 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
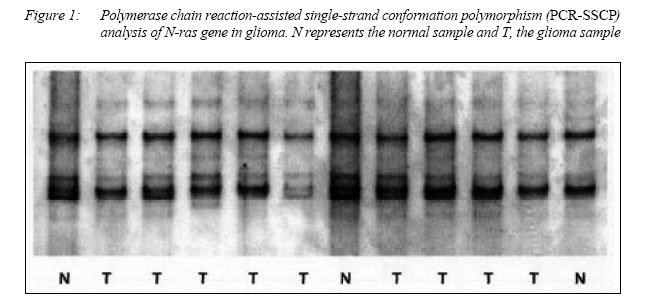
Malaysian Journal of Medical Sciences, Vol. 12, No. 2, July 2005, pp.27-33 ORIGINAL ARTICLE ABSENCE OF Ras, c-myc AND EPIDERMAL GROWTH FACTOR RECEPTOR (EGFR) MUTATIONS IN HUMAN GLIOMAS AND ITS CLINICAL FACTORS ASSOCIATED WITH PATHOLOGICAL GRADING AFTER SIX YEARS OF DIAGNOSIS IN NORTH EAST MALAYSIAN PATIENTS Mazira Mohammad Ghazali, Mohd Shahril Mohd Zan, Abdul Aziz Yusof, Jafri Malin Abdullah, Hasnan Jaffar*, Abdul Rahman Ariff**, Win Mar@Slamah**, Aini Ideris***, Abdul Manaf Ali***, Abdul Rahman Omar***,Khatijah Yuosff***, Mohd Azmi Mohd Lila***, Fauziah Othman***, Noordin Mohamed Mustapha***, Mohd Nizam Isa**** & Nyi Nyi Naing***** Department of Neurosciences, *Department of Pathology, **Department of Radiology, ****Human
Genome Center, *****Biostatistics and Research Methodology Unit, Universiti Sains Malaysia,
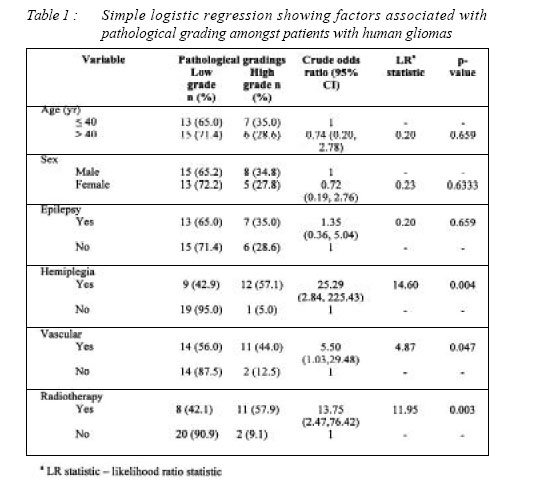
Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia, ***Universtiti Putra Malaysia, Serdang, Selangor Malaysia Code Number: mj05017 Neoplastic transformation appears to be a multi-step process in which the normal controls of cell proliferation and cell-cell interaction are lost, thus transforming normal cells into cancer. The tumorigenic process involves the interplay between oncogenes and tumour suppressor genes. In this study, we have selected the ras family, c-myc and epidermal growth factor receptor (EGFR) genes to detect whether their abnormalities are associated with the expression and progression of glioma cases in Malay patients. We have used the polymerase chain reaction-single stranded conformation polymorphism followed by direct sequencing for the study. For the ras gene family, we screened the point mutations in codons 12 and 61 of the H-, K-, and N- ras gene; for EGFR and c-myc, we analyzed only the exon 1 in glioma samples. In mutational screening analyses of the ras family, c-myc and EGFR gene, there was no mobility shift observed in any tumour analyzed. All patterns of single stranded conformation polymorphism (SSCP) band observed in tumour samples were normal compared to those in normal samples. The DNA sequencing results in all high-grade tumours showed that all base sequences were normal. All 48 patients survived after five years of treatment. In simple logistic regression analysis, variables which were found to be significant were hemiplegia (p=0.047) and response radiotherapy (p=0.003). Hemiplegics were 25 times more likely to have high pathological grade compared to those without. Patients with vascular involvement were 5.5 times more likely to have higher pathological grade. However, these findings were not significant in multivariate analysis. Patients who had radiotherapy were nearly 14 times more likely to have higher pathological grade. Multivariate analysis revealed that patients with hemiplegia were more likely to have higher pathological grade (p= 0.008). Those with higher pathological grading were 80 times more likely to have radiotherapy (p=0.004). Key words : Ras gene, c-myc, EGFR, Gliomas, Malaysia IntroductionNeurological tumours are common neoplasms of both adults and children. Recent studies have attempted to delineate the genetic abnormalities that underlie such tumours, and have implicated two classes of genes, oncogenes and tumour suppressor genes. Neoplastic transformation also appears to be a multi-step process in which the normal controls of cell proliferation and cell-cell interaction are lost, thus transforming a normal cell into a tumour cell. This tumorigenic process involves the interplay between at least two classes of genes: oncogenes and tumor suppressor genes. Oncogenes are abnormally activated versions of cellular genes that promote cell proliferation and growth. Therefore, activated oncogenes result in an exaggerated impulse for a cell to grow and divide. Gliomas mostly occur sporadically, and are known to be non-inherited tumours. The