 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 13, No. 2, July 2006, pp. 24-29 ORIGINAL ARTICLE SURVIVAL IN PATIENTS WITH NON-SMALL CELL LUNG CANCER WHO OPTED OUT OF CANCER-SPECIFIC THERAPY Li-Cher Loh, Ru-Yu Tan, Li-Yen Chan, Selvaratnam Govindaraju*, Kananathan Ratnavelu*, Shalini Kumar**, Sree Raman***, Pillai Vijayasingham***, Tamizi Thayaparan*** IMU Lung Research, International Medical University, Clinical School, Seremban; *Nilai Cancer
Institute, Nilai; **Department of Pathology, Seremban Hospital; ***Department of Medicine, Seremban
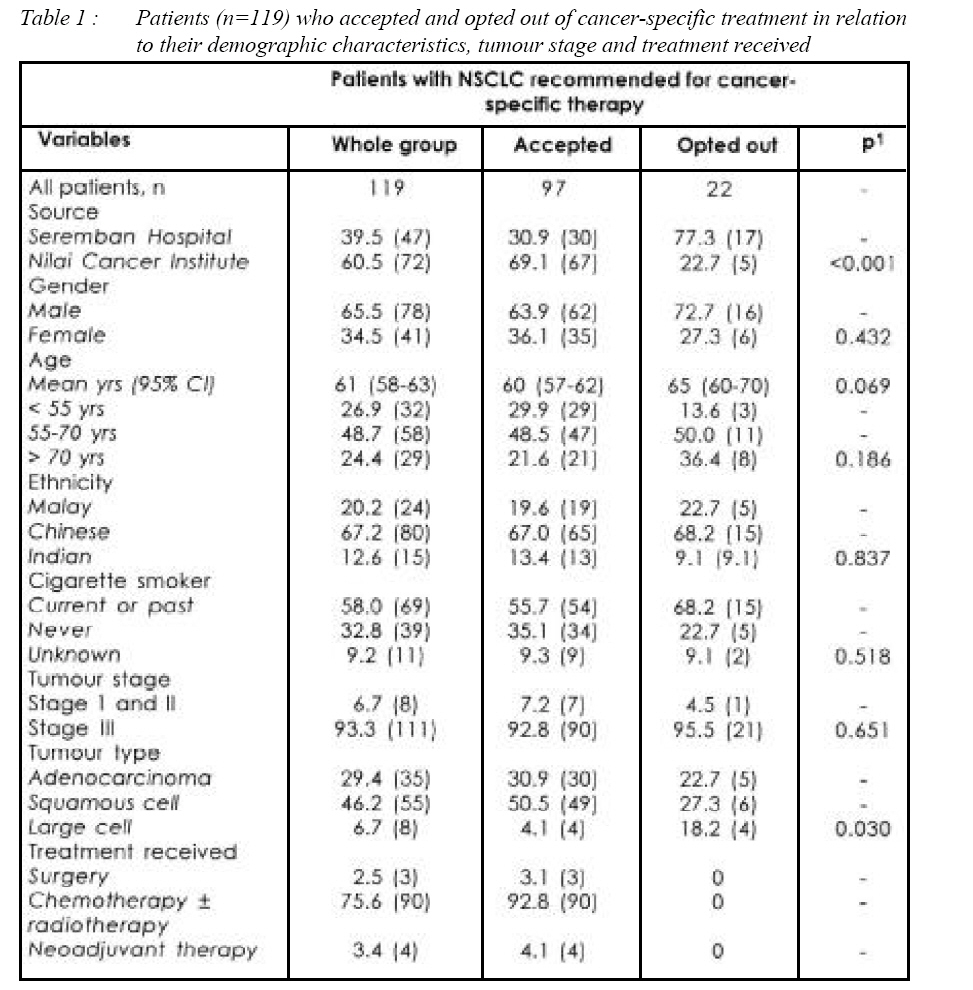
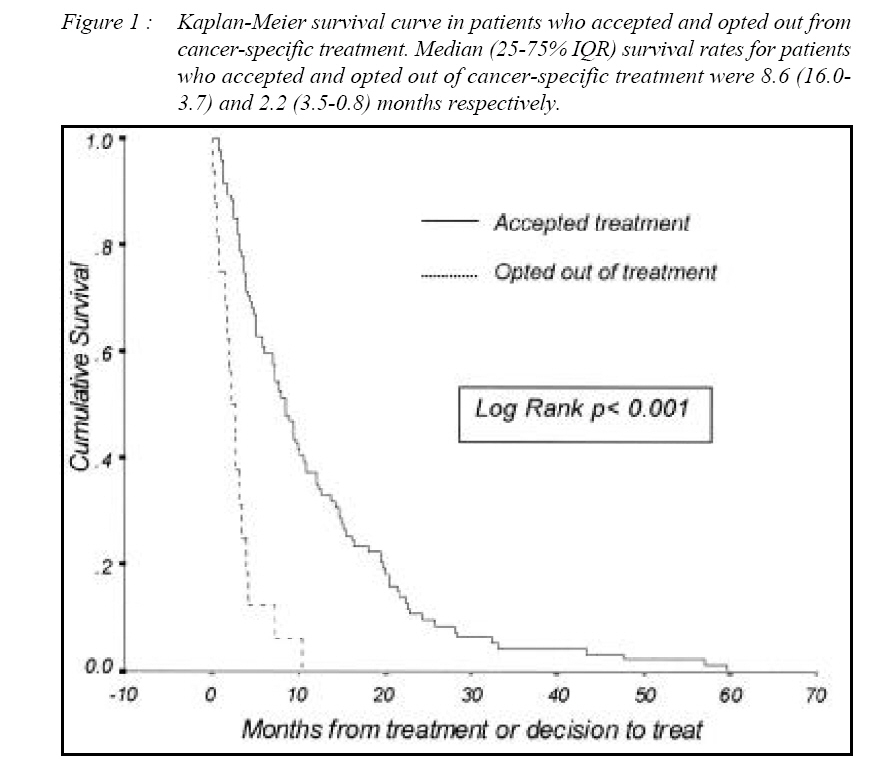
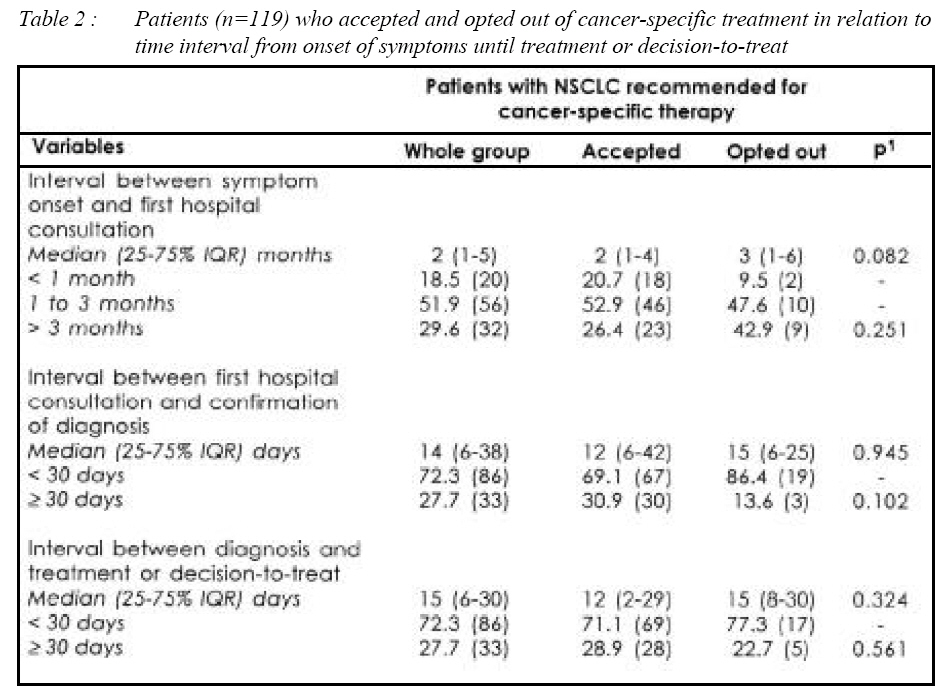
Hospital, Seremban, Malaysia Submitted-10.10.2004, Accepted-24.11.2005 Code Number: mj06019 In Malaysia, many patients opted out of cancer-specific treatment for various reasons. This study was undertaken to investigate the survival rate of patients with stages I to III non-small cell lung cancer (NSCLC) who opted out of treatment, compared with those who accepted treatment. Case records of 119 patients diagnosed with NSCLC between 1996 and 2003 in two urban-based hospitals were retrospectively examined. Survival status was ascertained from follow-up medical clinic records or telephone contact with patients or their next-of-kin. Median (25-75% IQR) survival rate for 79 patients who accepted and 22 patients who opted out of treatment, were 8.6 (16.0-3.7) and 2.2 (3.5-0.8) months respectively [log rank p< 0.001, Kaplan-Meier survival analysis]. Except for proportionately more patients with large cell carcinoma who declined treatment, there was no significant difference between the two groups in relation with age, gender, ethnicity, tumour stage, and time delays between symptom onset and treatment or decision-to-treat. We concluded that there was a small but significant survival benefit in accepting cancer-specific treatment. The findings imply that there is no effective alternative therapy to cancer-specific treatment in improving survival. However, overall prognosis for patients with NSCLC remains dismal. Key words : non-small cell lung cancer, survival, cancer-specific treatment, Malaysia Introduction The prognosis of lung cancer remains poor, with overall five-year survival figures varying between 5 and 10% worldwide (1). Unlike other solid tumours where survival rates have improved in the order of 60-90% with modern treatment, the management and prognosis of lung cancer has changed very little over the past 20 years (2). Malaysia produced its long-overdue first national cancer registry in 2003 and in its report, lung cancer is the commonest cancer in males and the fifth commonest in females (3). In view of this, there is merit in considering what may influence and be responsible for the poor prognosis of lung cancer in Malaysia. Doctors here frequently encounter patients who have decided to opt out of cancer-specific treatment, be it surgery, chemotherapy or radiotherapy, for various reasons. It is also recognized that many patients turn to alternative treatment, usually in the form of traditional medicine, although there is little data on their efficacy or survival benefit. In order to investigate