 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
ORIGINAL ARTICLE INCENTIVE SPIROMETRY AS A MEANS TO SCOREBREATHLESSNESS Li-Cher Loh, Pek-Ngor Teh, Sree Raman*, Pillai Vijayasingham*, Tarmizi Thayaparan* IMU Lung Research, International Medical University Clinical School, Seremban; *Department ofMedicine, Seremban Hospital, Negeri Sembilan, Malaysia Code Number: mj05008 Perceived breathlessness played an important role in guiding treatment in asthma. We developed a simple, user-friendly method of scoring perception of dyspnoea (POD) using an incentive spirometer, Triflo II (Tyco Healthcare, Mansfield, USA) by means of repetitive inspiratory efforts achieved within three minutes in 175 normal healthy subjects and 158 asthmatic patients of mild (n=26), moderate (n=78) and severe (n=54). Severity was stratified according to GINA guideline. The mean POD index in normal subjects, and asthmatic patients of mild, moderate and severe severity were: 6 (4-7) 16 (9-23), 25 (14-37), and 57 (14-100) respectively (p<0.001 One-Way ANOVA). Based on 17 asthmatic and 20 normal healthy subjects, intraclass correlation coefficients for POD index within subjects were high. In 14 asthmatic patients randomized to receiving nebulised b2-agonist or saline in a crossover, double-blind study, % FEV1 change correlated with % changes in POD index [rs –0.46, p=0.012]. Finally, when compared with 6-minutes walking test (6MWT) in an open label study, respiratory POD index correlated with walking POD index in 21 asthmatic patients [rs= 0.58 (0.17 to 0.81) (p=0.007] and 26 normal subjects [0.50 (0.13 to 0.75) (p=0.008)]. We concluded that this test is discriminative between asthmatic patients of varying severity and from normal subjects, is reproducible, responsive to bronchodilator effect, and comparable with 6MWT. Taken together, it has the potential to score disability and POD in asthma effectively and simply. Key words : Perception of dyspnoea, asthma, normal subject, incentive spirometer, six-minute walking test Introduction
Dyspnoea can be defined as an appreciation of increased effort and discomfort associated with the act of breathing (1). These symptoms are best appreciated during exercise by placing the cardiorespiratory system under the stress of increased oxygen requirement and carbon dioxide output. Thus, quantification of exercise capacity provides an objective evidence of the degree of dyspnoea, especially when resting cardiopulmonary test results are disproportionately ‘normal’ for the level of complaint reported (2). The global increase in asthma morbidity and mortality is worrying (3). One important factor that contributes to this increase is the lack of appreciation of the disease severity by both the patients and healthcare professionals (4, 5, 6). Furthermore, there is evidence that perception of dyspnoea in some asthmatic patients may be impaired resulting in fatal and near-fatal asthma attacks, and increased hospitalization (7, 8, 9). The most widely used exercise testing employ workloads that are progressively increased by a standardized amount at intervals of time, until the subject is unable to continue or reaches a predetermined end-point. The treadmill and cycle ergometer are commonly used for this purpose and a variety of non-invasive (e.g. ventilation and heart rate) or invasive (e.g. arterial and central venous catherterization) measurements can be carried out during this time to enable documentation of cardiorespiratory adaptation from rest to capacity (2). However, these tests are cumbersome to perform, time-consuming and not readily accessible in the majority of places. As a result, simpler tests such as the six-minute walking test that measure disability and dyspnoea provide a useful alternative. They have the attractiveness of ease, better tolerability, and ‘low technical requirement’ to perform in large-sample population studies, disabled individuals and elderly subjects (10, 11, 12). In keeping with the concept that exercise test is preferable to measurements done at rest in assessing disability and perception of dyspnoea, and that a test that is cheap and easy to perform has many advantages, we developed the idea of using an incentive spirometry in asthmatic patients to score the maximal breathing capacity (MBC) by repetitive inspiratory efforts within a set time (3 minutes), and breathlessness perceived at the end of the inspiratory exercise- converted into a score dependent on MBCas an index of perception of dyspnoea (POD). The objective of this present study was to provide preliminary validation of this tool (Three-Minute Respiratory Exerciser Test, 3MRET) for use in asthmatic patients with regards to its reliability to differentiate between disease severities, its correlation with Forced Expiratory Volume in One Second (FEV 1), its reproducibility, and its responsiveness to the effect of bronchodilation, and finally, in how well it compared with the Six-Minute Walking Test (6MWT). Normal healthy subjects were added for comparison. Subject and Methods
Subjects
