 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 11, No. 2, July 2004, pp. 59-64 ORIGINAL ARTICLE A DESCRIPTIVE ANALYSIS OF EXERCISE TOLERANCE TEST AT SEREMBAN HOSPITAL : AN AUDIT FOR THE YEAR 2001 Abdul Latiff Mohamed, Chan Chee Nee, Ahmed Azzad International Medical University,
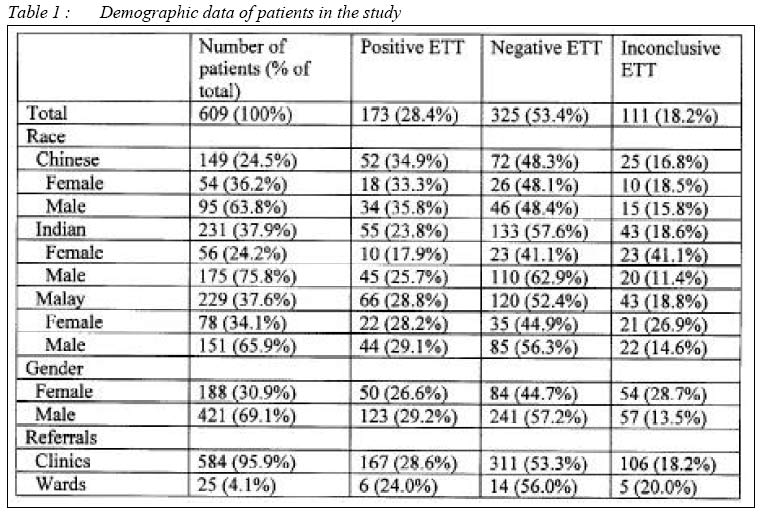
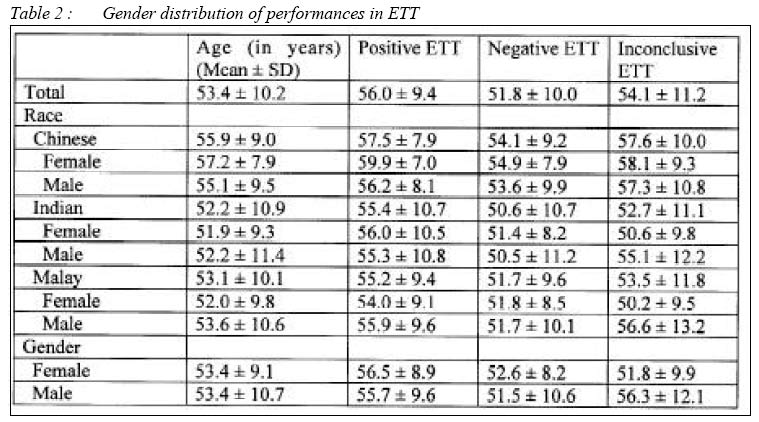
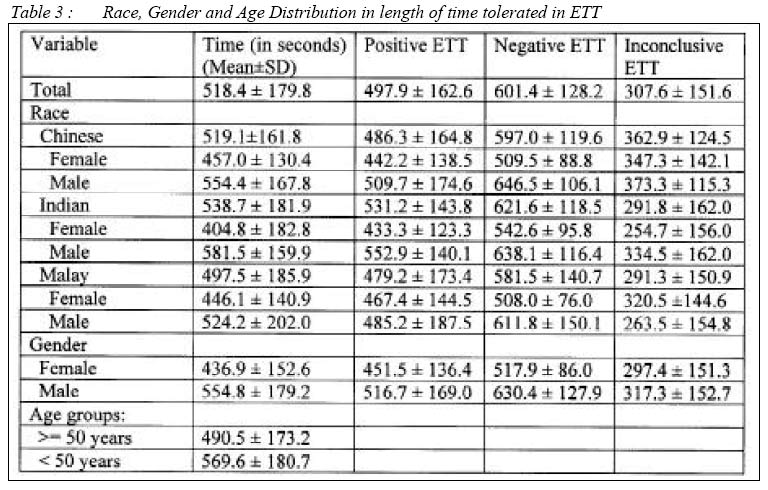
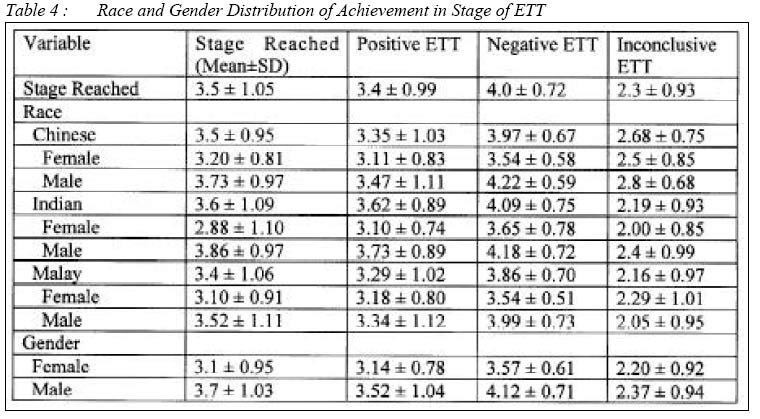
Clinical School, Seremban, Negeri Sembilan, Malaysia. Submitted-27.3.2004, Code Number: mj04021 ABSTRACT Our purpose is to report on the epidemiological variables and their association with the results of the exercise tolerance test (ETT) in the series of patients referred for standard diagnostic ETT at Seremban Hospital during the year 2001. ETT is widely performed, but, in Malaysia, an analysis of the associations between the epidemiological data and the results of the ETT has not been presented. All patients referred for ETT at Seremban Hospital who underwent exercise treadmill tests for the year 2001 were taken as the study population. Demographic details and patients with established heart disease (i.e. prior coronary bypass surgery, myocardial infarction, or congestive heart failure) were noted. Clinical and ETT variables were collected retrospectively from the hospital records. Testing and data management were performed in a standardized fashion with a computer-assisted protocol. This study showed that there was no significant predictive epidemiological variable on the results of the ETT. However, it was found that there was statistically significant difference between the peak exercise time of males and females undergoing the ETT. Key words : Exercise Tolerance Test, Race, Gender, Age Introduction Exercise, a common physiological stress, can elicit cardiovascular abnormalities that are not present at rest, and it can be used to determine the adequacy of cardiac function.(1) Three types of muscular contraction or exercise can be applied as a stress to the cardiovascular system: isometric (static), isotonic (dynamic or locomotor), and resistance (a combination of isometric and isotonic).(2, 3) Oxygen uptake quickly increases when dynamic exercise is begun or increased.(4) During staged exercise testing, oxygen uptake usually remains relatively stable (steady state) after the second minute of each intensity of exercise below the ventilatory threshold. Maximal oxygen consumption (VO2 max) is the greatest amount of oxygen a person can take in from inspired air while performing dynamic exercise involving a large part of total muscle mass.(5) There are many different exercise protocols available and the Bruce protocol is the most frequently used protocol in Seremban hospital. The advantages of the Bruce protocol are its use in many published studies and the value of 3-minute stages to acquire submaximal data. Its disadvantages are large inter-stage increments in work that can make estimation of VO2 max less accurate and a fourth stage that can be either run or walked, resulting in different oxygen costs. Some subjects are forced to stop exercising prematurely because of musculoskeletal discomfort or an inability to tolerate the high workload increments thus increasing those with inconclusive ETT results.(1, 17) Exercise tolerance testing (ETT) is often considered the opening gambit in the diagnosis of ischaemic heart disease. The purpose of this report is to provide an overview of relevant epidemiological background of patients who have undergone ETT and its correlation with their results in the setting of an average government hospital in Malaysia. To date there has been no data in Malaysia on this subject and we feel that it provides the examiner a fresh perspective of what to expect from patients referred for ETT. MethodsPopulation There were 701 patients who underwent ETT at Seremban Hospital for the year 2001 and all were selected for the study. Patients who were subjects in using the modified Bruce protocol (7 patients) were not considered in the analysis. The other 85 patients were excluded due to incomplete information and unavailability of results. The remaining 609 patients who were included as the study population. Referrals were from the clinics and the wards. Data collectionResults of the ETT conducted were recorded by the hospital staff in a central log-book. Each patient referred to cardiology lab for