 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
ORIGINAL ARTICLE AMBULANCE SERVICES AT HOSPITAL UNIVERSITI SAINS MALAYSIA AND HOSPITAL KOTA BHARU: A RETROSPECTIVE STUDY OF CALLS Mohd Shaharudin Shah Che Hamzah, Rashidi Ahmad, Nik Hisamuddin Nik Abdul Rahman, *Kasmah Wati Pardi, **Naimah Jaafar, Wan Aasim Wan Adnan, Kamaruddin Jaalam, *Syed Mohsin Sahil Jamalullail Department of Emergency Medicine, School of Medical Sciences,
*School of Health Sciences, Universiti Sains Malaysia, Health Campus
16150 Kubang Kerian, Kelantan, Malaysia, **Emergency Department, Hospital Kota Baharu,
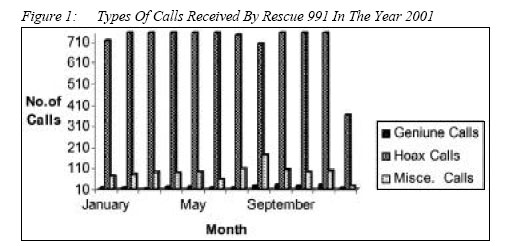
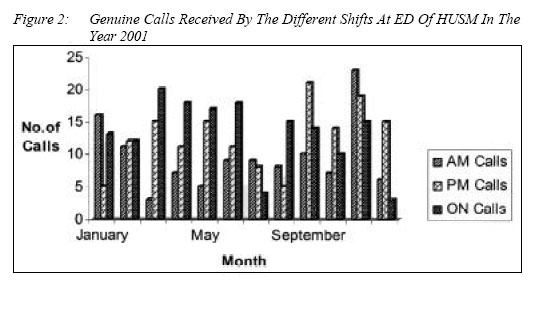
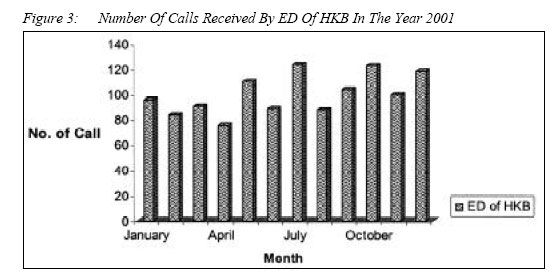
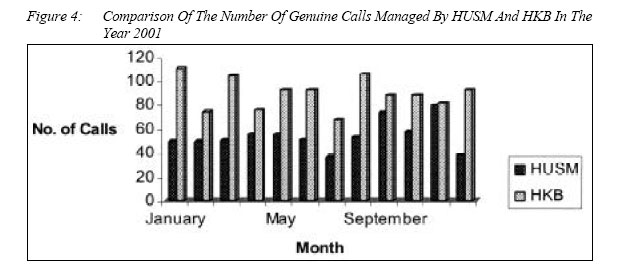
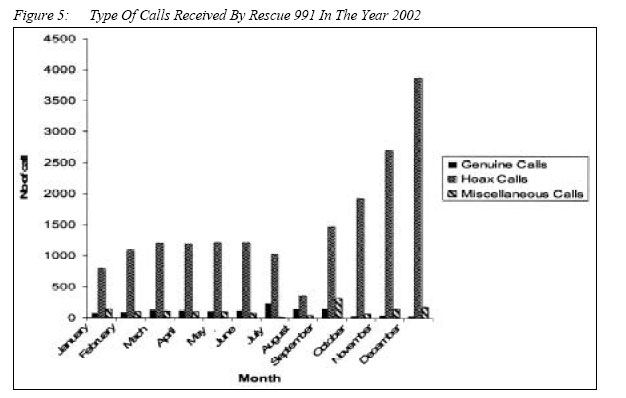
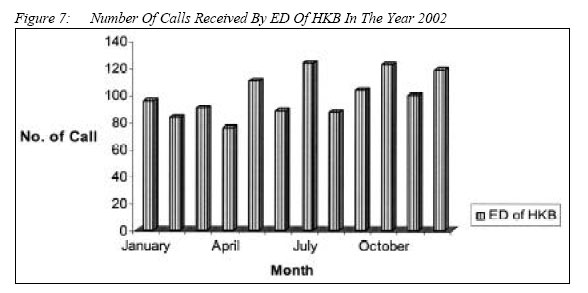
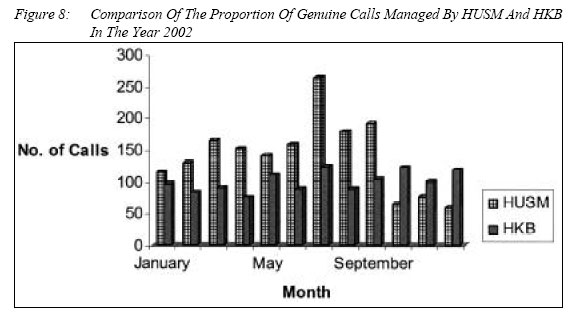
15586, Kota Bharu, Kelantan. Code Number: mj05018 This retrospective study attempted to identify the pattern of ambulance calls for the past two years at the Hospital Universiti Sains Malaysia (HUSM) and Hospital Kota Bharu (HKB). This study will provide a simple method of acquiring information related to ambulance response time (ART) and to test whether it met the international standards and needs of the client. Additionally, this paper takes into account the management of emergency calls. This included ambulance response time, which was part of Emergency Medical Services (EMS) episode: onset of ART, which started when details like phone number of the caller, exact location of the incident and the nature of the main complaint had been noted. ART ended when the emergency team arrived at the scene of incident. Information regarding ambulance calls from the record offices of HUSM and HKB was recorded for the year 2001 and 2002, tabulated and analyzed. There was a significant difference in the total number of calls managed by HUSM and HKB in the year 2001. It was noted that 645 calls were managed by HUSM while 1069 calls were recorded at HKB. In the year 2002, however, HUSM led with 613 extra numbers of calls as compare to HKB with 1193 numbers of calls. The pattern of ambulance calls observed is thought to possibly be influenced by social activities like local festivities, school holidays and the seasons. Further, it is observed that no studies were previously undertaken to compare the ART at both the HUSM and HKB to that of the international standards. In fact, a literature review undertaken so far showed no similar studies have been done for the whole Malaysia. Key words : Emergency Medical Services, Emergency Ambulance Services, Calls. Introduction Emergency Medical Services (EMS) system comprises of a comprehensive network of personals, equipment and resources established with the aim of delivering aid and emergency medical care to the community. These services are meant also to ensure that deliveries of care are partaken rapidly, effectively and with quality assurance. EMS efficiency can be measured in many ways. The most important way of looking at this system is by examining the whole process of EMS episode as mentioned by Guppy & Wollard (1). Meislin et al., (1999) defined the components of EMS episode based on timing as consisting of the following; receiving of a call, call processing time, control allocation time, crew mobilization time, traveling time to the scene, traveling time to the Emergency Department (ED) or hospital and ends with time spent at ED or hospital (2). In fact, the whole process of EMS episode plays a crucial role in determining service output. The EMS episode consists of 7 distinct period mentioned above with a component named ‘response time’ consisting of 3 components namely, control allocation time, crew mobilization time and traveling time to scene (3). The crucial determinant of successful EMS episode can be illustrated clearly with cases of out of hospital cardiac arrest patients. The concept that time interval between getting early initial treatment at the so-call ‘golden hour’ phase provided by ambulance crews has a greater effect on the morbidity and mortality rate of the victim or patient. A North American study stated that every minute delay in the initiation of cardio pulmonary resuscitation (CPR) during cardiac arrest for example, could increase the mortality and morbidity rate by up to 7 to 10% (4). Ambulance response time is undoubtly one of the parameters usually used in measuring EMS efficiency. Pell et al.,(2001) stated that in the United Kingdom, ambulances are expected to arrive at the designated scene within 7 to 14 minutes for 90% of the calls received (5). In addition, Breen et al., (2000) found that 