the impact on survival in patients who specifically opted out of cancerspecific treatment, we compared the survival rates between patients with Stage 1 to III NSCLC who accepted and those who opted out of cancer-specific treatment in two urban-based hospitals (a state government general hospital and a private oncology hospital) in Malaysia. We also attempted to identify any patient clinico-demographic variables, including the time interval between onset of symptoms and treatment or decision-to-treat, which could possibly influence survival rates. Patients & Methods Data collectionUsing a structured data collection form, relevant information was retrospectively collected from the medical records of patients with confirmed NSCLC between 1 January 1996 and 1 April 2004 in Seremban General Hospital and Nilai Cancer Hospital. Patients, with their NSCLC histology types, were first identified from the pathology database of the Department of Pathology, Seremban Hospital and the Cancer Register, Nilai Cancer Institute. Their medical records were then retrieved for perusal. Data on tumour stage, date of onset of first symptoms as stated by the patient, date of first hospital consultation, date of diagnosis, date of treatment (or decision-to-treat if date of treatment was not available or not applicable), the type of treatment offered, and whether treatment was accepted or declined, were obtained from these patients' medical records. Patients whose records indicated that lung involvement was metastasis, and patients who opted out of treatment but died within two weeks from the date treatment was offered, were excluded from the study. The latter was intended to exclude patients who were probably better classified as Stage IV disease because of the rapid progression of disease. The protocol of the study was approved by the local university Research & Ethics Committee and carried out in accordance to the recommendations of the Helsinki Declaration of 1975. Tumour stageFor the purpose of data collection, tumour stage was categorized into those whose cancers were amenable to resection, those with unresectable, locally advanced cancers that were amenable to non-surgical cancer-specific therapy i.e. chemotherapy, radiotherapy or both, with the intention of prolonging life and those with terminal disease, where only palliative treatment was recommended. Broadly, they were consistent with Tumour Node Metastasis (TNM) Stage I to II, III and IV respectively. The reason for this approach was because many records in Seremban Hospital did not state the TNM classification. Only patients with Stage 1 to III disease were accepted into the study. Survival statusSurvival status was ascertained from records of follow-up visits in medical outpatient clinics, and if necessary, by direct contact with patients or next-of-kin by telephone. Patients whose survival status could not be confirmed were excluded from the study. Accepting vs. opting out of treatmentThis information was based on medical records and if necessary, verified by telephone contact with patients or their next-of-kin. Patients where this information could not be verified were excluded from the study. According to our study