacy assistants should give special attention and should use their capability to minimize this errors .Estimated 1-2% patients admitted to the U.S. Hospital are harmed as a result of medication problems (16) and each problem results in additional US$5,000 cost, excluding legal cost (17). The Institute of Medicine (IOM) reports that 44,000 to 98,000 patients die each year as a result of medical error (18). Pharmacists are the important part of the risk versus benefit assessment process, because we see patients when they get new prescriptions filled and any time they return for refilled. During these interactions, assessment of potential medication problems is possible. At outpatient pharmacy, the pharmacist should thoroughly check the prescriptions before dispensing the drugs. By this way, any medical problems can be detected. However, it needs the pharmacists to spend all their time by doing the screening process. While the pharmacy is the only place for patients to get their medication , the manually screening process might no longer be suitable in the future. The use of computerized system is looked as the way that benefits both patients and pharmacists. Managerial level are urged to give attention because computerized system will be able to do screening process in a short time that make the job more efficient. Strategies to reduce the incidence of medication problems frequently point to the positive use of technology equipment. Some medical centers (especially in western country such as US) have begun using computer programs and other system supports to curtail medical mishaps by double-checking the care decisions doctors and nurses make. Even simple computer systems that use electronic prescriptions in place of handwritten ones have in some cases already paid off with substantial error reductions. Hospital in the Department of Veterans Affairs, long notorious for serious lapses in medical safety, are now adapting bar-coded medication and identification strips and wireless computer technology after a study at two(2) VA hospitals in Kansas found these devices reduced medication error rates by 70% over a five-year period (19). In some cases different doctors prescribe same medication (as previous doctor gave) to the same patient. These situation not only waste the drugs cost but also, it can be harmful to the patients health. Therefore, beside technological advances, doctors have their roles too. By checking patients’mediations profile and past medication history before prescribing also could avoid or at least minimize medical errors. Another way to minimize this problem is by regulating standard prescription writing by using generic name and standard abbreviation. This will avoid any confusion to the pharmacist in order to interpret the doctors’handwriting. By using standard drugs name and abbreviation it can avoid sound-alike and look-alike names. The FDA saw this situation as a big problem. FDA is developing new standards to prevent such name mix-ups, as well as to prevent confusion between similar-looking drug packaging(20). However, the implementation of electronic prescribing will probably eliminate some of these problems (15). Other aspect, which also can reduce medication problems is patients’awareness about their medication. In order to make them aware, education is very important. If patients concern what they are taking for their diseases, any changes to their medication supply can be detected immediately. In order to do so, counseling is thought as the best approach. Since patients are geriatrics this strategy however might not be effective. Alternatively, pharmacists could counsel the patients together with their family members. By this way, they can prevent medication problems by being vigilant about the health-care, understanding the treatment, keeping organized records of what doctors they see and what medications they take and asking questions when things don’t seem right. Another aspect that can reduce medication problem is to encourage participation of pharmacists during ward rounds. The availability of improved communications with pharmacists, pharmacists on patient care units, pharmacists on patient care rounds, drug information services, and pharmacists as drug therapy consultants have consistently demonstrated improved patient outcomes and cost-effectiveness. Thus, to enhance and update their knowledge the pharmacists should encourage themselves to attend the continuous pharmacy education(CPE), conferences and courses. As for that all organization and individual healthcare providers should cooperate towards improve the utilization of these valuable resources. ConclusionThe study concluded that medication errors are still polemic for healthcare team because of its impact clinically and economically. It demands ongoing and vigorous attention for a long time. This indicates that the importance of correct prescription writing by prescribers and prescription screening by the pharmacists. However, other strategies to reduce medication errors still continue to minimize the prevalence of medication errors. Further study should be carried out in order to explore in depth about medication problems situation in the hospital. AcknowledgementsThe authors wish to thank the staff of the Outpatient Pharmacy Unit and Aseptic Dispensing Unit, Hospital Universiti Sains Malaysia for their assistance and cooperation. References
The following images related to this document are available:Photo images[mj04020t3.jpg] [mj04020t1.jpg] [mj04020t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}