 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
CASE REPORT THE CO-EXISTENCE OF PURE RED CELL APLASIA AND AUTOIMMUNE HAEMOLYTIC ANAEMIA IN A CHILD WITH MALIGNANT LYMPHOMA Suhair Abbas Ahmed & Rosline Hassan Department of Haematology,
School of Medical Sciences, Universiti Sains Malaysia, Health Campus
16150 Kubang Kerian, Kelantan, Malaysia Code Number: mj05021 The association between pure red cell aplasia (PRCA) and autoimmune haemolytic anaemia (AIHA) has rarely been reported. PRCA represents an isolated process, characterized by normochromic, normocytic anaemia, reticulocytopenia and erythroid hypoplasia in the bone marrow, and may be attributable to infection with Parvo virus B19. AIHA is a condition in which peripheral red blood cell destruction is induced by the presence of autoantibodies. However, the co-existence of these conditions is very rare, since only few cases of PRCA and AIHA associated with malignant lymphoma (ML) were reported. A case of PRCA and AIHA was detected and described, for the first time in Malaysia, in a 10-year-old child suffering from non-Hodgkin lymphoma from the Department of Haematology, Universiti Sains Malaysia. Following the induction course of chemotherapy, the patient turned anaemic, with tendency for red cell clumping, reticulocytopenia and anisocytosis. AIHA was suspected in spite of the weak Coomb reaction obtained. The bone marrow aspirate revealed the presence of giant pronormoblasts, suggesting PRCA. Serological tests for Parvo virus and other viruses were negative. Key words : pure red cell aplasia, autoimmune haemolytic anaemia, malignant lymphoma. Introduction PRCA represents an isolated process, characterized by normochromic normocytic anaemia, reticulocytopenia and erythroid hypoplasia in the bone marrow. It has been attributed to infection with Parvo virus B19 (1,2,3). AIHA is a condition where peripheral red blood cell destruction is induced by the presence of autoantibodies (1). The combinations of these conditions are very rare, since only few cases of PRCA and AIHA associated with malignant lymphoma (ML) have been reported (4,5,6,7). In this report, a rare case of co-existence of pure red cell aplasia (PRCA) and autoimmune haemolytic anaemia (AIHA) in a child suffering from non Hodgkin lymphoma has been detected and described at the Haematology Department, Hospital UniversitiSains Malaysia. Case Report The patient was a 10-year old Malay boy who is a known case of non-Hodgkin
lymphoma (T-cell type), stage IV, first diagnosed in February 2002, with
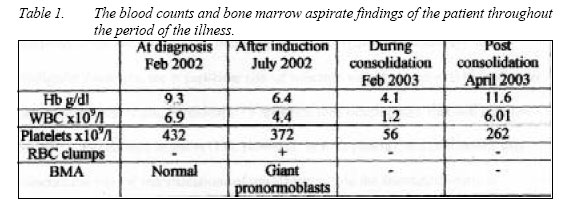
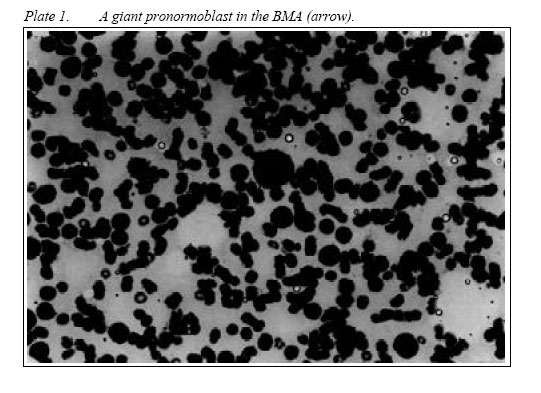
pulmonary involvement. Histopathological examination of tissue obtained from biopsy of the During that time, the full blood picture of the patient showed features of mild anaemia (table 1). The blood film did not contain any blast cells or other abnormal cells. At diagnosis, bone marrow aspirate (BMA) and trephine biopsy were performed for staging purposes and showed a normal marrow with no evidence of infiltration by malignant cells.The patient was started on the EORTC-VHR protocol for ML on the 4th of March, 2002. After the completion of the induction course of chemotherapy in July 2002, the patient became more anaemic in spite of the supportive blood transfusions that he was receiving. His blood counts are shown in table 1. An important finding was the anaemia and the reticulocytopenia which were very low for the degree of anaemia. At the same time, the blood film examination revealed red cell clumping, in addition to the lowered red blood cell (RBC) count and anisocytosis. The diagnosis of a cold type AIHA was suspected and a haemolytic work-up was requested. The Direct Coombs test was weakly positive at room temperature, and the serum reactivity showed no definite specificity. The red cell clumping and the weak Coombs reaction both turned negative when tested one week later. Consequently, another BMA was performed to assess the progress of the disease and to look for a cause for the anaemia. Examination of the BMA smears revealed hypocellularity, with markedly suppressed erythropoiesis, and an estimated 4% of the nucleated elements in the BMA were giant pronormoblasts (plate 1). The presence of these giant pronormoblasts is usually associated with Parvo virus infection, and its confirmation requires specific diagnostic serological tests. Serological investigations for viral infections which included Epstein Barr virus (EBV), Cytomegalovirus (CMV), Hepatitis C virus (HCV), Hepatitis A virus (HAV), Hepatitis B virus and Parvovirus IgM and IgG were all negative. The patient was, then, maintained on supportive red cell transfusion for his anaemia.The Hb started to rise gradually reaching around 7 g/dl. Consolidation therapy was then started, and the patient was noted to develop pancytopenia which could be attributed to the chemotherapy. His counts at that time are shown in table 1. The patient was maintained on the chemotherapy with the support of blood products. He completed the consolidation therapy on 25/2/03. He was maintained on supportive blood and blood products therapy through out the period of the chemotherapy. His latest blood counts are shown in table 1. DiscussionParvovirus B19, is a member of the Erythrovirus genus. It is named so because of its tropism for and selective replication in erythroid progenitor cells. Haematological consequences of B19 infection arise due to direct toxic effects on erythroid progenitors in bone marrow with interruption of erythrocyte production (8, 9, 10). Immunocompromised children, including those undergoing chemotherapy for malignant disorders, are at particular risk of infection with Parvo virus B19 leading to transient aplastic crises. Persistent B19 infection may develop and that will manifest as PRCA and chronic anaemia (11). However, in such patients, the malignancy may obscure the clinical manifestations of the infection, and the attenuated immune responses may obscure serological detection (11,12,13,14,15).The serological tests for Parvo virus B19 were negative in this patient. However, the diagnosis of PRCA due to Parvo virus B19 infection was adopted on the basis of the presence of giant pronormoblasts since many reports have emphasized the lack of serological findings in patients with cancer, especially children (8,11,12,13). The method of transmission of parvovirus B19 is through respiratory secretions, though infection can also be transmitted by blood and blood products. Among blood donors, approximately 1:10 000- 1:25 000 units of blood during epidemic seasons contain high titres of B19 (8,9). For diagnosing a Parvo virus B19 infection, BMA should be examined, whenever possible (12). A general reduction or even absence, of erythroid precursors, is usually associated with sparing reduction in other bone marrow lineages. Giant pronormoblasts may be visualized and are highly suggestive of Parvo virus B19 infection. The diagnosis of Parvo virus B19 infection can be performed serologically, or by nucleic acid hybridization assays (14). Most patients with symptomatic infection would have more than 105 B19 virions/ml of serum, detectable by dot blot hybridization assays. In acute infections, B19 DNA is usually present at these levels for only 2-4 days . The detection of B19 DNA in serum samples obtained more than two days after the onset of anaemia suggests a chronic parvovirus B19 infection. The sensitivity level of detection of B19 is greatly increased by use of PCR, but has the risk of giving false positive results due to contamination (8). Ultimately, in this case, the diagnosis of Parvo virus B19 infection was not supplemented by any confirmatory test, and was made solely on the detection of giant pronormoblasts in the BMA. The cold AIHA which the patient developed in association with the PRCA was detected at the same time when the PRCA was suggested. Nevertheless, the weak direct Coombs test, and the absence of clinical signs and symptoms, in addition to the absence of an active haemolytic process, may all be due to the attenuated humoral immune response, as well as the reduced numbers of RBCs in PRCA (4,5,6). ConclusionsThis is the first case report of an association of PRCA and AIHA in a child treated for ML, in Malaysia. Parvovirus B19 should be considered as part of the differential diagnosis in any patient with anaemia associated with low or absent reticulocytes, especially in immunocompromised patients, even in the absence of positive serological tests. AIHA can occur in immunocompromised children but with a masked picture and can be transient. AcknowledgmentThe authors thank Dr. Fawwaz S. Al-Joudi, Department of Chemical Pathology, School of Medical Sciences, Universiti Sains Malaysia, for his assistance in the preparation of this case report. References
© Copyright 2005 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj05021f1.jpg] [mj05021t1.jpg] |
| |||||||||

{kind=link}
{kind=link}