predisposition to develop gliomas is also associated with hereditary illness (including NF-1), tuberculosis complex, Gardner’s syndrome, Turcot’s syndrome, Li-fraumeni syndrome and other factors. Binger and colleagues have suggested that despite the heterogeneity observed among glioblastoma karyotypes, several distinct abnormalities are frequently detected as losses of chromosome 10 (60%) and 17, gains of chromosome 7 (18%), translocation and deletions of chromosome 9p at lower frequency (20%) and losses of chromosome 22 and sex chromosome (http:// www.thamburaj.com/neurogenetics.htm). Molecular abnormalities associated with primary brain tumours include a wide variety of changes in tumour suppressor genes, protooncogenes and growth factors. Ras gene families consist of 3 members: Nras, H-ras and K-ras, that encode for the highly homologous protein called p21 according to their molecular weights. The inactivation of ras genes by point mutation is the most frequent and well known genetic alteration associated with human cancer including brain tumours. Common mechanisms of inactivation of these genes include missense mutations at the well known hot spot of codon 12, 13 and 16 (1). The presence of ras mutation has also been shown to be significant for prognosis and considering the importance of the ras gene in tumorigenesis, this gene might be a good target for the development of anti-cancer therapy (2). The c-myc gene, mapped on human chromosome 8q24, encodes the transcription factor c-myc, that heterodimerizes with a partner protein, Max, to regulate gene expression. The amplification of the c-myc gene in neuroblastomas appears to correlate with the clinical stage of the tumour and poor prognosis. Therefore, it is tempting to speculate that the c-myc protein is one of the essential products necessary for the aberrant behaviour of neuroblastoma cells (3). Over-expression and amplification of c-myc may play an important role in metastatic progression, and there is evidence that it indicates poor prognosis in the largest clinical populations of breast, colon, lung and pancreatic cancers (3). c-myc’s status as an important target was reinforced by a recent widely-reported paper published in Science by Dean Felsher at Stanford, in which he demonstrated that a temporary reduction in c-myc expression followed by reactivation, in a genetically engineered mouse model, induced highly selective and complete apoptosis in cancer cells, while having no effect on normal cells (4). The EGFR gene is a multifocal allosteric transmembrane protein with an intra cellular binding site for EGF, and acts as a tyrosine kinase. The gene is localized on the short arm of chromosome 7, within 7p11 – 13, and is called erb – B1. This receptor has been found to be over-expressed in 50% to 70% of glioblastoma multiforme. Although the functions of the proteins encoded by most protooncogenes are not precisely known, biochemical activities of several proto-oncogene products have been identified. Some of the gene products are identical or related to proteins known to be important in growth regulation. We analysed ras family, c-myc and EGFR to determine whether they are involved in the tumourigenesis of gliomas in a group of patients in Hospital Universiti Sains Malaysia in North East Malaysia. The objective of this study was to relate the mutation analysis to the eventual response of these tumours to clinical outcomes. Materials and Methods Sample Collection and DNA ExtractionA series of 41 glioma specimens were obtained from the Brain Tumour Bank of the Department of Neurosciences, School of Medical Sciences, Universiti Sains Malaysia with ethical approval of the Research and Ethics Committee, Universiti Sains Malaysia. The tumours were classified according to the World Health Organizations (WHO) classification. DNA was extracted from the tumour tissue using commercial extraction kits (QIAGEN Inc. USA). PCR AmplificationPCR was performed to amplify DNA segments of