 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
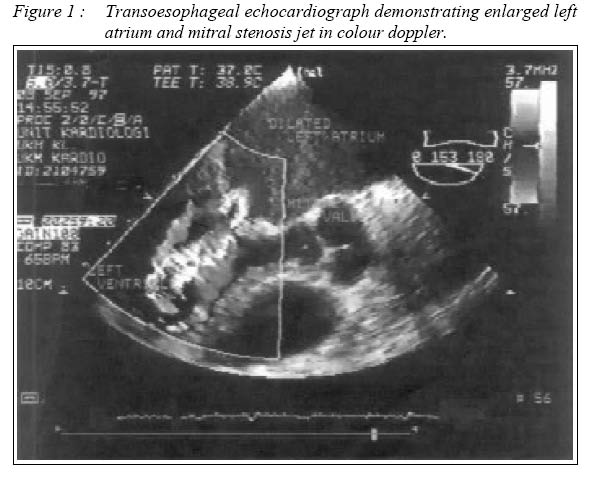
Malaysian Journal of Medical Sciences, Vol. 11, No. 2, July 2004, pp. 65-68 CASE REPORT HOARSENESS OF VOICE IN A PATIENT WITH MITRAL STENOSIS AND ORTNER’S SYNDROME Abdul Latiff Mohamed, Mollyza Mohd Zain Department of Medicine,
Hospital Universiti Kebangsaan Malaysia,
Jalan Tenteram, Bandar Tun Razak,
56000 Cheras, Malaysia. Submitted-27.3.2004, Code Number: mj04022 ABSTRACT Rheumatic mitral stenosis is prevalent in this part of the world and it gives rise to wide array of manifestations. However, hoarseness of voice secondary to recurrent laryngeal nerve paralysis (Ortner’s syndrome) is an uncommon manifestation. This case illustrates an uncommon presentation in a common disease. A 29-yearold lady presented with a 2-year history of hoarseness of voice. Physical examination revealed a mid-diastolic murmur and left vocal cord paralysis. Echocardiography confirmed mitral stenosis with pulmonary hypertension. She underwent percutaneous mitral balloon valvotomy in 1991 with return of normal speech after a few months. The recurrent laryngeal nerve paralysis is mainly due to the compression by an enlarged pulmonary artery as initially thought. This complication is rarely seen nowadays due to greater awareness of the disease and earlier intervention. With the advent of percutaneous transvenous mitral valvotomy in the nineties, effective non-surgical intervention is plausible. Key words : mitral stenosis, Ortner’s syndrome, percutaneous transvenous mitral valvotomy Introduction Mitral stenosis is a valvular lesion typically seen in adults as a result of childhood rheumatic carditis. If the valve lesion is unrecognized and untreated, serious and potentially fatal complication can occur. Left vocal cord paralysis and dysphagia are uncommon complications. These complications are hardly seen nowadays as intervention is taken early in its course. Mitral valve disease leading to production of hoarseness of voice due to left recurrent laryngeal nerve paralysis was first described by Ortner in 1897(1). Ortner was a Viennese physician who in 1897 described two patients with mitral stenosis and left recurrent laryngeal nerve paralysis. Occurrence of this syndrome is a rare phenomenon. Ortner reported the incidence of this syndrome in 0.5 per cent in their cases of mitral valve disease. Analysing all cases of recurrent laryngeal nerve paralysis, various authors have found mitral valve disease to be responsible in 0.25 per cent to 0.5 per cent of total cases(2-4). Case report A 29-year-old lady presented to an ENT surgeon with a two-year history of hoarseness of voice. She was subsequently referred to the cardiology unit for an incidental finding of a heart murmur. On direct questioning, she had a history of exertional dyspnea for the past two years. She could manage to climb three flights of stairs and 200 meters of brisk walk. There was no history of palpitation, orthopnoea or paroxysmal nocturnal dyspnoea. She gave no history of recurrent fever with sore throat during childhood. She had four uneventful spontaneous vaginal deliveries without any cardiac symptoms. Her last childbirth was 3 years prior to presentation. On examination, the patient appeared well with no dysmorphic facies. There was no peripheral oedema, cyanosis or clubbing. Her blood pressure was 120/80 mm Hg and her pulse was regular with a rate of 84/min. The head and neck examination was normal. Cardiovascular examination revealed an apex beat which was tapping in nature although not displaced. Left parasternal heave and a palpable second heart sound was present. On auscultation, the first heart sound was loud and the pulmonary component of the second heart sound was prominent at the apex and pulmonary area respectively. A grade 3/6 long rumbling diastolic murmur with opening snap was heard at the mitral area. The lungs were clear. Direct laryngoscopy performed by the ENT surgeon revealed a left vocal cord paralysis. Electrocardiogram showed sinus rhythm at a rate of 75/min. Tall p waves with bifid morphology (P mitrale) was evident with right axis deviation. Chest radiograph demonstrated normal cardiothoracic ratio with left atrial enlargement and mildly enlarged pulmonary arterial trunk. Transesophageal echocardiography (fig. 1) showed that the mitral valve was thickened and pliable. The mitral valve area was 0.95 cm2 using calculation from pressure half-time and no mitral regurgitation was seen. The