 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 12, No. 1, July 2005, pp.64-67 CASE REPORT GALLIUM SCAN IN DIAGNOSING OCULAR SARCOIDOSIS
Shatriah Ismail, Zunaina Embong, Wan Hazabbah Wan Hitam Department of Ophthalmology,
School of Medical Sciences, Universiti Sains Malaysia, Health Campus
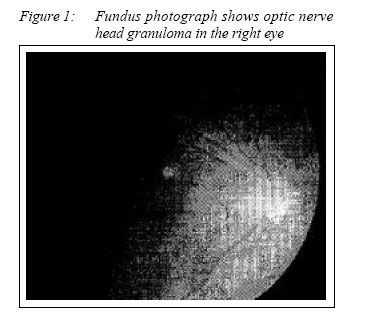
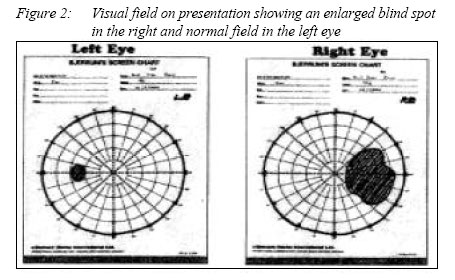
16150 Kubang Kerian, Kelantan, Malaysia Code Number: mj05011 A 40-year-old man presented with floaters and painless progressive blurring of vision in the right eye for one month duration. Visual acuity in the right eye was 6/24. There was mild anterior chamber reaction and vitritis. The optic disc was swollen and elevated with presence of granulomatous lesion in the optic disc head. Blood investigations were unremarkable. Serum angiotensin converting enzyme (ACE) was normal and conjunctival biopsy showed presence of inflammatory cells. B-Scan ultrasound revealed an echo-dense lesion in the optic nerve head. There was increased uptake of the right lacrimal gland and presence of ‘Panda sign’ with Gallium scan. A diagnosis of right ocular sarcoidosis was made base on the clinical features and Gallium scan. Key words : Ocular sarcoidosis, Gallium scan Introduction Ocular sarcoidosis may present with a wide variety of ocular symptoms in all parts of the eye. The diagnosis may be difficult owing to the absence of diagnostic criteria and the variety of presentations. The diagnosis usually is suggested by a combination of clinical, radiology and laboratory findings and supported by a tissue biopsy showing non-caseating granulomas (1). Gallium scan has been shown to be useful in aiding the clinical diagnosis of ocular sarcoidosis in patients with either normal or equivocal chest radiographs. Case report The patient is a 40-year-old Malay male who presented with a history of painless progressive reduced vision in the right eye for one month duration. The central vision was affected and decreased vision was associated with floaters. Vision in the left eye was good. There was no history of joint pain, backache, skin rash or nodule, mouth or genital ulcer, haemoptysis and loss of weight or appetite. He denied other medical illness before. The visual acuity in the right eye was 6/24 and not improved with pinhole. Vision in the left eye was 6/6. There was relative afferent pupillary defect in the right eye. The other optic nerve function tests such as colour vision and light brightness were also impaired. There was no enlargement of the lacrimal gland or eyelid nodule noted. Anterior segment examination of the right eye revealed a clear cornea and normal conjunctiva. There was mild anterior chamber reaction and normal iris texture. The intraocular pressure was normal. The anterior segment examination of the left eye was unremarkable. The right posterior segment revealed moderate vitritis with presence of few snowballs and vitreous strands inferiorly. The optic disc was swollen and elevated with presence of granuloma in the optic disc head (Figure 1). The vessels were dilated and tortuous with sheathing of superior branch of retinal vein. There were presence of multiple discrete yellow-white choroidal lesions at the superotemporal area of peripheral retina. The macula was normal. The fundus examination of the left eye was unremarkable. Visual field examination showed an enlarged blind spot with central scotoma in the right eye and normal field in the left eye (Figure 2). Systemic physical examination was unremarkable. There was no lymphadenopathy, organomegaly or neurological deficit noted. No sign of chronic inflammatory disease was elicited.
