 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
ORIGINAL ARTICLE TIME DELAY AND ITS EFFECT ON SURVIVAL IN MALAYSIAN PATIENTS WITH NON-SMALL CELL LUNG CARCINOMA Li-Cher Loh, Li-Yen Chan, Ru-Yu Tan, Selvaratnam Govindaraju*, Kananathan Ratnavelu*, Shalini Kumar**, Sree Raman***, Pillai Vijayasingham***, Tamizi Thayaparan*** Lung Research Unit, International Medical University, Clinical School, Seremban; * Nilai Cancer
Institute, Nilai; ** Department of Pathology, Seremban Hospital; ***Department of Medicine,
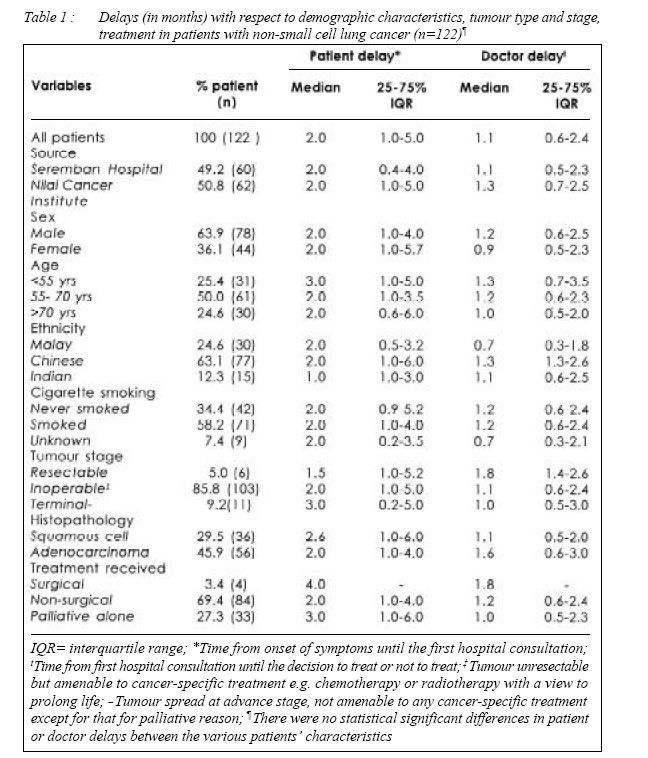
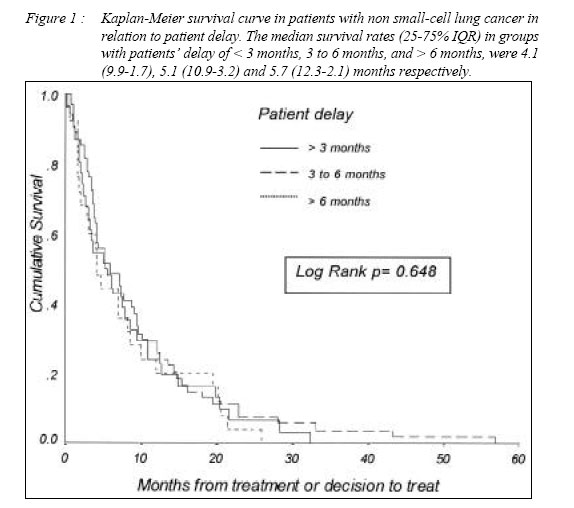
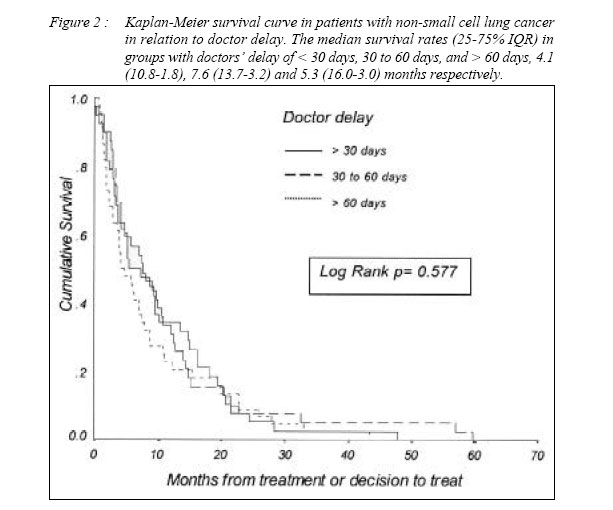
Seremban Hospital, Seremban, Malaysia Code Number: mj06007 While evidence indicates that early stage disease has better prognosis, the effect of delay in presentation and treatment of patients with non-small cell lung cancer (NSCLC) on survival is debatable. A retrospective study of 122 Malaysian patients with NSCLC was performed to examine the presentation and treatment delay, and its relation with patient survival. Median (25-75% IQR) interval between onset of symptoms and first hospital consultation (patient delay) and between first hospital consultation and treatment or decision to treat (doctor delay) were 2 (1.05.0) and 1.1 (0.6-2.4) months respectively. The median survival rates in patient delay of <1, 1 to 3, and >3 months were 4.1 (9.9-1.7), 5.1 (10.9-3.2) and 5.7 (12.32.1) months respectively (log rank p=0.648), while in doctor delay, <30, 30-60, >60 days, the rates were 4.1 (10.8-1.8), 7.6 (13.7-3.2) and 5.3 (16.0-3.0) months respectively (p=0.557). Most patients presented and were treated in a relatively short time, and delays did not appear to influence survival. This Asian data is consistent with those from Western population, reiterating the need for public health measures that can identify disease early.. Key words : non-small cell lung cancer, Malaysia, survival, time delay Introduction The prognosis of lung cancer remains poor, with overall five-year survival figures varying between 5 and 10% worldwide (1). However, it has been shown that surgery in patients with early stage disease in non-small cell lung cancer (NSCLC) can achieve five-year survival rates up to 80% (2), while there is no evidence that immediate treatment of patients with unresectable locally advanced nonsmall cell lung cancer affects survival (3). What is currently debatable is whether time delay from onset of symptoms to treatment influences prognosis. Some studies have shown that delay adversely affects prognosis (4, 5), while others could not show any associations (6, 7). Published data from the Asia-Pacific region on time interval and its effect on survival in patients with NSCLC is lacking. Malaysia produced its longoverdue first national cancer registry in 2003. In its report, lung cancer is the commonest cancer in males and the fifth commonest in females (8). These rankings are very similar to the published figures from many western countries (9). Therefore, there is merit in considering what might influence and be responsible for this poor prognosis. The objective of this study was twofold: (1) to investigate the time interval between the onset of symptoms and first hospital consultation for suspicion of lung cancer (described as ‘patient delay’), and between first hospital consultation and treatment or decision-to-treat or not-to-treat (described as ‘doctor delay’), and (2) to examine the association between delay and survival in patients with NSCLC. Patients & Methods Data collectionUsing a structured data collection form, relevant information was retrospectively collected from medical records of patients with confirmed NSCLC between 1 January 1996 