 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 13, No. 2, July 2006, pp. 45-51 ORIGINAL ARTICLE RATIONAL MANAGEMENT OF DIFFERENTIATED THYROID CANCER Birendra Kishore Das*, Biswa Mohan Biswal, Venkata Murali Krishna Bhavaraju Department
of
Nuclear
Medicine,
Radiotherapy
and
Oncology
School
of
Medical
Sciences,
Universiti
Sains
Malaysia
16150
Kubang
Kerian,
Kelantan,
Malaysia Submitted-10.10.2004, Accepted-24.11.2005 Code Number: mj06022 Differentiated thyroid cancer ( DTC ) is usually not very common ( incidence is about 1 % of all cancers and women are more often affected than men ). However, higher incidences has been reported in many parts of South East Asia particularly in iodine deficient areas. Unlike other solid tumors , DTC is potentially curable with documented survival rate of > 90 %. Even if the disease is not totally cured, through repeated high dose radio iodine therapy the progress of the disease can be controlled with significant improvement in quality of life for many years. This is possible if a proper and state of the art therapeutic approach is made. Since the incidence is relatively low, individual experience of treating physicians or centers is mostly inadequate leading to improper management with subsequent increase in morbidity and mortality. The purpose of this review is to evolve a rational management protocol for the treatment of thyroid cancer. Centers which do not have all facilities like high dose radio iodine therapy etc. may still follow the protocol by referring the patient for a particular step to another centre. What is needed is the awareness of the treating physician about the appropriate management of DTC. In recent years, there have been some important developments in the management of differentiated thyroid cancer like use of recombinant human thyrotropin (rhTSH), use of retinoic acid for redifferentiation etc. Some of these developments having practical relevance have been briefly mentioned. Key words : Thyroid cancer management, Differentiated thyroid cancer, Radioiodine therapy in thyroid cancer Introduction Malignancy of the thyroid gland is rare and in general makes up about 1% of all cancers (1). However, in endemic goiter regions the incidence of thyroid cancer is relatively high. It is suggested that long term stimulation of thyroid tissue proliferation in iodine deficient areas is one of the causes for this increased incidence (2). Iodised salt prophylaxis in iodine deficient regions has resulted in decline of endemic goiter and goiter associated diseases. Interestingly, a significant change in the histological pattern of thyroid malignancy has been observed after introduction of iodised salt prophylaxis (3). For example, long term systematic data analysis in Switzerland has shown that the percentage of undifferentiated thyroid carcinoma has declined from almost 39 % before introduction of iodised salt to about 24 % thereafter. Similarly, there is decline of follicular thyroid cancer from about 42 % to almost 28 % while papillary thyroid cancer shows increase to 23 % from 8 %. This indicates that iodised salt prophylaxis has not only decreased the overall incidence of endemic goiter, but also shifted the more aggressive form of thyroid cancer to a less aggressive form. The most outstanding feature of most thyroid malignancy is that complete cure and / or long term remission is possible even in stage IV provided appropriate and adequate treatment is made available. The reason being that the differentiated thyroid ca including metastases, retains its property of concentrating iodine and therefore enabling radio iodine therapy to delivery a very high radiation dose capable of completely eliminating the malignant tissues. Classification of Thyroid tumors :Malignant tumors of the thyroid gland can be divided broadly into three groups: Carcinomas, sarcomas and others including metastasis from extra thyroidal malignancies. Thyroid carcinomas which form the majority of thyroid malignant tumors, appear in two forms: differentiated and undifferentiated. The differentiated thyroid carcinoma develops from thyrocytes and include papillary, follicular and mixed varieties. The medullary (C-Cell) thyroid carcinoma which originates not from the thyrocytes but from calcitonin producing para-follicular cells belongs to this form of differentiated thyroid ca. The undifferentiated thyroid carcinoma (also known as anaplastic ca) occurs in the form of small cells, polymorph cells, spindle cells and rarely squamous cells. The sarcomas include fibrosarcoma and many other types of sarcomas. A variety of other malignancies, though very rare, are also found in the thyroid. They include carcino-sarcoma, malignant hemangioendothelioma, malignant lymphoma and malignant teratoma. The thyroid gland may also be the site of metastasis from bronchial, colorectal, renal and other cancers (4). As already stated above, the most common malignancy of the thyroid gland is the differentiated thyroid cancer. The follicular thyroid cancer causes early hematogenic metastasis in the lungs and bone whereas the papillary ca spreads by lymphatic system to regional neck lymph nodes. A special form of follicular cancer is the oncocytic (also known as Hurthle – cell) carcinoma. The typical feature of this variety is that it does not concentrate radioiodine, but produces thyroglobulin so that estimation of thyroglobulin and not whole body scan will form the basis of follow up. The prognosis of this variety is relatively poor (survival rate 50 to 60 %). Diagnostic modalities :The fact that appropriate treatment of the commonest form of thyroid cancer can lead to long-term survival and cure, makes it prudent to conduct proper investigation of each case of suspected malignancy. The simplest method which is absolutely non-invasive, is to go for a sonogaphy or scintigraphy. Reduced ecogenicity in ultrasound with irregular border and signs of infiltration are highly suspicious of malignancy. With thyroid scintigraphy, it is very easy to distinguish a hot nodule from a cold nodule. The former practically rules out malignancy whereas the later warrants further