left atrium and left atrial appendage were enlarged (left atrial diameter = 5.2 cm). There was no left atrial thrombus or spontaneous echo contrast seen. The right atrium and ventricle were both enlarged. Other valves were normal and no tricuspid regurgitation was noted. Her hemoglobin was 13.0 g/l, total white cell count was 4.9 x 109/(l and platelet count was 231 x 109/(l. ESR was 10 mm in the first hour. Blood urea was 3.6 mmol/l, sodium was 140 mmol/l, potassium was 3.8 mmol/l and serum creatinine was 98 mol/l. Total protein was 78 g/dl, albumin was 40 g/l, bilirubin was 8 mol/l, alanine transaminase was 12 U/l, alkaline phosphatase was 100 U/l and lactate dehydrogenase was 320 U/l She underwent a percutaneous transvenous mitral valvotomy using an Inoue balloon. Post procedure, the mid-diastolic murmur was no longer audible but there was a late 2/6 systolic murmur at the apex. Echocardiography one week later revealed thickened mitral valve with mild mitral regurgitation (secondary to posterior medial cusp being affected during the commisurotomy). No atrial septal defect demonstrated and the mitral valve area measured was about 3 cm2. Her hoarseness of voice recovered after a few months. She remained asymptomatic on follow-up. DiscussionMitral valve disease leading to production of hoarseness of voice due to left recurrent laryngeal nerve paralysis was first described by Ortner in 1897(1). Ortner was a Viennese physician who in 1897 described two patients with mitral stenosis and left recurrent laryngeal nerve paralysis. Occurrence of this syndrome is a rare phenomenon. Ortner reported the incidence of this syndrome in 0.5 per cent in their cases of mitral valve disease. Analysing all cases of recurrent laryngeal nerve paralysis, various authors have found mitral valve disease to be responsible in 0.25 per cent to 0.5 per cent of total cases(2-4). Vocal cord paralysis apppears to be caused by compression of the left recurrent laryngeal nerve between the enlarged hypertensive pulmonary artery, the aorta, and the ligamentum arteriosum and not by dilatation of the left atrium, as some observers have thought. Enlarged tracheobronchial lymph nodes may be an additional contributory factor(5). The onset of hoarseness is usually insidious and in the beginning it may be intermittent. But in due course of time it progresses to complete aphonia. Very few patients recover from hoarseness of voice after medical therapy but most of the patients treated surgically improves(6). The time of recovery may vary from a few days to a few years. Most of the patients with mitral stenosis have gradual development of left atrial hypertension, a large, compliant left atrium, and only a passive rise in pulmonary-artery-pressure, a rise commensurate with the increase in left atrial pressure. As the disease progresses their cardiac output may become fixed and eventually fall. The large, compliant left atrium and the low cardiac output may serve to prevent a sudden rise in the pulmonary venous pressure and protect them from paroxysmal dyspnoea and pulmonary oedema. Such patients may remain asymptomatic for many years and even after the appearance of symptoms, generally shortness of breath and fatigue, may lead comfortable lives. Their degree of disability may be slight. This could explain why patients with Ortner’s syndrome do not develop symptoms of heart failure despite significant enlargement of the left atrium or pulmonary artery. In addition to this paralysis of left recurrent laryngeal nerve has been reported with raised pulmonary pressure in essential hypertension (7,8), Eisenmenger’s syndrome(9), patent ductus arteriosus(10), atrial septal defect(11), left ventricular failure(12) and congenital heart disease(13). It seems that pulmonary hypertension is an important factor in production of hoarseness of voice in these patients. Other complications of left atrial enlargement includes dysphagia, thromboembolism and atrial fibrillation. Several studies before the days of cardiac surgery indicate that about 40 percent of the patients were dead within 10 years after the diagnosis of the mitral stenosis and close to 80 percent of the patients were dead at 20 years(16,17). The onset of atrial fibrillation which usually denotes underlying pulmonary hypertension often heralds a progressive decline in the patient’s condition and is a poor prognostic sign. References
© Copyright 2004 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj04022f1.jpg] |
| |||||||||

{kind=link}