and 1 April 2004, in two urban-based hospitals (Seremban General Hospital and Nilai Cancer Hospital) in Malaysia. Patients, with their NSCLC histology types, were first identified from the pathology database of the Department of Pathology, Seremban Hospital and the Cancer Register, Nilai Cancer Institute. Their medical records were then retrieved for perusal. Data on tumour stage, date of onset of first symptoms as stated by the patient, date of first hospital consultation, date of treatment (or decision-to-treat or not-to-treat if date of treatment was not available or not applicable) and the type of treatment received by the patients, were obtained from these patients’ medical records. Patients whose records indicated that the lung involvement was metastasis, were excluded from the study. The protocol of the study was approved by the local university Research & Ethics Committee and carried out in accordance to the recommendations of the Helsinki Declaration of 1975. Tumour stageFor the purpose of data collection, patients were categorized into those : (1) whose cancer was amenable to resection ; (2) Those with unresectable, locally advanced tumours cancer that were amenable to non-surgical cancer-specific therapy, i.e. chemotherapy, radiotherapy or both, with the intention of prolonging life; and (3) with terminal disease, where only palliative treatment was recommended. Broadly, they were consistent with TNM Stage I to II, III and IV respectively. The reason for this approach was because many records in Seremban Hospital did not state the TNM classification. Survival statusSurvival status was ascertained from followup visits in medical outpatient clinics, and if necessary, by direct contact with patients or nextof-kin by telephone. Patients whose survival status could not be confirmed were excluded from the study. Data analysisDescriptive analyses were used to characterize all patients. Median delay (with 25% to 75% interquartiles, IQR) was calculated for each of the characteristics. As time intervals were not normally distributed, non-parametric tests were used. The Mann-Whitney test was used for pair-way comparisons of delay and the Kruskal Wallis test for analyses involving multiple groups. The cumulative and median survival rate was measured using Kaplan-Meier survival analysis and log-rank test used to study the difference in survival curves between groups with varying time delays. The time at risk will be accumulated from the date of treatment or decision-to-treat or not-to-treat, until death, or in those still alive, until 1 April 2004. All computation was made using statistical package SPSS version 11.5 for Windows (Chicago, Illinois, USA). In all cases, the significance was defined at the 5% level and two-tailed. ResultsOver this period of time, there were 158 patients diagnosed with NSCLC. However the medical records of only 133 patients could be retrieved. Final analysis was only possible in 122 patients, due to the problem of completeness of data in other records. The two hospitals contributed almost equally to the number of patients in this study. The majority of patients were male and half were between the ages of 55 and 70 years. The majority of the study population was Chinese, followed by Malays and then Indians. The majority of the patients were current or past cigarette smokers. More than onethird (34%) of the patients claimed that they had never smoked before. Only 6 patients (5%) had resectable NSCLC on presentation, while the large majority (85%) had locally advanced unresectable tumour. Another 11 patients (9%) had terminal disease. The main NSCLC type was adenocarcinoma (45%), followed by squamous cell carcinoma (29%). Only 4 of the 6 patients with