14% of calls took 5 minutes or longer to activate response while 38% of emergencies obtained responses within 9 minutes. Further, it was noted that only 4.5% of emergency calls originating from places greater than 5 miles from the ambulance bases responded to within 9 minutes (6). Narad & Driesbock (1999), in their study on all California local EMS agencies had shown that only 57% of Californian counties ambulance services regulate their response times. Many of the ambulance enforcement programs in California have enforcement mechanism that is unlikely to promote compliance. Therefore, response time regulation is intended to improve the effectiveness of the EMS system in pre hospital care (7). Studies done in Perth, Australia shows similar finding. It was found that the trend in occurrence and survival following out of hospital cardiac arrest are similar to those found elsewhere (8). Another study was also done with the objective to determine the relative effectiveness of differences in response time interval, proportion of bystander Cardiopulmonary Resuscitation (CPR) and type and tier of EMS system on survival after out of hospital cardiac arrest (9). They concluded that increased survival rates of these patients upon discharge from the hospital might be associated with decreased response time interval and the used of two tier EMS systems as compared to a one-tier system. Another call-response interval study was done in the Turkish city of Ankara with the aim of trying to determine the various times related to the ambulance activities of Ankara Emergency Aid and Rescue Services (EARS) (10, 11). These authors expected that results of their studies might contribute to the improvement of the EMS system. A descriptive study was planned to determine various times related to the ambulance activities of Ankara EARS. The variables of the study were: delay time, response time, time at the scene (scene time), round trip time, transport time and total run time of Ankara EARS ambulance activities. The median response time of Ankara EARS was found to be 9 minutes. In the research year, the median delay time was 2 minutes. Median arrival time to patient contact time of Ankara EARS was 2 minutes. Median time at the scene was 7 minutes. Median round trip time of the system was 44 minutes. The median time for the arrival at the scene from the ambulance station was 8 minutes. The median transport time was 10 minutes. The median total run time was 30 minutes. As the median response time was found to be 9 minutes it is concluded that there should be more ambulance vehicle to improve this response time for Ankara EARS. It is observed, that due to financial problems the ambulance crew and dispatchers of Ankara EARS recorded their times manually (10). These authors also concluded that if digital and electronics recording systems were utilized, time recordings could be more precise. Based on a report commissioned by The Ministry of Health and Social Affairs of Norway, Steen-Hansen et al., (2000), proposed that standards for ambulance response intervals in emergencies if performed would be able to assess the current ambulance response interval (12). The report also proposed that an ambulance should reach 90% of the population in cities and urban areas within 8 minutes, whilst in rural areas, 90% should be reached within 25 minutes. The study concluded that the proposed standard was not achieved in any of the municipality in the country. However, the city of Tonsberg having shown the best performance can only achieved 48.9% of the populations where ambulance reaches their destination within 8 minutes. In Singapore, a study conducted just over a decade ago had ascertained the time it took for ambulance team to reach a patient and transport the patient to an emergency department after an emergency call (13, 14). It was reported that it took an average of 11.40 ± 4.88 minutes for an ambulance team to reach a patient and 30.50 ± 10.62 minutes for the patient to reach an emergency department. At the level of staffing in Singapore at that time, the basic life support care starts around 11.40 minutes whilst advanced life support care started 30.50 minutes after an emergency call. In Malaysia, no published studies related to ambulance services and their efficiency was found so far. It is reasonable, therefore, to conclude that any study in Malaysia would be novel. Like other developing countries, the Malaysian government subsidizes a substantial portion of the healthcare cost. There is, however, a lack of effort and money spend towards the development of pre hospital care component such as ambulance services as compared to expenditure and concern