investigations like fine needle aspiration cytology (FNAC). All suspicious nodules of more than 1.5 cm size need FNAC unless they are ‘hot'. About 10% of so called ‘cold nodules' are found to be malignant (5). This differentiation is necessary not only to proceed with appropriate therapy but also to avoid unnecessary surgery in 90% of cases which are found to be benign (6). TNM staging of thyroid tumors :The pre-therapeutic clinical staging is important. However there are a number of different staging / classification systems like AGES, AMES, FORTC, DAMES etc. mainly from a prognostic point of view. For management, the TNM classification has been used widely and may be made as follows : T0 -not palpable Based on long term experience and critical analysis, there is by and large worldwide consensus about therapeutic modalities (7,8). Near total thyroidectomy followed by high dose radioiodine therapy forms the basis of treatment. The objective is elimination of all thyroid tissue (total ablation) from the body. Although this basic concept of treatment has been standardised the following points of controversy remain :
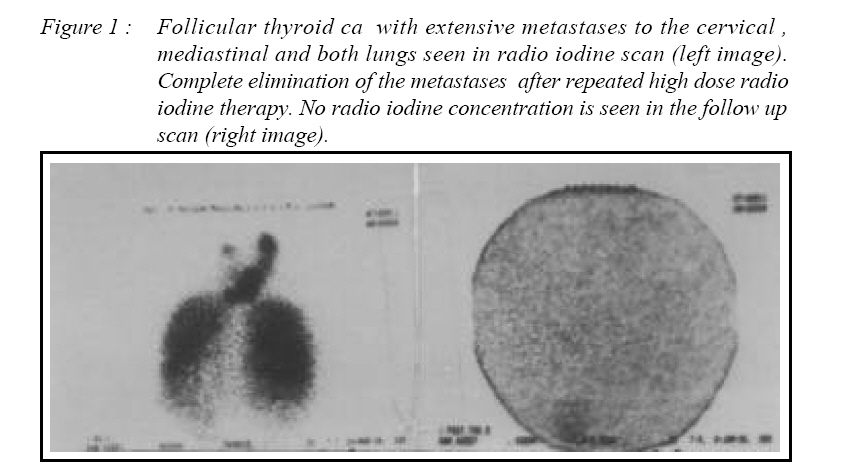
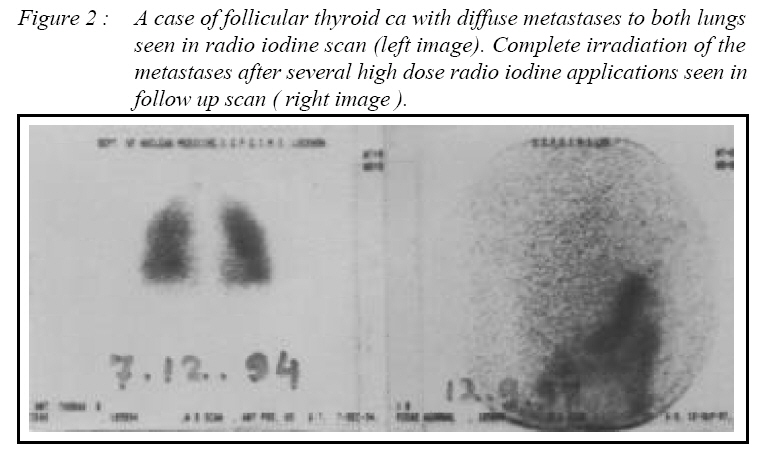
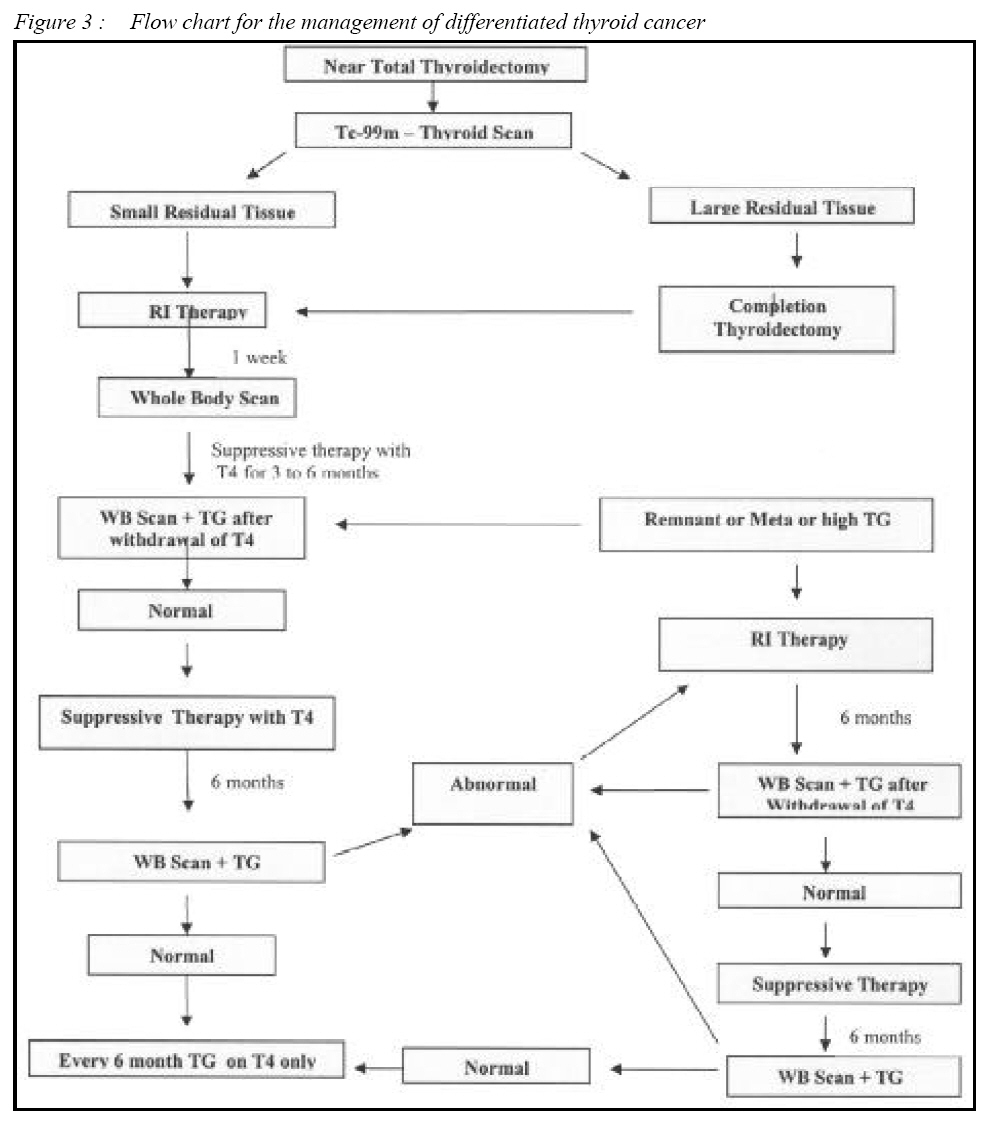
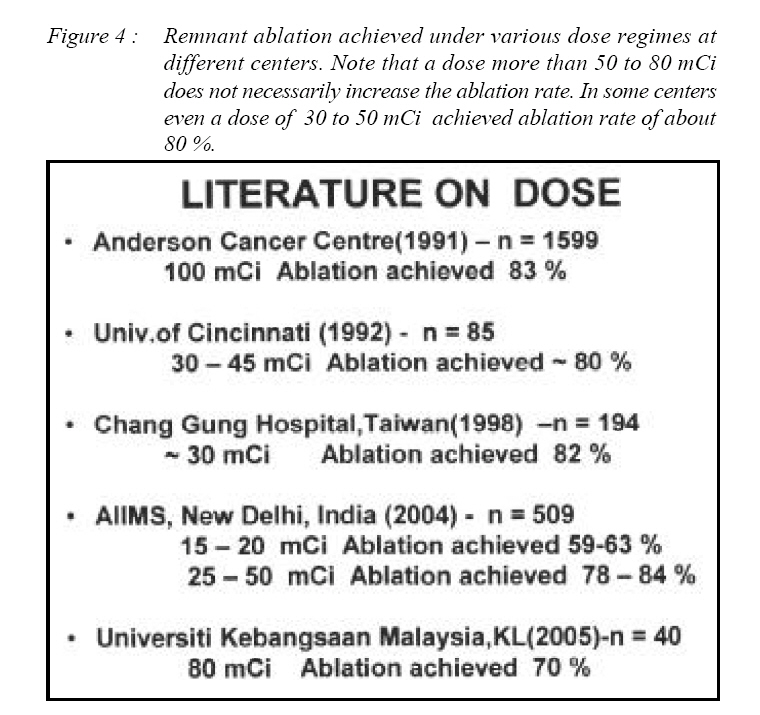
Radio iodine ( I-131 ) was first introduced in the early 1940s as an oncologic therapeutic agent. After more than fifty years, I-131 has become the agent of choice and is now available in many centers. Some physicians, however, feel that young patients with well differentiated solitary tumors have excellent prognosis and therefore may not need I-131 treatment. Other groups have however shown lower rates of recurrence and prolonged survival rates for patients treated with I-131 compared to those who did not receive radio iodine therapy (9,10). Although, these tumors usually appear as cold areas on the thyroid scan, nearly 80% concentrate significant amount of radioiodine if serum TSH is elevated (more than 30 uIU/ ml).The beta rays ,the major component of radiation emitted by I-131, deliver a very high absorbed dose (60,000 to 100,000 rads) effecting total kill of the tissue. Destruction of the remnant thyroid tissue after surgery with radioiodine thus decreases the risk of recurrence and death from well differentiated thyroid cancer. A whole body scan with I-131 prior to therapy can detect residual tissue or metastases which can then be treated with high doses of I-131. Cervical lymph node metastases are usually destroyed and at least half of lung metastasis are completely eliminated. Fig 1 shows a case of follicular thyroid ca with metastases to cervical-mediastinal lymph nodes and both lungs successfully treated by radio iodine therapy. Fig 2 shows another case of follicular ca with diffuse metastasis of the lungs and total cure after multiple radio iodine therapy. However, in some patients with persistent invasive thyroid cancer with distant metastases, the role of I-131 is palliative. Life can be prolonged and symptoms relieved in a large percentage of patients