 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
ORIGINAL ARTICLE IMPACT OF A SPREADING EPIDEMIC ON MEDICAL STUDENTS Li-Cher Loh, Anita Mohd Ali, Ter-Hoay Ang, Ambiga Chelliah, IMU Lung Research,
International Medical University,
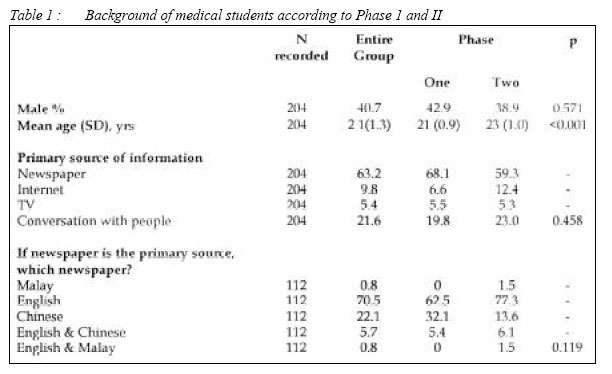
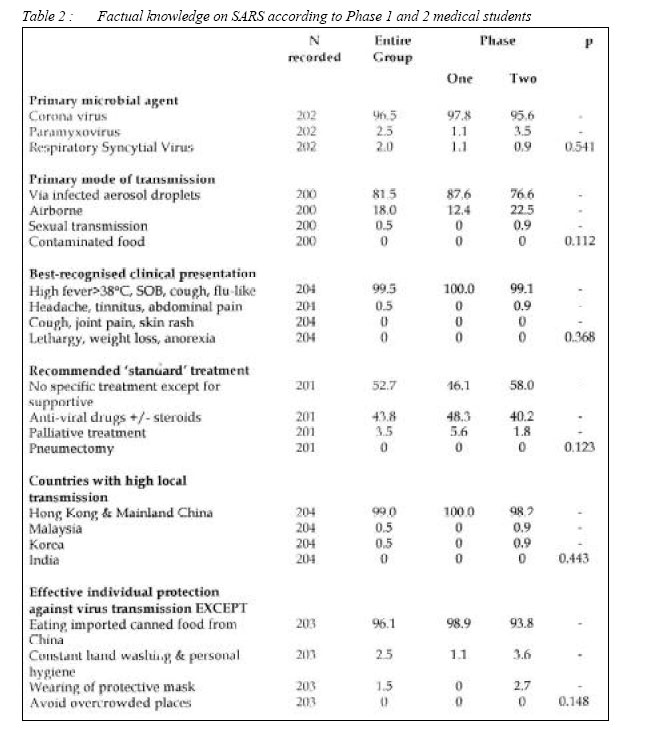
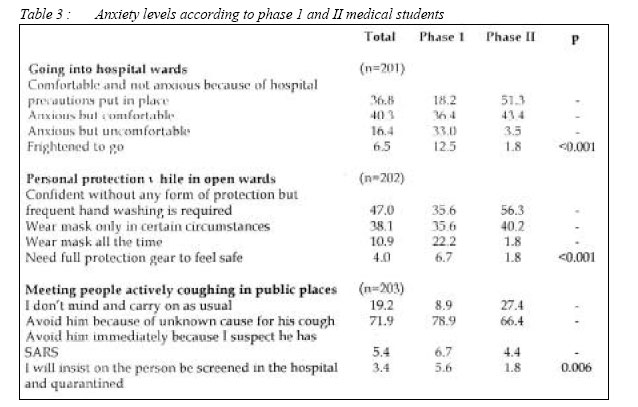
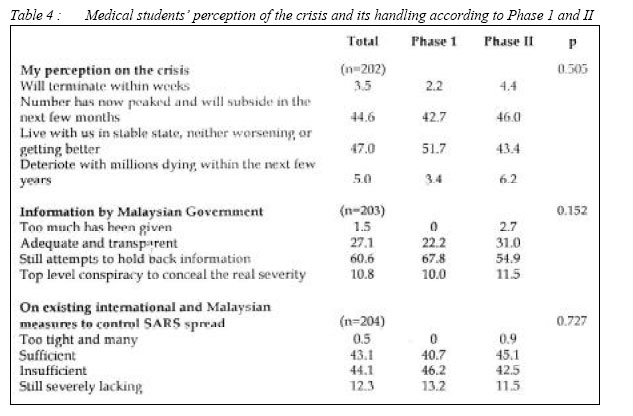
Clinical School, Seremban, Malaysia Code Number: mj05019 The emergence of severe acute respiratory syndrome (SARS) had caused fear and anxiety of unprecedented proportion. To examine the impact of SARS on the medical students in a private medical university, a self-reporting questionnaire study was carried out to assess the factual knowledge, anxiety level and perception of the crisis, among the students. The two-week study (between 12 and 23 May, 2003) was carried out three weeks after the first reported SARS-related death in Malaysia. Ninety-one Phase I (junior) and 113 Phase II (senior) students completed the questionnaires. A large majority of students of Phase I and II were correct in their factual knowledge and were sensible in their perception of the future and the handling of the crisis by government(s). However, phase 1 students expressed significantly greater degree of anxiety compared to Phase II in relation to attendance and personal protection in hospital, and in meeting people coughing in public places. The lesser degree of anxiety expressed by phase II senior students may be due in part, to a more realistic assessment of SARS risk brought about by maturity, time spent in hospital and interaction with clinical lecturers and medical staff. Key words: severe acute respiratory syndrome, SARS, medical students, knowledge, anxiety, perception, Malaysia Introduction On the 15th March 2003, the World Health Organization issued a rare emergency travel advisory as a global alert to a readily transmissible new respiratory disease, named Severe Acute Respiratory Syndrome or SARS. It showed clear capacity for spread along the routes of international air travel and in densely populated areas. Countries and cities especially Hong Kong, Beijing, Toronto, Singapore and Taiwan had suffered severe socio-psychological and economic consequences from the rampage of SARS (1). Although there had not been any local transmission of SARS in Malaysia, its close travel ties with the surrounding countries and cities affected by SARS, in particular Singapore, had caused much concern and anxiety among the Malaysian public and healthcare workers. During the crisis, the medical students’ teachings in hospitals in Hong Kong (2), Toronto (3) were completed halted because of SARS epidemic occurring in these sites. In our private medical university, while hospital teaching for students continued, there was a heightened emphasis for stringent infection control measures such as meticulous hand washing, appropriate use of respiratory mask, and banned entry to designated SARS isolation wards. We also banned all teachings in Accident & Emergency Departments of our three teaching hospitals and the entry points of universityaffiliated health clinics where the screening of suspected SARS patients occurred. Furthermore, all student electives to all SARS-affected areas were prohibited. One of the authors (LCL) of this paper chaired a medical advisory panel that was established to make recommendations to the university on SARS-related policies for staff and students. The author conducted an urgent three-day compulsory briefing for all students (Phase I and II) during the start of the SARS epidemic in March 2003, on the precautionary steps against SARS and the university policies of ensuring student safety. To investigate the impact of the SARS crisis on our medical students, a questionnaire study was conducted among the undergraduate students overa two-week period (between 12 and 23 May, 2003), initiated three weeks after Malaysia reported its first SARS-related death (accumulative figures at study commencement were two SARS-related death and six probable SARS cases). While there was no evidence of local transmission in Malaysia then, other areas such as China, Hong Kong and Singapore were facing a hard time to contain local transmission of SARS disease (4). The objective of our study were twofold: first, to examine the factual knowledge, anxiety level and perception of students on the current SARS crisis; second, to compare between the Phase I and Phase II students, their factual knowledge (based on the current