protocol, no attempt was made to elucidate the reason for opting out of treatment. This was due to the lack of such information from medical records and the possible sensitive nature of direct enquiry. Data analysisDescriptive analyses were used to characterize all patients. Differences between those who accepted and those who opted out of treatment were tested using Chi Square or unpaired t tests. The cumulative and median survival rate was measured using Kaplan-Meier survival analysis with log-rank test for the detection of difference in survival between the two groups of patients. The time at risk was accumulated from the date of treatment or decision-to-treat, until death or, in those alive, until 1 April 2004. Median delay (with 25% to 75% interquartiles, IQR) was calculated for each group, and Mann-Whitney test was used for pair way comparisons of delay. All computation was made using the statistical package SPSS version 11.5 for Windows (Chicago, Illinois, USA). In all cases, the significance was defined at the 5% level and twotailed. ResultsOf the 142 patients identified with the diagnosis of Stage 1 to III NSCLC, 21 patients were excluded due to incompleteness of data or missing medical records. Two were excluded due to death within two weeks from the date of treatment offer. The remaining 119 (83.8%) patients constituted the final analyzable sample for this study. Of these patients, 22 (18.4%) patients opted out of cancer-specific treatment (1 recommended for surgery; 21 for chemotherapy +/- radiotherapy). Most of them were from Seremban Hospital (77.3%), male (72.7%), of Chinese origin (68.2%), and were either current or past cigarette smokers (68.2%). Half of them were between 55 and 70 years of age. The majority of the tumour histological type was adenocarcinoma (46.2%). Significantly greater proportion of patients in Seremban Hospital opted out of treatment, compared with those in Nilai Cancer Institute (p<0.001). The histological types between the two groups were also significantly different in that there were proportionately more patients with large cell carcinoma in the group that opted out of treatment. Otherwise, there were no significant differences in the patient demographic characteristics and tumour stage between the two groups (Table 1). Mean age of patients who opted out of treatment was higher than those who accepted (65 vs. 60 yrs). This was, however, not statistically significant (p=0.069). Median (25-75% IQR) survival rates for patients who accepted and those who opted out of cancer-specific treatment were 8.6 (16.0-3.7) and 2.2 (3.5-0.8) months, respectively. The difference was statistically significant (log rank test p<0.001) (Figure 1). In patients who opted out of cancer-specific treatment, the median (25- 75% IQR) time interval between onset of first symptoms and first hospital consultation, between first hospital consultation and confirmation of diagnosis, and between diagnosis and treatment or decision-to-treat, were 3 (1-6) months, 15 (6-25) days, 15 (8-30) days, respectively (Table 2). These time intervals were not significantly different from those who accepted cancer-specific treatment. DiscussionWe have shown that there was a