given to the public health and in-patient care. Throughout Malaysia, the government through Ministry of Health is the main provider of ambulance services. These ambulance services are hospital based and manned usually by a driver, hospital attendant and assistant nurse or staff nurse or medical assistant. In light of the above situation, it was thought that a retrospective study on ambulance calls in the Emergency Department of Hospital Universiti Sains Malaysia (HUSM) and Hospital Kota Bharu (HKB) would be appropriate as a pilot study. The need for this kind of studies was thought to be long overdue since the HKB ambulance services started in 1960, while HUSM since the hospital started services in 1983. No formal study was done at these places to either determine the efficiency or the extended services of the EMS in Kota Bharu region. The present study is an attempt at collecting and analyzing data recorded at both hospitals over a period of two years (2001 and 2002). Results obtained may then provide background information for further studies. MethodsRecords at the Emergency Departments of HKB and HUSM were collected and discussion with ED staff at the both places were undertaken. The information gathered from these discussions together with recorded data were collated and analysed. Since the year 2000, a squad called Rescue 991 under the Jabatan Pertahanan Awam Malaysia (A special government body established to assist in all emergency and disaster event in Malaysia) was located at ED of HUSM. Their specific aim is to help extend social work services to the public including ambulance services. These services include emergency cases or non-emergency cases. This arrangement is unique and only exists in HUSM, whereas, in HKB these kinds of services were purely undertaken by the hospital staff. Information gathered from HUSM must therefore be combined together with some record from Rescue 991 unit. All data from the records office at HUSM and HKB were collected loaded to the computer and analyzed using Microsoft Excel‚. Information regarding ambulance calls recorded were for the year 2001 and 2002. Results Record for the year 2001Upon examination of previous recorded data at the Emergency Departments (ED) of HUSM and HKB, a retrospective study on ambulance calls was performed. At the HUSM, two groups of data were collected - from Rescue 991 records and from records of ED of HUSM. In 2001, Rescue 991 received a total of 10,170 of calls. Out of the total number of calls, there were 231 genuine calls while a whooping 8871 calls were hoax and the rest were categorized as miscellaneous calls The numbers of genuine calls were noted to be lower in the months of December to July but were almost double in the months of August to November. Whereas, hoax calls were consistent for the whole year. April, September and November were the peaks months. This correspond to the school holiday period and may explain the high number of calls. July to September was the peak in the miscellaneous call category (Figure 1a) In ED of HUSM, a total 338 of calls were noted and managed subsequently by them in the same year. This information is shown as divided shifts. The morning shift (7am to 2pm) shows the highest number of calls in November while March shows the lowest. The afternoon shift (2pm to 9pm) registers the lowest number of calls in January and August while the highest was in September. Lastly, the night shift (9pm to 7am) shows that the highest numbers of calls were in March to June while December is the month that received the lowest number of calls. (Figure 2a). It can be concluded that there were not many differences in term of the number of calls for the whole year. The ED of HKB on the other hand managed to receive a total of 1069 ambulance calls in 2001. The months of January, March and August had a total number of calls exceeding more than 100. The highest numbers of calls were in January with 110 calls, followed by August with 105 and March with 104. The lowest number of calls for year 2001 was in July with only 67 calls. Four peaks were seen in the yearly tabulation of the number of calls. This was seen in January, March, May, June, August and December while July recorded the lowest number of calls (Refer figure 3a). There was a large difference in the total number of calls managed by HUSM and HKB in the year 2001. 