understanding of SARS then), anxiety level and the perception of the future for SARS and the handling by the international and Malaysian governments. In our curriculum, students are exposed to hospital ward teaching from first year and the amount of hospital ward teaching increases exponentially from the second half of the third year when they enter Phase II. On average, Phase I students spent about half a day in one or two weeks in hospital ward teaching, interacting with real patients. Phase II however would spend almost everyday in hospital or health clinics with real patients as the requirement for Phase II curriculum. We tested the hypothesis that Phase II students, compared to Phase I, had better understanding of SARS but were more anxious about the risk of exposure to SARS because of their time spent in hospital wards. We also hypothesized that Phase II students had a more realistic perception on the future for the crisis and about the actions taken by the international and Malaysian governments. Subjects & MethodsTwo hundred and twenty medical students [consisting of the Phase I Semester 3 & 5 students (n=100) and Phase II Semester 7 & 9 students (n=120)] of the International Medical University, Malaysia, were invited to participate in a selfreporting questionnaire study. The rationale for choosing these groups was because they had completed one year into their respective phases. The two-page questionnaire were completed anonymously and consisted of closed questions relating to students' background, their level of factual knowledge on SARS (based on the understanding of the disease at that time), anxiety level during hospital attendance and in public places, and their personal perception on the SARS future and the handling by the international and Malaysian governments. Respondents answered from categories of answers, some of which requiring a 4point scale (e.g. questions related to anxiety level and perception of severity). A pilot study of the questionnaires was carried out with 5 medical students and 3 doctors and amendments made wherever necessary. Incorrectly filled questionnaires (n=16) were excluded from analysis (e.g. two answers were given when only one answer was asked for). Differences in results between the Phase I and II students were assessed using two-tailed Chi Square tests (or two-tailed Fisher exact tests when the expected cell frequency was less than five). A p< 0.05 was considered as significant. The analysis was performed with statistical software, SPSS' Version 11.0 for Windows. ResultsTwo hundred and four students [91 Phase I (60.6%) students and 104 (69.3%) Phase II students] completed the questionnaire satisfactorily. Of the respondents, nearly 60% was female. The gender differences between the two groups (Phase 1 and II) were comparable. Mean age in Phase II was significantly higher than in Phase I. Most derived their information from newspaper (63%), followed by conversation with people (21%), internet (9%) and TV (5%). Of the 112 students who selected newspaper as their primary source of information, 70% read English newspaper and 22% used Chinese newspaper. The proportions were comparable between the two groups (Table 1). Almost all (96%) quoted Coronovirus as the primary microbial agent implicated in SARS. There was one student from each group who wrongly implicated Respiratory Syncytial Virus. 81% correctly reported infected aerosol droplets as the primary mode of transmission while 18% reported 'airborne'. One student in Phase II was completely wrong by reporting 'sexual transmission'as the primary route of transmission. Almost all (99%) correctly reported high fever ≥ 38 ∞ C, breathlessness, cough and flu-like symptoms, as the 'best-recognised'clinical presentation. Most correctly identified 'no specific treatment except for supportive'(52%) and 'anti-viral drug +/- steroids' (43%) as the recommended standard treatment. For countries with high local transmission, almost all (99%) correctly stated Hong Kong & Mainland China. In Phase II group, one wrongly stated Malaysia and another one stated Korea. On the exception to effective individual protection against transmission listed, most (96%) corrected selected ‘eating imported canned food from China' . However, one student from Phase I and four students from Phase II selected ‘constant hand washing and personal hygiene' as their answers, while another three in Phase II selected ‘wearing of protective mask' . The selection of wrong answers for these students was likely to be due to misinterpretation of this question where the exception was asked for. In all these questions, the answers were comparable in both groups of students (Table 2). Questions concerning going into the hospital wards revealed that 40% were anxious but comfortable about this, while 36% were comfortable and not anxious due to the hospital precautions put in place. 