H-ras, K-ras and N-ras. The nucleotide sequences of H-ras, K-ras and N-ras were shown in Table 1 (1). PCR reactions were performed in 100 µl volumes using 50 to 100 ng of genomic DNA templates, 1 X PCR buffer, 200 µM of dNTP, 2 mM MgCl2, 1.0 µM (50 pmol) of each primer and 2.5 unit of Taq DNA polymerase (Fermentas USA). Thirty-five cycles were performed as follows: denaturation at 94oC for 1 min, annealing at 58oC for 1 min and extension at 72oC for 1 min. after the last cycle of amplification, the extensions were continued for an additional 7 min at 72oC. Primers designed to amplify the c-myc exon I intron I regulatory region contained the sequence in Table 2. The PCR products were 589 bp in size and included 162 bp in exon I and 427 in intron 1. The PCR reaction mix consists of 1 µl of DNA extract, 10 mM Tris (pH 8.3), 50 mM KCl, 1.5 mM MgCl2, 200 µM of each dNTP (Promega, Southampton, U.K) in a total volume of 25 µl. Forty cycles of PCR were carried out on a thermal cycler (Perkin Elmer) consisting of denaturing at 94oC for 30 s, annealing at 65oC for 30s and extension at 72oC for 45oC. And initial denaturing step at 95oC for 5 min preceded the addition of enzyme and an extension step at 72oC for 5 min concluded the reaction. Three microlitres of PCR product was checked for yield size on a 1% agarose gel. A total of 5 µl of PCR products was digested by Taq I (Promega Inc. USA) to generate one 223 bp and two 183 bp fragments. The total volume of the PCR mixture of EGFR was 100 ml containing 1X PCR buffer, 200 mM of dNTP, 2 mM MgCl2, 1.0 mM (50 pmol) of each primer and 2.5 unit of Taq DNA polymerase (Fermentas USA). Amplification was carried out in MJ Research for 940C for 1 min, 580C for 1 min and 720C for 1 min, with an initial denaturation step at 940C for 10 min, and a final extension at 720C for 10 min, for 30 cycles. SSCP (Single-Strand Conformation Polymorphism)Each of 8 µl PCR product of ras, c-myc and EGFR were added to 4 µl of sequencing stop solution (Amresco Inc. USA). The mixture was heated at 90oC for 5 minutes, chilled on ice and applied to a 0.5X MDE gel (FMC Bioproduct USA) or 6% acrylamide gel containing 5%-10% glycerol. Electrophorisis was performed using the Dcode universal mutation Detection System (Bio-Rad Laboratories USA) at 10 watts constant and at room temperature. The running time was approximately 14 to 18 hours. The gels were stained using silverstaining (5). Direct Sequencing AnalysisThe samples that showed abnormal mobility in the SSCP analysis were isolated and run on 2% agarose gels and purified using a Geneclean II kit (Bio101 Corp, USA) in preparation for sequencing. Purified products were sequenced on an ABI 3100 automatic sequencer using the same primer as those used in the PCR-SSCP. Clinical, Radiological and Treatment ParametersThe patients were studied over a period of 60 months. Parameters like age, sex, socio- economic status, and presenting complaints such as headache, visual disturbances, hemiplegia, epilepsy as well as radiological images (site, size, consistency of tumour, oedema, calcification, haemorrhage, intensity on MRI, midline shift and vascularity) were compared to their management, ras family, c-myc and EGFR mutations, relapse rate and outcome. Socio-economic groups were divided into upper class (> 250 USD), middle class (100-250 USD) and lower class (<100 USD). All patients underwent a MRI GE 1 Tesla prior to surgery and received gadolinium following certain protocols. Location of tumours was recorded according to the respective lobes and sites. Size of tumours was measured using the standard software provided by the GE MRI machine. The consistency of tumours were reported by two blinded radiologists as defined by a Japanese study (2). Calcification was detected by CT Scan of the brain with a Hounsfied between 100-300 H.U. . Haemorrhage in the tumour is defined as any hyperdensity (Hounsfield between 75 to 80 H.U.) measured using the classical protocol. Midline shift was