Investigation
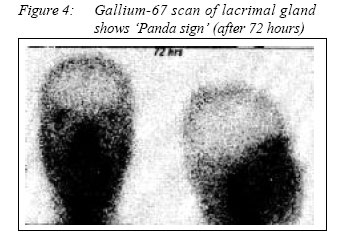
Blood investigations were unremarkable. The Mantoux test was normal (10mm). The Chest Xray finding was also normal without hilar opacity seen. Both serum and urine calcium levels were within normal range. The angiotensin converting enzyme level was 53 U/L (normal range: 40-140U/L). Conjunctival biopsy specimen from the right eye showed evidence of chronic inflammatory condition with no granuloma seen. Gallium-67 citrate showed increased uptake of the right lacrimal gland and presence of ‘Panda sign’ (Figure 3) Diagnosis and Treatment
Based on the clinical features and Gallium scan finding, the patient was diagnosed to have ocular sarcoidosis of the right eye. He was treated with oral prednisolone 1.5 mg/kg daily and topical dexamethasone every 2 hourly. The ocular features were monitored closely including visual acuity and visual field. His visual acuity gradually improved to 6/6 over 10 days of oral prednisolone. Review of the fundus showed improving vitritis with less vitreous strands. The optic disc was still elevated but with clearer margin. Sheathing of the superior branch of retinal vein had disappeared. The choroidal lesions became less prominent and there was no new lesion noted. The oral prednisolone was tapered down after two weeks and subsequently off after six weeks. The visual field gradually improved back to normal following the above treatment. The size of the granuloma of the optic nerve head became smaller and the vitreous became clear. There was presence of a chorioretinal scar inferiorly with no more vitreous strand seen. Discussion Gallium scanning has been used extensively for diagnosing sarcoidosis and other inflammatory process (2,3,4). The 67-gallium molecule probably blinds to the T lymphocyte and macrophages, representing a regional inflammatory response. Combined lacrimal, parotid, and submandibular gland uptake has been termed the ‘panda sign’, whereas the triad of right paratracheal and bilateral pulmonary and mediastinal uptake is the ‘lambda sign’, highly suggestive of sarcoidosis (5,6). In the above patient, gallium scanning of the orbit, head and neck demonstrated significantly increased 67-gallium uptake in the right lacrimal gland. There was also increased 67-gallium uptake in the left lacrimal gland and parotid glands that gave an appearance of ‘Panda sign’. Depression delayed-type hypersensitivity is one of the immunological changes in sarcoidosis. Increased proportion of circulating suppressor cells have been demonstrated in sarcoidosis (7). Positive tuberculin reactivity in sarcoid patient is suggestive of increased helper-cell activity (8). Serum ACE and serum lysozyme are found to be elevated in sarcoidosis. The source of the ACE is probably the giant cells. Baarsma et al (9) reported that in patients with uveitis who had serum ACE level above 50 u/L, the sensitivity of the test was 84% and the specificity was 95% in the diagnosis of ocular sarcoidosis. The combination of positive gallium uptake and an elevated serum ACE was a specific and sensitive tool for diagnosing patients suspected of having ocular sarcoidosis but had normal chest radiographs. Power et al (10) reported that the specificity for diagnosis was 100% and sensitivity 73% when there was a combination of elevated serum ACE level and a positive 67-Gallium scan present. Serum ACE activity reflects overall systemic inflammatory activity, whereas Gallium scanning assessing localized sites of inflammation (10). The most useful non-invasive test which should be performed in helping to confirm the diagnosis of sarcoidosis are serum ACE and Gallium scan of the lacrimal gland. Acknowledgement
I would like to convey many thanks to Dr Malik Mumtaz, Lecturer in Department of Nuclear Medicine, School of Medical Sciences, Universiti Sains Malaysia, Kelantan for his tremendous help and encouragement in writing this report. References
© Copyright 2005 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj05011f3.jpg] [mj05011f1.jpg] [mj05011f4.jpg] [mj05011f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}