645 calls were managed by HUSM while 1069 calls were recorded at HKB. HKB consistently managed a higher proportion of calls in almost every month, except for November (Figure 4a). Records for the years 2002In a year 2002, the data was different especially in a total number of calls. The total number of calls received by Rescue 991 increased to 20669. Out of the total calls only 1254 were a genuine calls while a whooping 18039 calls were hoax and the rest were classifies as miscellaneous. The number of genuine calls was noted to be higher in the months of March to September with peak in July but troughs in October to December. Monthly total numbers of hoax calls were more than one thousand except in the months of August (356 calls) and January (795 calls). Miscellaneous calls registered saw July and December as the months with the lowest number of calls at 7 and 179 cases respectively while the highest was December with 179 cases (Figure 5a). ED of HUSM managed to receive 552 calls in 2002. This is tabled accordingly with shifts. The morning shift shows the lowest number of calls in March and May while January and February show the highest. Afternoon shift shows that monthly total number of calls exceeded 10 except for the month of January, July and August. Night shift calls show peaks in March and become lowest in July (Refer figure 6a). ED of HKB received a total 1193 number of calls. The months of May, July, September, October and December recorded more than 100 numbers of calls with the highest being in July (123). April is the month with the lowest number of calls (75). Figure 7a shows that there were several peaks in the number of calls for the year 2002. They were in January, May, July, October and December, while April registered the lowest. There were obvious differences between the activities at the HUSM and HKB. HUSM received 613 numbers of calls, which is more than HKB for that year. The month of July received the highest number of calls at both hospitals but the lowest for HKB was in April whereas for HUSM it was in October (Figure 8a). DiscussionInformation regarding ambulance calls recorded for the year 2001 and 2002 at both hospitals; HUSM and HKB show that there was an increase in the percentage of calls for both the hospitals in a year 2002. HKB experienced an 11.6 % increase in the number of calls whilst HUSM showed an increase of 180%. The huge increase in HUSM figure is explained by the existence of the special squad called Rescue 991 under the Malaysia Department of Civil Defense (A special government body established to assist in all emergency and disaster events in Malaysia) was located at HUSM ED since 2000. Their specific aim is to help extend social work and services to the public including ambulance services. This arrangement is unique and only exists in HUSM, whereas, in the HKB this services were purely undertaken by the hospital staff. Information gathered from HUSM must therefore be combined together with some record from Rescue 991 unit. Apart from the increased in the percentage of the number of calls for the year 2002, the result of this study also showed that there were peculiar pattern of calls at both hospitals. The pattern of ambulance calls at the both places; HUSM and HKB looks similar and it was observed that it might be due to the yearly social activities like festivities, school holidays and climatic seasons. For an example, in the year 2001, the total number of calls was increased in February and March. These periods coincide with the celebration of the Hari Raya for Muslims and the Chinese New Year for the Chinese. In the months of September to December, the same pattern was observed. These increases in the number of calls are attributed to the wet season experience in the state of Kelantan. By looking at the total number of ambulance calls per capita within a 2-year period of study, it was noted that the district of Kota Bharu, Kelantan with a population of 266,000 had a ratio of 1:155 for the year 2001 and 1:89 in the year 2002 (15-18). Taking all these information together the results obtained confirmed that the district of Kota Bharu is relatively not a busy area in terms of the number of emergency cases. In the absent of any published data in other areas in Malaysia, a comparison can only be done with that of internationally established data. For example is Canada, the Emergency Medical Services of Manitoba (2002) reported that some Regional Health Authority (RHA) in that particular area received a significant number of ambulance calls per-capita in the year 2002. These RHA are Assiniboine, which recorded a ratio of 1: 13 from a total population of 71,497 people, Brondon had 1: 12 (populations 47,652), Burntwood recorded a ratio of 1: 7 from populations of 44, 806 and lastly, Winnipeg showed a ratio of 1: 1.2 (populations of 65,728) (19). Smith (2001) in his study found that rural area in Australia with population of 413,026 people managed to receive a total of 20,000 ambulance