ETT had his or her name, age, sex, race and registration number noted. Also included were the source of referral (ward or clinic), the attending physician responsible for the referral, reason for referral and the protocol used in the ETT. The duration of the test was noted upon completion of the ETT. This log-book was used as the reference of patients used in the study. Data was cross-referenced with patient records for verification to rule out any error in data recording. Exercise testingPatients underwent a standardized ETT using the Bruce protocol. The tests were conducted in the presence of trained allied health personnel with the results being interpreted by medical officers of the Internal Medicine Department of Seremban Hospital. The equipment used for the exercise stress tests include a Max-1 Marquette Advanced Exercise System by Marquette Electronics Incorporated and an Accuson Manual Standing sphygmomanometer. Statistical AnalysisSPSS for Windows Release 9.0.0 was used for all statistical analysis after the data was transferred from an EXCEL (Microsoft) Spreadsheet. Data is presented as mean ± standard deviation. Two-tailed Student t-test was used to compare the peak exercise time between genders in different races and 2 age groups (above 50 years and below 50 years of age). The results are deemed significant when the p value was less than 0.05. Results Population demographics The mean age of the subjects were 53.4 (± 10.2) years. 69.1% (421) were males and 30.9% (188)were females. There were 37.9% Indians, 37.6% Malay and 24.5% Chinese. Out of these, 95.9% were referrals from the clinics and 4.1% referrals from the wards. ETT results There were 53.4% negative results of the ETT and 26.4% Positive results and the remaining 18.2% inconclusive results. (Table 1) Three hundred and thirty (54.2%) of the patients were referred for ETT for a cardiac assessment. Two hundred and seventeen (35.6 %) were referred for assessment of IHD. Other reasons include assessment for post myocardial infarction, assessment of angina, and assessment for post coronary artery bypass grafting, hyperlipidaemia and others which all add up to the remaining 10.2% of referrals. (Table 2, 3, 4) The mean peak exercise time of ETT is 518± 180 seconds (8 minutes 38 seconds ± 3 minutes). There is no statistically significant correlation seen in the age of the patient and the peak exercise time of ETT. There was no correlation between peak exercise time and the different results (inconclusive, negative or positive) of the ETT. There were no difference between the peak exercise time in the different races (Chinese, Malay or Indian) and between the different gender. However, the peak exercise time of males is greater than that of females and males tend to have a greater range of time (spending longer time undergoing the ETT) than females. Comparing the peak exercise times of the two sexes and the races show that males tend to have a higher peak exercise time (555 ± 179 seconds) than females (437 ± 153 seconds) in general (not statistically significant). The t test comparing the average times of patients of different age groups shows that there was no statistical difference between the age group greater or equal to 50 years old and the age group less than 50 years old. 43.7 % of the patients reached stage 4 Bruce protocol. There was no statistically significant difference in the races and the stages reached. On further analysis, it was found that the mean difference of stages among the males and females was only different in the Indian subjects, where the males reached an average of one stage higher (stage 4) than their female counterpart (stage 3). DiscussionBackground ETT is widely performed, but an analysis of the associations between the epidemiological data and the results of the exercise stress test has not been presented for a large number of consecutive tests performed on patients referred for assessment of cardiac disease in Malaysia. As with any noninvasive tests of cardiovascular function, this test is not very sensitive and is subjected to pre-test and post-test bias as compared with the gold standard of coronary angiography. (10, 11, 13) However, it is highly specific in a given population and provides incremental gain in estimating disease likelihood in individual patients. There are also gender-based differences in the accuracy of test results, which suggest that test results must be analyzed in a gender-specific fashion and that the decision to proceed to invasive tests must take into account gender-based differences in measures of test accuracy. (6, 7, 8, 9, 14, 15) We intend to find out if there is any epidemiological data that would in any way influence the results of the ETT and in knowing such recommend these as guidelines for ETT referrals to increase the sensitivity of the ETT. Population DemographicsMalaysia is a multi-racial country. It presents itself in a unique position