Between January and July 2003, a convenient sample of 158 asthmatic patients followed up in chest clinic of an 800-bed urban-based teaching hospital was recruited for the study. Asthma diagnosis was made according to international guidelines (3) and all severity of asthma was accepted. Over the same period of time, 175 normal healthy subjects, defined as having no chronic respiratory symptoms or any other known medical conditions, were recruited from the public and hospital staff. Normal healthy subjects were not current cigarette smoker and if previously had do so, smoked < 10 pack years. Socio-demographic and asthma-related variables were recorded using a standard questionnaire. All patients completed a selfanswered, health-related quality of life questionnaire, St Georges’ Respiratory Questionnaire (SGRQ) and underwent a threeminute respiratory exerciser test. Patients who had respiratory tract infections or asthma exacerbations postponed their study until at least 6 weeks after the complete resolution of symptoms. The study was approved by the local university research and ethics committee. Written informed consent was obtained from all patients. Three-minute respiratory exerciser test (3MRET)
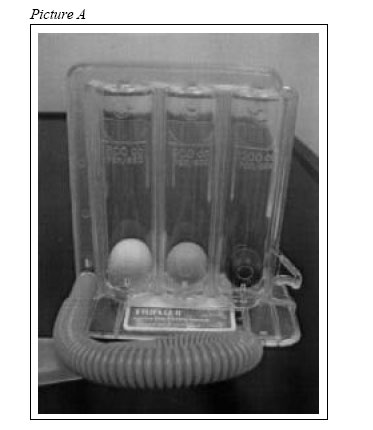
This test scored the maximal breathing capacity (MBC) by repetitive inspiratory efforts within three minutes, based on an incentive spirometry, Triflo II (Tyco Healthcare, Mansfield, USA) [Picture A] that was routinely used in our hospital for the purpose of chest physiotherapy, and scored the perception of dyspnoea (POD) at the end of this three-minute period. By repeated inspiratory effort, patients were asked to get as many balls as possible to reach the top of each of the three columns (A, B and C) within three minutes. Columns A, B and C required flow rates of 600 ml/min, 900 ml/ min and 1200 ml/min respectively to bring the balls to reach the top, and as such, required the generation of sufficient inspiratory effort on the part of the subject to achieve this. When all three balls reached their column tops, it indicated that the subject was able to generate inspiratory airflow of 1200 ml/ml. When only two balls reached their column tops, it indicated that the subject generated 900 ml/min. When only one ball reached their column tops, it indicated that the subject could only generate 600 ml/min. The cumulative times of three balls, two balls or one ball reaching the column top became an index of maximal breathing capacity (MBC score), and the formula used was as follows: MBC score= (number of times that all three balls reached the top of columns) x 2 + (number of times that two balls reached the column top) x 1.5 + (number of times that only one ball reached the column top) x 1. Immediately after the test, the patient placed a score on a visual analogue scale (VAS) between zero (not breathless at all) and ten (worst imaginable breathlessness) with regards to his POD. The POD index was calculated by dividing the POD VAS score with the MBC score, and then multiplying it by 1000. To standardize, POD VAS score of zero was replaced by a standard value of 0.125, to enable the calculation of the POD index using the equation described. Higher POD index indicated greater perception of breathlessness. Reproducibility study
From the original cohort of recruited subjects, 17 asthmatic and 20 normal subjects, matched for sex and age, were randomly recruited to undergo a study of the repeatability of MBC and POD measurements, where they underwent another 3MRET on a separate occasion at least one week after. Study on the bronchodilator effects on 3MRET
From the original cohort of asthmatic patients, 14 were randomly invited to undergo a randomized, placebo-controlled, double-blind, crossover study. In two visits separated by at least one week, each patient was nebulised with either 10mg bricanyl (active) or normal saline (placebo), and 3MRET preceded by measurement of FEV1 was performed before and after each nebulisation. Study comparing 3MRET and 6MWT
23 asthmatic and 26 normal subjects, matched for age and sex, randomly chosen from the original cohort of recruits were invited to participate in this open-label study whereby the subjects attended a separate visit at least one week after for a 6MWT. During this visit, the subjects were required to walk to and fro along a flat corridor as fast as they could within 6 minutes. The distance walked within this time was recorded as ‘walking distance’, considered equivalent to MBC by 3MRET. Immediately after the completion of 6MWT, the subjects were asked to place a score on a visual analogue scale (VAS) between zero (not breathless at all) and ten (worst imaginable breathlessness) with regards to their POD. Similar to the way POD index was calculated in 3MRET, walking POD index was produced by dividing POD VAS score by walking distance, and then multiplying it by 1000. Like before, to standardize, POD VAS score of zero was replaced by a standard value of 0.125, to enable the calculation of the POD index using the equation described.