calls for the years of 1996 and 1997 (20). Thus the ratio of number of calls to population of 1: 20.7 seem to indicate a possible norm. As such the figures for district of Kota Bharu is low as compared to that of the international records ratios. This observation may be related to the absent of proper method of data recording for ambulance calls, lack of interest in calling for the ambulance services amongst the local population or perhaps the sheer lack of facilities to make the call. On the other hand it is also possible that data of ambulance calls and other information may be missing or left unrecorded. Our inquiries to the ambulance services at HUSM and HKB confirmed that differences in the recording system for telephony at these places could further complicate and may contribute to the lack of documentation. This situation correlates well with the findings of this study where it was found that there is no standard method of data recording for both the hospitals. Altintas & Bilir (2001) in their study also faced with a similar problem in Turkey (10). These authors mentioned that due to financial problems the ambulance crew and dispatchers of Ankara EARS recorded their times manually. This observation is further emphasized by another study in Japan where it was concluded that if digital and electronics recording systems were utilized time recordings can be more precise (21). The situation may be the same for HUSM and HKB in the Kota Bharu District. Emergency ambulance services are present at the both HUSM and HKB. However, as mentioned earlier, the quality of pre-hospital care services, especially emergency ambulance services is found neglecting due the possible lack of funds allocated for the development of vital components within this service. It is also possible that the lack of proper planning during the initial phase of the development of these hospitals could have contributed to this state of affair. Budgeting for these areas may be categorized as of low priority. Further, there were no single body or organization that has taken serious attention in this matter. This situation could be rectified by establishing an independent body to oversee all the Emergency services under one body as can be seen in most European countries and North America. In these countries, EMS is totally run by dedicated single body or organization. In the USA for example, they have a special body to take care of EMS system including ambulance services. Two studies stated that in the state of California, a special organization called The California Emergency Medical Services Authority (CEMSA) play the crucial part in managing Emergency Medical Services (EMS) in that state (22, 23). This Authority also trains ambulance personnel up to level of Emergency Medical Technician (EMT). They also develop protocols in the management pre-hospital care and prepare career pathways for their staffs, which include courses and programmed leading to bachelors and advanced degrees. Whereas in Malaysia, the EMS is totally run by the same personal who are also hospital staffs. The drivers, medical assistants and staff nurses are all under the hospital payroll and at the same time given task to manage EMS. This system is seemed to be difficult to run properly. It is suggested, therefore, that there should be a dedicated body with their own staffs managing the EMS system, which is thought to be the best way to preserve better outcomes (24). The present study pre-empt that ambulances services in the local setting may require modifications and adjustments if not a major overhaul. The philosophy and function of EMS system in Malaysia is still unclear and substantial attentions from the authorities are needed. No studies have been reported with regards to the efficiency of neither the emergency services nor the ambulance response time at these two hospitals under study. In fact no similar studies have been done for the country. In the absence of formal study to determine either efficiency or the extended services of the EMS system in Kota Bharu region, it is reasonable; therefore, to conclude that this paper may provide the initial impetus towards a more detailed and comprehensive analysis of the EMS in Malaysia. AcknowledgementsThe authors would like to thank the Emergency Departments (EDs) of HUSM, HKB and Jabatan Pertahanan Awam Cawangan Kelantan for their support and permission to use their records. References
© Copyright 2005 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj05018f6.jpg] [mj05018f8.jpg] [mj05018f5.jpg] [mj05018f3.jpg] [mj05018f1.jpg] [mj05018f2.jpg] [mj05018f7.jpg] [mj05018f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}