defined as any deviation of the midline, taking the pineal gland as the centre. Vascularity was defined as any tumour blush seen on MRI done on the 1 Tesla machine as seen by two blinded neuroradiologists. All patients underwent total removal of tumours confirmed by repeat CT scans with contrast within 24 hours of operation. If the tumour was still present a reoperation was done to remove all tumour tissues and reconfirmed by CT scan of the brain with contrast. Treatment modalities were chemotherapy, radiotherapy and immunotherapy as requested and agreed by both radiation therapist/oncologist and patient. Recurrence on CT/MRI was defined as any disease or lesion returning or showing a tendency to return from time to time within the study period. Relapse of signs and symptoms were defined as the reoccurrences of symptoms similar to the previous complaints or signs seen again on physical examination without the knowledge of the radiological results. Ras family, c-myc and EGFR mutations were examined using various methods mentioned above. Outcome was defined as alive in good condition with a score of > 70, alive in poor condition, being unable to fend for oneself completely with a Karnofsky score of < 70 and dead. All patients were operated on and had a Karnofsky score of more than 70 before being included in the study. All histopathological examinations were reported according to the WHO classification and seen by at least three histopathologists and discussed in our neuropathology conferences and all the specimens were analysed twice to rule out false or negative results. Statistical Analysis on Factors Associated with Pathological GradingsSimple logistic regression analysis was applied to determine potential factors associated with the pathological grading. Pathological grading was treated as a binary outcome variable. Crude odds ratios with 95% confidence intervals likelihood ratio statistics and corresponding p-value were presented. Variables that were significant in simple logistic regression and variables that were considered to be clinically important were included in multivariate analysis. Multiple logistic regression analysis was applied to determine factors associated with the pathological grading. Stepwise backward logistic regression was used with the probability of entry at 0.05 and removal at 0.3. Likelihood ratio test was applied in the modeling procedure. Adjusted odds ratios with 95% confidence interval, Wald statistic and corresponding p-values were presented. Fit of the model was determined by using the Hosmer and Lemeshow test and overall classification percentages. Results Identification of Mutation of Ras Family, c-myc and EGFR GeneForty one glioma samples underwent PCR amplification by using H-ras, K-ras N-ras, c-myc and EGFR gene primers and were subjected to PCR-SSCP analyses and DNA sequencing. In mutational screening analyses of the ras family, c-myc and EGFR genes, there was no mobility shift observed in any tumour analyzed. All patterns of SSCP band observed in tumour samples were normal compared to those in normal samples. The DNA sequencing results in all high-grade tumours showed that all base sequences were normal. Clinical Factors Associated with Pathological FindingsAll 41 patients survived after six years of treatment. In simple logistic regression analysis, variables which were found to be significant were hemiplegia (crude OR 23.29, 95% CI 2.84- 225.45, p=0.004), vascularity (crude OR = 5.5, 95% CI 1.03 – 29.48, p=0.047) and response radiotherapy (crude OR=13.75, 95% CI 2.47-76.42, p=0.003). Hemiplegics were 25 times more likely to have high pathological grades compared to those without. Patients with vascular involvement were 5.5 times more likely to have higher pathological grades. However, this finding was not significant in multivariate analysis. Patients who had radiotherapy were nearly 14 times more likely to have higher pathological grades. Multivariate analysis revealed that patients with