Statistical analysis
Descriptive statistics were used to study the clinical variables of asthmatic and normal subjects. The values were expressed in mean and 95% confidence interval, or percentage. Differences in means or percentages of variables between groups were assessed using One-Way ANOVA for continuous data and Chi-Square test for categorical data. MBC score and POD index were expressed as means and 95% confidence interval, and their differences between groups were first assessed by One-Way ANOVA followed by post-hoc analysis with unpaired t tests if significant difference was found. Correlations between FEV1 % predicted normal with MBC score and POD index in asthmatic and normal subjects were assessed by Spearman rank tests. Intra-subject reproducibility of MBC score and POD index was assessed by intraclass correlation coefficients (13). Responsiveness of the 3MRET to bronchodilator effects on asthmatic patients was studied by assessment of correlations (by Spearman rank tests) between percentage FEV1 change and percentage change in MBC score and POD index before and after bronchodilation. Finally, correlations between measurements on disability (MBC for 3MRET and walking distance for 6MWT) and POD (POD index by 3MRET and 6MWT) were compared by Spearman rank tests for strength of associations and significance. Results
Subjects
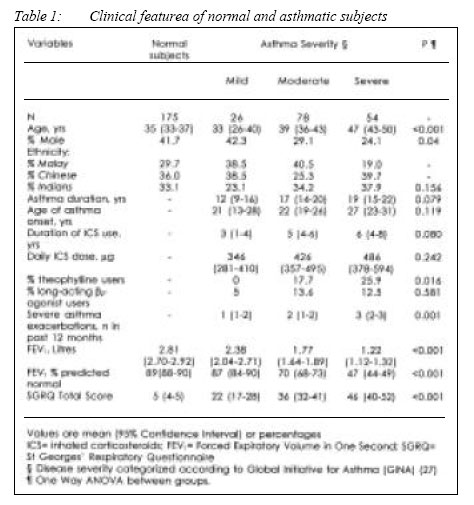
The clinical features of recruited subjects are listed in Table 1. Except for gender, the clinical variables that were statistically different between the groups were consistent with the severity of asthma in that patients with more severe disease were older, required more controller medication such as theophylline, had more severe exacerbations, exhibited greater airflow limitation, and reported poorer quality of life. MBC and POD score in asthmatic and normal subjects
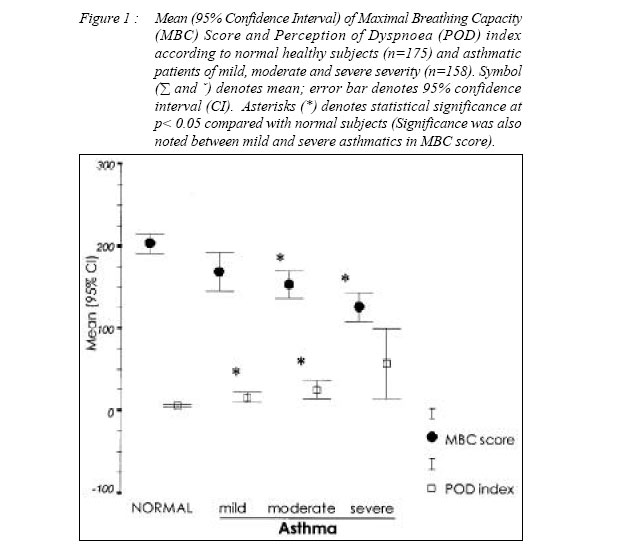
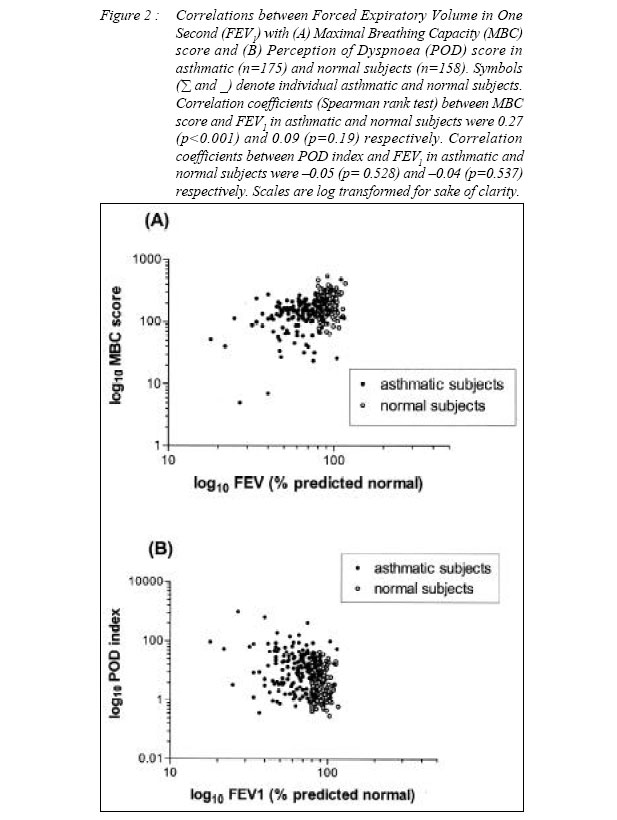
The mean MBC score in normal healthy subjects was the highest [mean (95% CI): 202 (191214)] across all groups. The mean scores were progressively lower with increasing disease severity [mild: 168 (145-192); moderate: 153 (136-169); severe: 125 (109-142)]. Statistically significant differences were observed between normal subjects and moderate asthma patients [mean difference (95% CI): 49 (23-76), p<0.001] and between normal subjects and severe asthma patients [77 (49-104), p<0.001], and between mild and severe asthma patients [42 (4-81), p=0.004] [Figure 1]. Mean POD index was lowest in normal subjects across all groups [mean (95% CI): 6 (47)]. The mean scores were progressively higher with increasing disease severity [mild: 16 (9-23); moderate: 25 (14-37); severe: 57 (14-100)]. Statistically significant differences were observed between normal subjects and mild asthma patients [mean difference (95% CI): 10 (1-19), p=0.004] and between normal subjects and moderate asthma patients [19 (4-34), p=0.001] [Figure 1]. It is noteworthy that unlike MBC, the spread around mean POD index increased dramatically with the increase of asthma severity. In severe asthmatic patients, the 95% confidence interval of mean POD index was between 14 and 100. The only correlation of FEV1 (% predicted normal) with MBC score in asthmatic patients was significant [rs (95% CI)= 0.27 (0.118- 0.416); p<0.001]. There was no correlation between POD score and FEV1 in asthmatic and normal subjects, or between MBC score and FEV1 in normal subjects [Figure 2]. Reproducibility of MBC score and POD index