resectable disease underwent surgery (two of whom were administered adjuvant chemotherapy and radiotherapy). Only 84 of the 103 patients recommended for chemotherapy and radiotherapy for locally advanced disease received treatment. Over a quarter of the patients (27%) received palliative treatment alone [Table 1]. Overall, the median (25-75% IQR) patient delay and doctor delay were 2.0 (1.0-5.0) and 1.1 (0.6-2.4) months respectively. There were no significant differences in time delay in relation to patients’ age, gender, ethnicity, smoking status, source of hospitals, type and stage of tumour and treatment received [Table 1]. The median survival rates (25-75% IQR) in groups with patient delay of < 3 months, 3 to 6 months, and > 6 months were 4.1 (9.9-1.7), 5.1 (10.93.2) and 5.7 (12.3-2.1) months respectively. Survival rates between these groups were not statistically significant (log rank p=0.648) [Figure 1]. The median survival rates (25-75% IQR) in patients with doctor delay of < 30 days, 30 to 60 days, and > 60 days, were 4.1 (10.8-1.8), 7.6 (13.7-3.2) and 5.3 (16.0-3.0) months respectively. Differences in survival rates between these groups were again not statistically significant (log rank p=0.577) [Figure 2]. DiscussionThis is the first study on Malaysia patients with NSCLC with regards to the time lapse between onset of first symptoms and treatment, and is probably one of the very few studies available in the South-Asian region. The study is timely in view of the recently released first National Cancer Registry for Malaysia that reported lung cancer as the commonest cancer in males and the fifth commonest in females (8). In our patients, the median time from onset of first symptoms to first hospital consultation was 2 months. With time lapse of another one to two months between presentation and treatment, our median delay from symptom onset to treatment is comparable to those reported by UK investigators (median 3.6 months) 10, and much shorter compared to other countries like Sweden (median 4.6 months) (11). This generally indicates that patients with lung cancer tend to seek help late because of their failure to recognize the significance of their symptoms. Our median time from first hospital consultation to treatment or decision-to-treat was 1.1 months. This figure is similar to those reported in other European countries like UK (12) and Sweden (11). Recommendations from these countries (13, 11, 14) generally advocate an interval of no more than four weeks between the initial visit to a doctor and confirmation of diagnosis, and another interval of not more than two weeks between diagnosis and the commencement of radical treatment such as surgery, curative chemotherapy or radiotherapy. It is somewhat of a surprise to note the short doctor delay in our study, because cancer-specific treatment (including surgery) is not readily available in many parts of Malaysia. It is likely that Seremban Hospital’s close proximity to the national cancer center in the capital Kuala Lumpur, and the fact that Nilai Cancer Institute itself is an oncology center, attributed to the relatively short delay. As such, our data may not be representative of most other hospitals in Malaysia. We did not find any significant association between the median delays by patient or doctor with patient gender, age, ethnicity (of the three main ethnic groups in Malaysia), smoking status, tumour type and stage, treatment received, or hospitals. More importantly, we did not find any significant difference in patient survival with relation to patient or doctor delay. Our findings corroborated with reports by others on doctors’ delay (6, 11, 15). In fact, Myrdal et al (11) in their large sample of 466 