clear survival benefit for patients who accepted cancer-specific treatment. Except for tumour histology, we could not identify any association with the patients' demographic characteristics, tumour stage, and time intervals from onset of symptoms to treatment or decision-to-treat, between patients who accepted and who opted out of treatment. Although our study showed what is already intuitively known, i.e. cancer-specific treatment conveys survival benefit, albeit small especially when complete resection of tumour is not possible (1), the purpose of our study was also to examine the category of patients who specifically opted out of modern-day cancer-specific treatment in the Malaysian setting. As far as possible, this information was verified during follow-up visits or during telephone contact with patients or their next-of-kin. Unfortunately, the retrospective nature of the study and the possible sensitive aspect of direct enquiries prevented our study from probing into the reasons for the decline. It is widely known that patients decline cancer-specific treatment for various reasons. Studies addressing reasons for this are sparse, perhaps due to the complexity in studies of such nature. A study in Russia, published in 1980 by Efimov et al (4), looked at the reasons in 180 patients who refused surgical treatment for lung cancer. They showed that 45% of patients declined treatment for fear of surgery, or due to unawareness of its potential benefit, or opted for home remedies instead. Another 35% did not believe in the cure offered by surgery. It is very possible that these same reasons are still relevant today in Malaysia and worldwide. The psychosocial impact of lung cancer on patients and their families is well recognized and has been extensively studied (5 - 7). Patients with lung cancer experience stigmatization, blame and shame (5), and frequently manifest psychiatric symptoms such as insomnia, poor concentration and disinterest (6). Family members including spouses also play an important role, and it has been shown that they tend to view patients' functioning more negatively than the patients themselves (7). These socio-psychological factors play an important role in the patients' decision making of whether to accept or decline treatment. Seeking home remedies (4) or traditional treatment as a cause for opting out of treatment may be of particular relevance in Malaysia. Doctors often encounter patients who prefer alternative treatment, usually in the form of traditional medicine. One reason for this may be the fear of the toxicity of chemotherapy or radiotherapy, as experienced by other cancer patients. Another reason may also be cultural, reflecting a highly established tradition of medical pluralism in Malaysia where doctors, sinsehs and bomohs are readily available (8 - 10). Patients move freely between the modern and traditional medicinal system, or use both systems simultaneously (9). Confidence in traditional medicine has resulted in patients of self-discharging themselves from hospital against medical advice (11) or not complying to treatment (12). While there is emerging evidence that many traditional herbal medicines contain anti-cancer properties (13, 