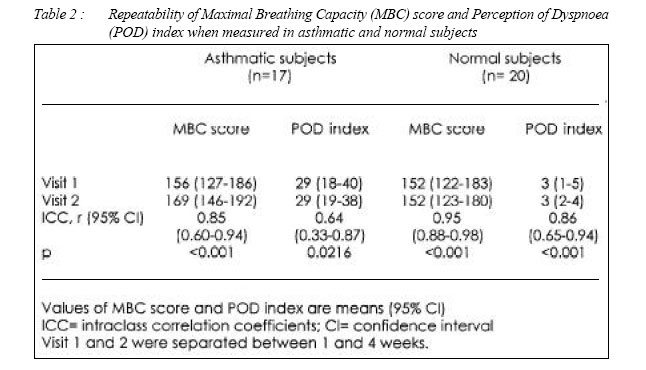
17 asthmatic patients [mean (95% CI): age, 44 (35-52) yrs, FEV1 % predicted normal, 64 (5671); 41% male] and 20 normal healthy subjects [age, 46 (42- 49) yrs; FEV1 % predicted normal, 89 (8593); 30% male] successfully completed this study. Intraclass correlation coefficients of measurements within subjects for both MBC score and POD index performed on two separate occasions were generally high and all were statistically significant [Table 2]. Normal subjects had overall higher intra-subject consistency in both measurements, compared with asthmatic subjects. The lowest consistency (r= 0,64) and widest 95% confidence interval (between 0.33 and 0.87) is found in the measurement of POD index in asthmatic subjects. Responsiveness of MBC score and POD index to bronchodilatation
14 asthmatic patients [mean (95%): age, 39 (27-50) yrs, FEV1, 63 (57- 68)% predicted normal; male, 42%] successfully completed the randomized, double-blind, placebo-controlled, crossover study. The mean percentage (95% CI) FEV1 change after nebulised short acting b2-agonist and normal saline were +23 (+8 to +38) and 0 (-6 to +5) respectively. Correlations, rs (95% CI) between changes in % FEV and those in MBC score and POD index were 0.49 (0.14 to 0.74) (p<0.01) and –0.46 (-0.72 to – 0.10), (p=0.012) respectively. Correlations between three-minute respiratory exercise test and six-minute walking test
Apart for 2 asthmatic patients who were withdrawn following development of clinically important wheezing during the 6MWT, 21 asthmatic patients [mean (95% CI): age, 42 (32-51) yrs, FEV% predicted normal, 69 (60-77); male, 19%] and 26 normal healthy subjects [age, 40 (32- 49) yrs; FEV% predicted normal, 89 (86- 93); male, 26%] successfully completed the study. Correlation coefficients, rs (95% CI) between MBC score and walking distance in asthmatic and normal subjects were 0.47 (0.02 to 0.76) [p=0.03) and 0.53 (0.16 to 0.76) [p=0.005] respectively. Correlation coefficients, rs (95% CI) between respiratory and walking POD index in asthmatic and normal subjects were 0.58 (0.17 to 0.81) [p=0.007] and 0.50 (0.13 to 0.75) [p=0.008] respectively. Discussion
We have shown that 3MRET can differentiate between asthma severities, and MBC score in asthma patients correlated with FEV1. Furthermore, we showed that the scores by 3MRET are reproducible, responsive to the effect of bronchodilation, and comparable to that of 6MWT. This exercise test requires repetitive inspiratory effort by the subject to achieve as high score as possible from the number of balls reaching the column tops of an incentive spirometry (Triflo II by Tyco Healthcare). It is simple for the subject to perform and easy