16% were anxious and uncomfortable about going while 6% were frightened to go. There was a significant difference between the two groups in that over 90% of the Phase II students were comfortable about this, compared to just over 50% of the phase I students, and about 45% of Phase I students were either uncomfortable or even frightened to go into hospital, compared to only 5% in Phase II (Table 3). Regarding personal protection in open wards, 47% were confident without any form of protection but would exercise frequent hand washing, and 38% would wear mask only in certain circumstances. 10% would wear mask at all times while 4% would need full protection gear in order to feel safe. The pattern of answering was significantly different between the two groups in that over 96% of Phase II students were confident without any form of protection or wear mask only in certain circumstances, compared to about 72% in Phase I. Similarly, about 3% of Phase II students would wear mask at all times or require full protection gear in order to feel safe, compared to almost 30% in Phase I (Table 3). When meeting people in public places who actively cough, most (71%) would avoid him because of the unknown cause for his cough. 19% stated that they would not mind and would carry on as usual, while some would avoid him immediately because of suspicion of SARS (5%) or insist on the person be screened in the hospital and quarantined (3%). There was significant difference between the two groups in that compared to Phase I, proportionately more students in Phase II would either carry on as usual or avoid active coughers because of unknown cause of his cough, and proportionately fewer in Phase II would suspect that active coughers had SARS or insisted on screening and quarantined in hospital (Table 3). With regards to perception on the future of the crisis, 47% stated that SARS would live in human population in stable state, neither worsening or better, while 44% stated that the number had now peaked and would subside in the next few months. Small proportions stated that the crisis would terminate within weeks (3%) or deteriorates with millions of people dying within the next few years (5%). The pattern was similar and comparable in both groups of students (Table 4). More than half the students (60%) believed that there had been attempts by the Malaysian government to hold back information, while about a quarter (27%) reckoned that the government had been transparent and their information adequate. Around 10% believed that there was a top-level government conspiracy to conceal the true degree of severity while very few (1%) felt that too much information had been provided to the general public. The pattern was similar in both groups of students (Table 4). With regards to the measures taken by international and Malaysian governments to control SARS, almost similar proportions of students reckoned that they were sufficient (43%) and insufficient (44%). 12% of the students perceived that the measures were severely lacking, while only one student from the Phase II group reckoned that they were too tight and many. Overall, the two groups were comparable in these (Table 4). DiscussionWe have shown that while a large majority of students in both groups was correct in their factual knowledge and sensible in their perception of SARS crisis, Phase I students compared to Phase II, expressed greater degree of anxiety about being in hospital, adequacy of individual protection against SARS and meeting people who cough in public places. A small but comparable proportion of students in both groups were pessimistic about the future outlook on SARS and some 10%, from both groups, were highly suspicious and critical of governments' dealing with public information and the control measures. Fear and anxiety caused by spreading epidemics of known or unknown diseases can have damaging consequences on people and economy. Never before in the era of modern world with its advances in medicine has a disease like SARS that had caused a psychological impact of such global scale (1, 5-6). At the stage of the study, the public and healthcare worry was at its peak with countries