Swedish patients, showed that patients with advanced disease had shorter delay times compared to those with less advanced disease. The authors suggested that the severity of clinical symptoms and signs on presentation might be responsible for accelerating the medical decision process. The reason for the contradicting findings by other researchers (4, 5) that delay adversely affects survival is unclear. The study by Myrdal et al (11) and ours are probably the very few studies that have looked into the question of delay beginning from onset of first symptoms. The findings in both theirs and ours did not show that the time delay from symptom onset adversely affects patient survival. It suggests that by the time the tumour manifests itself with symptoms and signs, the patient’s prognosis with or without treatment may already be determined. The current understanding is that although tumour volume can expand exponentially within a short time (14), lung cancer tends to grow slowly, taking probably an estimated 130 months to reach a diameter of 1cm (16). As such, it may be assumed that patients with the best prognosis are those with the slowest growing tumours. As in most studies quoted here, our study is retrospective, with most of the key information obtained from patient medical records. However, the survival status in a substantial number of patients was confirmed by direct contact with patients or next-of-kin over the telephone. Inaccuracies or lack of information in some medical records were successfully rectified during the telephone interview. Nevertheless, date of onset of first symptoms could still be inaccurate, as this was based on the patient’s recall. In many records, the dates of treatment were not available, and therefore the dates of decisionto-treat or not-to-treat were used instead, as stipulated in our study protocol. In these patients who later received treatment, we are unable to ascertain whether there had been any significant time lapse between decision-to-treat and actual treatment. Nevertheless, we have no reason to believe that any misclassification in this respect would significantly affect our findings. Lung cancer remains one of the highestranking cancers in the world that carries a poor prognosis (9). Unlike other solid tumours where survival rates have improved in the order of 60-90% with new and advanced methods for early detection and treatment, the management of and the prognosis for lung cancer has changed very little over the last 20 years (17). Given the high prevalence of cigarette smoking in South-Asia and other European regions, lung cancer will continue to be a major public health threat in the next century. Reducing the time delay in diagnosis and treatment of lung cancer may not contribute substantially to improving lung cancer mortality. Dependence on tobacco control alone will not achieve any real milestones, since most newly diagnosed individuals are either former smokers or never-smokers. It seems obvious that finding an effective public health approach to diagnosing early or pre-cancerous stage of lung cancer would be a crucial step toward improving survival from lung cancer (18, 19). More research on this is required. AcknowledgementsThe authors wish to thank the support of Hospital Directors, Seremban Hospital and Nilai Cancer Institute for this research, and the permission of the Director-General, Ministry of Health Malaysia to publish the data from Seremban Hospital. The research is supported by an internal research grant from International Medical University. References
© Copyright 2006 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj06007f1.jpg] [mj06007t1.jpg] [mj06007f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}