for the assessor to score. The apparatus is cheap (about US$ 4.00 each), washable and reusable up to at least 50 times. The time limit of three minutes was arbitrarily chosen based on the preliminary observation that most normal healthy subjects experience some degree of breathlessness after this time (data not shown). Also in this study, subjects were also routinely asked whether they could differentiate between ‘breathlessness’ and ‘tiredness’ for the purpose of scoring POD on the VAS. All except one normal healthy subject responded in affirmation, suggesting that differentiation between dyspnoea and fatigue is unlikely to be a major problem for most subjects. This can be important as dyspnoea and fatigue may be considered as separate variables of outcome measures in exercise test including the 6MWT 10. It is safe in that no subjects, normal or asthmatic, reported any adverse events, for example, severe wheezing or fainting, from the 3MRET test. However, two asthmatic patients were not able to complete the 6MWT due to development of clinically significant wheezing during walking. Like other dynamic lung function test like spirometry, the 3MRET is a volitional test in that it is dependent very much on the effort put in by the subject. Thus, it requires proper supervision and adequate motivation. Low effort by the subject will result in low MBC score that may not cause much sense of breathlessness. For this reason, POD was scored by dividing MBC score over VAS on POD, naming it as POD index. As a result, a subject who has a low MBC score resulting in a low VAS on POD, would produce a similar POD index to another subject who has a high MBC score resulting in a high VAS on POD. However, a subject who truly has breathlessness beyond that which is normally experienced, would have a low MBC score but high VAS on POD, leading to a high POD index. Conversely, a subject who is capable of a high MBC score but has little breathlessness, would have a very low POD index. Therefore, POD index makes correction for the breathing workload capable of an individual. Our findings of relatively narrow 95% confidence intervals (CI) in POD index of normal and asthmatic subjects of mild and moderate severity, but relatively wide 95% CI in severe asthma patients, provided some validity that such index is meaningful, since if this approach is inappropriate, 95% CI would be large and similarly so in all groups of asthma severity and in normal subjects. Another important consideration is whether our test results are subjected to bias by intra- and inter-observer error. The assessor, due to the speed by which balls hit the top, may misjudge the number and frequency of balls reaching their column tops. This had not been formally investigated in our study and should be further explored. Importantly, we showed that while the 95% confidence intervals in MBC scores in normal and asthmatic of different severity were relatively similar, the intervals in POD index were progressively widened with increasing asthma severity. This indicates that in patients with more severe asthma, the POD can vary considerably for