 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
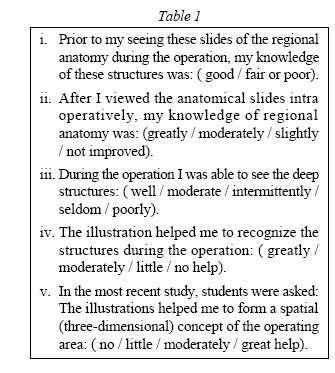
LETTER TO EDITOR THE ROLE OF ANATOMISTS AND SURGEONS IN CLINICAL ANATOMY INSTRUCTION INSIDE AND OUTSIDE THE OPERATING ROOM Correspondence: Dr. Nasir Aziz. MBBS(Pak), M.C.P.S.(Pak), M.Phil(Pak) Department of Anatomy School of Medical Sciences, Universiti Sains Malaysia, Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Tel : 609-766 3892 Fax : 609-764 7884 Email : nasiraziz@kb.usm.myCode Number: mj06014 Dear Editor,In undergraduate medical training, teaching of anatomy is increasingly needed in the fourth and fifth (clinical) years due to various reasons (1, 2) . A number of medical institutions have shortened the duration of gross anatomy in their curriculum with the introduction of newly emerging specialties in medical sciences (3). Anatomy is considered a prime learning issue in the operating room (2). Dissection of cadavers is no doubt the best mode of learning gross anatomy (even today) but medical illustrations, photographs, slides and posters of regional anatomy do play an important role from Vesalius in 1538 to the latest edition of Gray's Anatomy (4). These illustrations are very helpful to revise the knowledge of gross anatomy for the senior medical students as they provide visual positive reinforcement in the learning process. To facilitate clinical anatomy instruction in surgery and allied clinical sciences, the University of South Florida developed a system of instruction in which regional anatomy is taught both before and during surgical procedures in the operating room (5). Anatomists can play a very positive role to make this method more practical and effective for the students in two different ways. As the patient to be operated upon is prepared for surgery, medical students on duty can review the anatomy with the help of a surgeon and an anatomist using anatomical illustrations, radiographs, Magnetic Resonance Imaging and Computed Tomography (C.T) Scan of the relevant area of surgery. Occasionally patients are admitted on the same day of their surgery. The students who are allotted that particular patient may have forgotten the detailed anatomy of that particular region. Normal regional anatomy along with some of the common anatomical anomalies or variants can be demostrated with the help of slides, plastinated specimens and models before starting the surgery. The structures in layers to be dissected could also be demostrated during the operation. To start with, this method can be practiced for commonly performed operations such as nephrectomy, herniorrhaphy, laporotomy, cholecystectomy and fracture dislocations. During the operation, when it is safe for the patient, the operating team pauses to look at the illustrations pertaining to those phases of procedure. Students can be asked to identify the anatomical structures on the patient and confirm them from illustrations. There are many steps, from incision to removal of kidney during a nephrectomy procedure. The surgeon can ask the students about the structures encountered during these steps starting from skin to kidney. Similarly, students can view the illustrations of normal inguinal anatomy during herniorraphy. They may be asked to identify the external oblique, internal oblique and transversus abdominis muscles, inguinal ligament, ilio-inguinal nerve and vessels, internal inguinal ring and inferior epigastric vessels. These illustrations can give frontal, sagittal and three-dimensional views. A group of students can be requested to attend the anatomy museum one day before a specific operation is done where clinical anatomists can illustrate to them gross anatomy of that particular region with the help of illustrations, models and dissected cadavers. This approach was tried and evaluated at the University of South Florida (USF) recently through verbal feedback and a questionnaire to the students of the last 8 years (5). Questions were asked of the students who were divided into two groups. The first group comprised of students who could see the deeper structures during operation while standing near the operation table while the second group comprised of student who could not see the deeper structures during the operation : (Table 1). Nintysix percent (96%) of students of the first group rated this method of great or moderate help while only seven percent (7%) claimed that it provided little or no help. Eighty-seven percent (87%) of the students of the second group rated it to be of moderate or great help while thirteen percent (13%) claimed little or no help from it. The USF students accepted this method of teaching anatomy because anatomy was taught to them in the early years of their medical course, yet they needed it in the final years or during post graduation. This time gap resulted in gaps in knowledge of gross anatomy. Practical anatomy (dissection on cadavers) has been replaced by theoretical anatomy in some of the institutions due to non-availability of unclaimed or donated bodies. Dissection of cadavers is said to be the most important and best method of learning gross anatomy throughout the world even today. Lack of individual attention to students during their academic session may be one of the causes of inadequate knowledge of gross anatomy. Hart and O'Shanick (1993) postulated that non-verbal memory storage is more stable than verbal memory storage over intervals of hours to days. Snodgrass and Mc Clure (1975) postulated that recognition memory seems to indicate that adult subjects in memory experiments will encode and store both pictorial and verbal codes to simple pictures where as they do not naturally doubly encode words alone. They consider two memory encoding to be better than one. It is proved that learning process of the students is enhanced by having visual confirmatory stimuli to assist the learning process in addition to verbal instructions by the teachers in the gross anatomy laboratory and the operating room. These advantages are highlighted (Table 2). Keeping in mind the effectiveness of the system of anatomy instruction developed by University of South Florida, this method can be introduced in the training of senior medical students and postgraduates of University Sains Malaysia on a trial basis, followed by evaluation. References
© Copyright 2006 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj06014t2.jpg] [mj06014t1.jpg] |
| |||||||||

{kind=link}
{kind=link}