although patients with extensive bone and lung metastasis, eventually succumb to the disease (11). Post operative radioiodine therapy also provides the following advantages during follow up period where it enables easy and better detection in case of recurrence. It allows interpretation of Thyroglobulin (TG) levels during follow up period and it enables detection of very small metastases using follow up radio iodine whole body scans. Complications of Radio iodine therapyRadiation thyroiditis may occur, 1-8 days after therapy and consist of transient pain and tenderness in the neck region. Discomfort or pain on swallowing is frequent and may radiate up to the ears or down into the chest. There may be slight swelling of the region over the remnant tissue and rarely the swelling may be severe enough to cause partial airway obstruction. Radiation thyroiditis may be associated with transient elevation of thyroid hormones due to rapid release of iodinated protein. Severe pain on swallowing and transient hyperthyroidism are extremely rare and appear to occur when intact thyroid glands or whole lobes are ablated. The mild pain can be treated with salicylates but severe pain requires steroids (30 mg daily tapered rapidly over 7 days) while transient hyperthyroidism if present is treated with propanolol (40 mg twice daily). Long term follow upSuccessful elimination of all cancer tissue from the body is to be confirmed by two consecutive negative whole body scans. Suppressive therapy is to be started as early as possible and must be continued life long. It should be adequate (usually 150 to 300 ugm of thyroxine, preferably to be taken on an empty stomach). It is important to explain to the patient about the relevance and need of the substitution therapy to ensure compliance. Optimal suppressive therapy has to be documented by occasional estimation of TSH which should be below 0.01 in young adult patients and below 0.5 in elderly patients. Long term follow up at various time intervals (6 months to 12 months depending upon the individual case) is mandatory. Estimation of thyroglobulin along with thyroglobilin antibodies during the follow up period has been found to be very useful in detecting eventual recurrence. The general therapy concept for treatment of differentiated thyroid cancer does not vary much from one centre to the other. The basic therapy plan (Figure 3) followed by us has been found useful and can be recommended . Medullary thyroid caeinomaIn case of Medullary thyroid ca (C-cell Ca), intensive surgery including removal of cervical and if needed mediastinal lymph nodes is necessary. Therapy with 131-I-MIBG has been introduced recently and the results are quite encouraging. Regular estimation of calcitonin level during follow up has proven to be a very sensitive parameter for detection of recurrence. Recent advancesIn recent years, some new developments have taken place which may be considered for incorporation in the routine management. Withdrawal of thyroxine for a prolonged period to achieve endogen stimulation before