14), our data implies that used alone (15), there is no effective alternative therapy when compared to modern-day cancer-specific treatment. We do not think that financial consideration was an important cause for declining treatment in our study, since the majority of patients who opted out of treatment were from Seremban Hospital where treatment is available at low cost due to government subsidy. Finally, it is possible that religious sentiment might play a role in the patients' decision as most religions here consider death as the will of God. With the exception of tumour histology, we did not identify any factors that differentiated between those who accepted and those who declined treatment. The reason for proportionately more patients with large cell carcinoma opting out of treatment is unclear. The small number of patients with large cell carcinoma in both groups (4 vs. 4) suggests that the statistical significance found is likely to be coincidental. The trend towards more older patients being in the group that opted out of treatment suggests the possibility of age affecting the decision whether to accept specific treatment. Being retrospective in nature, our study seeks to reduce bias by excluding nearly 20% of the initial patient sample, in whom information were incomplete. Nevertheless, inaccuracies of doctors' records and patients' recall could still introduce bias in the study. Nevertheless, we have no reason to believe that any misclassification in this respect would significantly affect our findings. While there have been several studies on lung cancer in Malaysia (16 - 18), none, except for one on surgically treated patients (19) has looked into the question of survival. Our study provides survival data in patients with Stage I to III NSCLC, with and without cancer-specific treatment, in the Malaysian setting. This is timely in view of the recently released National Cancer Registry (3). The overall prognosis of NSCLC remains dismal, with the median survival rate for patients (primarily Stage III) amenable to cancer-specific treatment (primarily non-surgery) is 8.6 months. Our findings show that there is a small survival benefit of several months in persuading patients to accept cancer-specific treatment. It is unclear however whether this longer survival is associated with improved quality of life. More research is required to address this, and also to study the reasons for patients to opt out of modern-day cancer-specific treatment. It is possible that many of the reasons for declining treatment are unjustifiable and irrational, and appropriate intervention, perhaps in terms of support and counseling, can prevent this (20-21). AcknowledgementsThe authors wish to thank the support of Hospital Directors, Seremban Hospital and Nilai Cancer Institute for this research, and the permission of the Director-General, Ministry of Health Malaysia to publish the data from Seremban Hospital. The research is supported by an internal research grant from the International Medical University. References
© Copyright 2006 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj06019t2.jpg] [mj06019f1.jpg] [mj06019t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}