like Hong Kong, Singapore and parts of China struggling to contain the escalating number of local cases. Our key teaching hospital, where both phases of students attended for ward teaching, was a designated SARS hospital for Malaysia where suspected cases were sent in for screening and isolation. As such, students and parents alike were understandably concerned of the possible risk of contracting SARS and about the adequacy of hospital screening and control measures. Contrary to our hypothesis, both phase I and II students showed comparable level in their understanding on SARS, and perceived similarly on SARS future and its handling by governments. Surprisingly however, phase I students, compared to phase II, were much more anxious about being in hospital and about the crisis. This discrepancy in their level of anxiety could not be explained by their source of information or the types of newspapers they read since these variables were not significantly different in both groups. One plausible explanation is that Phase I students, compared to Phase II, exhibited greater degree of health anxiety. Health anxiety refers to the phenomena of medical students having excessive anxiety about their health that had often lead to frequent request for medical consultations and sometimes, needless investigations. It has been termed variously as medical student' s disease, nosophobia and medicalstudentitis (7-8). While the existence of such a condition in medical students is still debatable (9), there is no evidence to show that junior students experience this to a greater degree than their senior counterparts, or even a suggestion of this. Another explanation may be simply the fact that Phase II students, by having more contacts with the hospital, clinical lecturers and medical staff, had a more realistic assessment of the SARS risk. They might have also observed first hand the stringent measures put in place for the screening and isolation of suspected SARS patients. This in turn helped to build confidence and provide reassurance that the risk of contracting SARS was minimal. Finally, the chronological maturity of Phase II students in medical knowledge and as an individual, compared to Phase I might play some role in avoiding excessive anxiety in these circumstances. In one study on Hong Kong medical and nursing students (10), it is worth noting that when compared to nonhealthcare students, they exhibited a significantly greater degree of anxiety and psychological stress. In general, most students of both the phases held realistic view on the future for SARS in that the answers selected were a reflection of the feelings among the experts at that time. A majority of students from both phases appeared skeptical at the government information on the statistics of cases presented to the general public, and some 10% from both groups would even believe that there had been top-level conspiracy to conceal the true severity. This is perhaps understandable, considering what previously had taken place in Malaysia where some degree of deliberate concealing of information by the government was deemed necessary. The students appeared to be ‘divided' in their perception of the adequacy of infection control measures put in by WHO and Malaysia. Looking back now, it is obvious that they had worked, supporting the notion that they were adequate at the time. Our novel findings from this study implies that there is a need to address the anxiety status among the medical students that goes beyond the imparting of factual knowledge. The training needs between the junior and senior students may require to be probed into separately in the overall effort to improve the training of our future medical doctors. Perhaps, as what was said by Professor Sydney Chung, Dean, Chinese University of Hong Kong during the crisis 'It is precisely at the time of such a major medical crisis that educating the next generation of doctors becomes so important' , it may be apt for us to think of ways to use such future crisis as an opportunity to better educate our medical students (2). AcknowledgementsThe authors acknowledged with thanks the help from the Student Council, International Medical University and class representatives of Semester 3, 5, 7 and 9, in facilitating the distribution and collection of the questionnaires. References
© Copyright 2005 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj05019t4.jpg] [mj05019t3.jpg] [mj05019t1.jpg] [mj05019f1.jpg] [mj05019t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}