diagnostic WB scan or ablation therapy may cause in some patients sever problems associated with hypothyroidism. With the administration of recombinant human thyrotropin (rhTSH) (i.m. injections of 0.9 mg of rhTSH on two consecutive days) sufficient stimulation is achieved to perform the diagnostic WB scan or administrating ablation therapy, thus avoiding hypothyroid state (13,14). It has also been found that rhTSH-stimulated serum Tg level gives more reliable information about the existence or recurrence of malignant tissue than diagnostic WB scan after T4 withdrawal.(15,16). The sufficient stimulation even after two weeks of T4 withdrawal has been seen in serial estimations of TSH following withdrawal of thyroxine. Many authors have shown that a sufficiently high basal TSH level (> 30 uIU/ml) is achieved even after 15 days so that effective radio iodine therapy can be given after this period. It is not necessary that all patients wait till 4 weeks after T4 withdrawal, thus reducing morbidity which can be very severe in some patients (17, 18). Differentiated thyroid cancer even with extensive metastases can be well managed. However it has been observed that up to one third of such malignancies become de-differentiated during years of follow up (19) and loose the property of concentrating iodine and hence not amenable to radio iodine therapy. Other options of therapy are limited and generally not effective. Recent studies have shown that retinoic acid (RA) can cause re-differentiation in about 40 % of such patients and lead to tumor regression after radio iodine therapy (20). RA is administered at a dose of 1.0 to 1.5 mg/kg/day for 5 weeks before radio iodine therapy. It can re-induce radio iodine uptake by the tumor and thus render them suitable for further radio iodine therapy (21). The use of lower dose for ablation therapy is discussed in a number of recent publications advocating lower radio iodine dose for initial ablation therapy. It appears that a dose beyond 50 to 80 mCi does not increase the rate of initial ablation. (Figure 4) shows some of the data on dose response to ablation (22-26). ConclusionsDifferentiated thyroid carcinoma, if treated adequately, has excellent prognosis. After near total thyroidectomy, adjuvant therapy with radioiodine is indicated in all cases having remnant tissue with the objective of eliminating all thyroid tissue from the body. Radioiodine should also be used in cases of extensive metastasis to achieve long term palliation and improvement of quality of life. Regular follow up is necessary to ensure compliance of substitution therapy as well as to take timely decision if repeat of radioiodine therapy becomes necessary. If two consecutive low dose radioiodine whole body scans done at 6 months interval are negative for remnant tissue or metastasis, it is sufficient to do follow up by thyroglobuline (TG) alone. References :
© Copyright 2006 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj06022f2.jpg] [mj06022f4.jpg] [mj06022f1.jpg] [mj06022f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}