the same degree of MBC. In general, it has been shown that diminution or impairment of POD can occur in asthmatic patients with more severe disease in terms of lower baseline FEV1 (19, 20, 21), greater airway hyperresponsiveness (19, 20, 21), persistence of airway inflammation (23). In ‘exercise’, as in our test, we showed that the variation of POD also increased, most prominently in severe disease, providing support for the notion that in severe disease, there are over- and under-perceiver of dyspnoea. Our observation that POD index correlated poorly with FEV1 in asthmatic patients provides further support that change in FEV1 alone in asthmatic patients does not explain their perceived breathlessness (2), and therefore, other factors such as age (24), hyperinflation (25), and treatment with inhaled corticosteroids (26), may also have an influence on POD. The reproducibility of these measurements by 3MRET is important as it supports the validity of the results of a crossover study. While statistical significance was observed in all outcome measures for both the reproducibility and randomized controlled study, it is worth noting that POD score generally fared poorer than MBC score, reflecting the wider variability in POD between and within subjects when compared with MBC. The converse however is true when compared with 6MWT where POD score calculated at the end of maximal exercise, whether by repetitive inspiratory effort or walking, correlated at a greater significance level than the degree of maximal exercise capable of the individual. This seems to suggest that regardless of the forms of symptoms limiting exercise, scoring of POD can be reliably carried out using our simple ratio of perceived breathlessness over maximal workload capable of the individual. It may be that the 3MRET is superior in that the exercise is confined to respiratory effort, and not complicated by other physiological constraints such as leg muscle fatigue when walking or cycling is involved. Our preliminary study suggests that the 3MRET has discriminative value between normal healthy subjects and asthmatic patients of varying severity. Its reproducibility and responsiveness to bronchodilator effect, and correlation with 6MWT suggest that it has evaluative value for assessing disease progression and therapeutic interventions. The full potential for this test requires testing in larger sample of subjects and patients with other chronic respiratory diseases such as COPD and pulmonary fibrosis. The possibility of a tool like 3MRET that reliably scores POD in such convenient and user-friendly manner may provide insight into the research on nature of POD in various disease states, and the study of asthmatic patients who underor over-perceive breathlessness. Acknowledgements
References
This study was supported by an internal research fund provided by International Medical University, Malaysia.
© Copyright 2005 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj05008t1.jpg] [mj05008f3.jpg] [mj05008f1a.jpg] [mj05008f2.jpg] [mj05008t2.jpg] [mj05008f4.jpg] [mj05008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}