to see if there is any difference in results of the ETT in different races.
The sample from our population has a good balance of the three major races
in Malaysia all of which contributes to the significance of this study. Surprisingly,
majority of the referrals were from the clinics and very few are from the wards. It was found that there was no statistically significant effect of time in the two genders, and the time was not a good predictor of the results of the ETT. However, it was shown that the patients who had inconclusive ETT results generally did not spend enough time on the test (did not achieve target heart rate). Patients with positive ETT results had to undergo the test for a longer time (until the target heart rate is reached) before knowing that the result is positive or negative. Males tend to be able to undergo the ETT for a longer period of time as compared with the female counterpart. We found that there was evidence to show that males and females had different average times by means of a t-test. This is true for the Indians and Malays, but not for the Chinese. The results from the ETT stage attained showed a similar picture. Because both results are based on the same thing, and the time taken being more sensitive, these results serve to confirm our previous results rather than add to it. The t-tests done showed that the average time between the two were not statistically significant for either group (arbitrarily split at 50 years). LimitationsThe major limitation of our study is that much of the data was not standardized. (16) Many physicians interpreted the results of different patients and we made the assumption that they followed the standard guidelines for interpreting the results of the ETT. Much of the personal data of the individual patients were not available, thus some factors that could potentially affect the results of the stress test were possibly excluded from the study. These factors could be the BMI of the patient, the dietary habits of the patient, whether or not the patient exercises frequently, the variation in room humidity and temperature and so on. (1, 12) Another limitation was setting the objectives too wide. The objectives could have been narrowed down to patients in of a certain gender in a certain age group with certain characteristics and then comparing each with each other. This was not possible due to the limited number of patients and also some information not being present. This problem could have been addressed by using multiple centres. Having said all that, this being a pilot study, it is good to have identified potential problems that can arise from such a project and steps to correct these problems can be taken in the future. While not giving substantial authoritative information about our objective of finding whether there is a relationship between the patients referred for ETT and the epidemiologic data, it has served its purpose in finding out some of the potential problems and results that might arise if a similar project on this subject would be planned on a greater scale. ConclusionThis study has shown that there was no significant predictive epidemiological variable on the results of the ETT. However, it showed that males were able to reach a longer exercise time on the Bruce protocol compared with their female counterpart. AcknowledgementsThe authors of this study would like to acknowledge the assistance given by Mr. Chiang, senior medical assistant of Seremban Hospital Cardiology Laboratory, and his staff who assisted in the data collection. We would also like to acknowledge the management and staff of Seremban Hospital for kindly allowing us the opportunity to conduct this study in their premises. References
© Copyright 2004 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj04021t4.jpg] [mj04021t3.jpg] [mj04021t1.jpg] [mj04021t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}