hemiplegia were more likely to have higher pathological grades (adjusted OR =171.36, 95% CI 3.88 – 7566.01, p= 0.008). Those with higher pathological gradings were 80 times more likely to have radiotherapy (adjusted OR 80.92, 95% CI 3.941662.91, p=0.004). DiscussionThere were no mutations of 3 types of genes (ras family, c-myc and EGFR) in our study. We identified no abnormal SSCP band shift in these samples and reconfirmed by performing direct DNA sequencing analysis. The ras family, c-myc and EGFR genes were not involved in the tumourigenesis in our patients and may not be the common inactivation mechanism in the pathogenesis of gliomas in North East Malaysian patients. The authors of previous studies have also shown that EGFR gene was often mutated in highgrade gliomas in adult, but the frequency of EGFR mutations was still low (6, 7). Feng et al (8) reported that 90% of human pancreatic cancers, 50% of colon cancers, and morethan 30% of smoking-related lung cancers have a mutation at codon 12 of the K-ras gene. Interestingly,only 5% of lung cancers that are not smoking-related containa mutation at codon 12 of the K-ras gene. The presence of ras mutation has also been shown to be significant for prognosis and considering the importance of the ras genes in tumorigenesis, the ras gene might be a good target for the development of anti-cancer therapy (8). However, our results revealed that no mutations were present in the ras gene family in gliomas using the Polymerase Chain Reaction-Single Strand Confirmation Polymorphism (PCR-SSCP) analyses in the DNA extracted from glioma tissues. According to Yusoff et al, Zan et al and Ghazali et al, there were no ras mutation detected in all tumours analyzed from Malaysian patients (9 11). They concluded that this gene does not play a major role in the tumourigenesis of malignant gliomas (6). Direct sequencing analysis in oral tumours also reported that no mutation has been found in N-ras, K-ras and H-ras genes. Activating ras mutations can be found in human malignancies with an overall frequency of 15-20%. A high incidence of ras gene mutations has been reported in malignant tumours of the pancreas (80-90%, Kras), colorectal carcinomas (30-60%), nonmelanoma skin cancer (30-50%, H-ras), hematopoietic neoplasia of myeloid origin (18-30%, K-and N-ras) and seminoma (25-40%, K-ras). In other tumours, a mutant ras gene is found at a lower frequency: breast carcinoma (0-12%, K-ras), glioblastoma and neuroblastoma (0-10%, K-and Nras) (8). Trent et al described the amplification and expression of the cellular oncogene c-myc in doubleminute-containing cells from one patient with glioblastoma multiforme, and they have shown that the amplification is associated with the rearrangement of the c-myc gene (12). This finding further supports the uncommon association of the myc gene family in neurogenic tumours and provides rare evidence of myc gene amplification in high grade gliomas. In another study, c-myc gene was involved in leukemia, breast, stomach and lung cancer. The c-myc gene was discovered as the cellular homolog of the retroviral V-myc oncogene 20 years ago. The c-myc proto-oncogene was subsequently found to be activated in various animal and human tumours . It belongs to the family of myc gene that includes B-myc, L-myc, N-myc and s-myc; however only c-myc, L-myc and N-myc have neoplastic potentials. It is possible that other mechanisms exist where ras family, c-myc and EGFR inactivation are involved in the development of brain tumours in our Malay patients. It is interesting to note that these patients are still alive 6 years after treatment despite some having high grade gliomas. AcknowledgementsThis work has been supported in part by Majlis Kanser National (MAKNA), Malaysia grant with collaboration between USM, UPM and MAKNA References
© Copyright 2005 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj05017t2.jpg] [mj05017f1.jpg] [mj05017t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}