 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 13, No. 2, July 2006, pp. 52-60 ORIGINAL ARTICLE IS GRANDMULTIPARITY A SIGNIFICANT RISK FACTOR IN THIS NEW MILLENNIUM? Noraihan Mohd. Nordin*, Choong Khim Fen*, Suhaimi Isa**, Edwin Malcolm Symonds* *Obstetrics
and
Gynecology
Division,
Department
of
Human
Growth
and
Development,
Faculty
of
Medicine
and
Health
Sciences,
University
Putra
Malaysia,
Kuala
Lumpur,
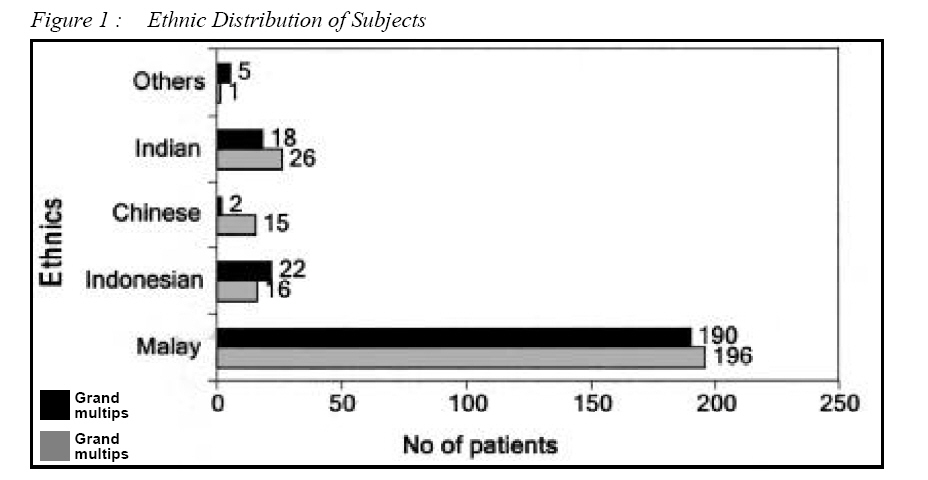
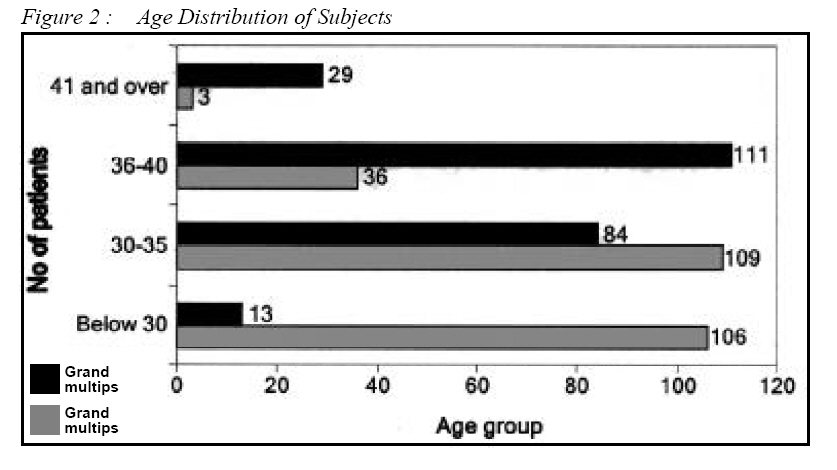
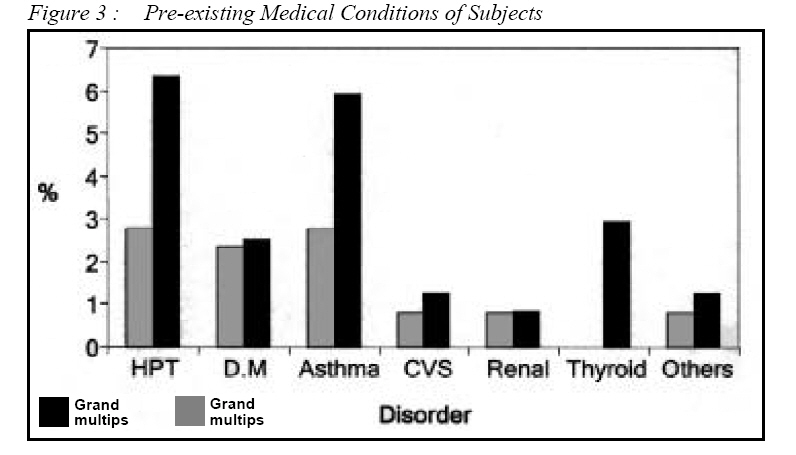
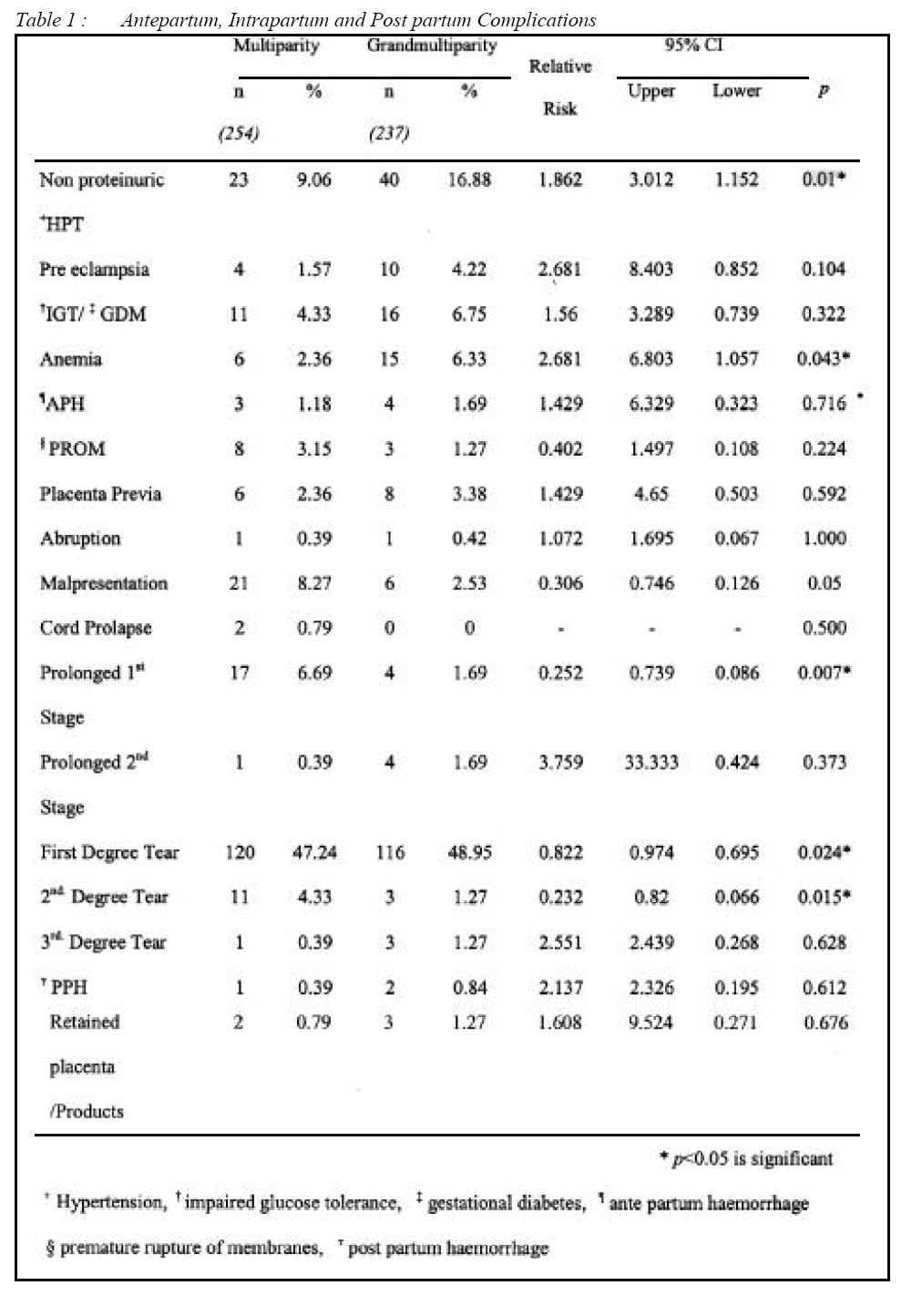
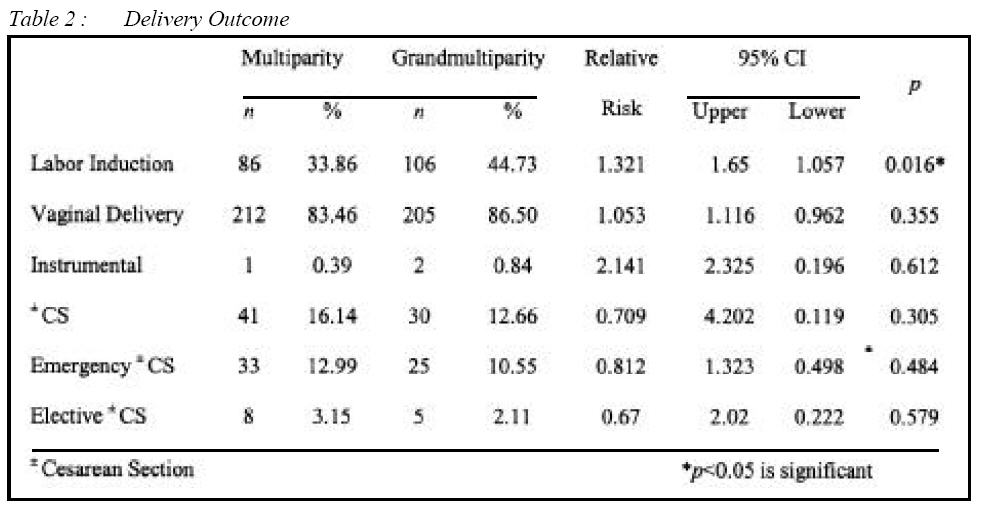
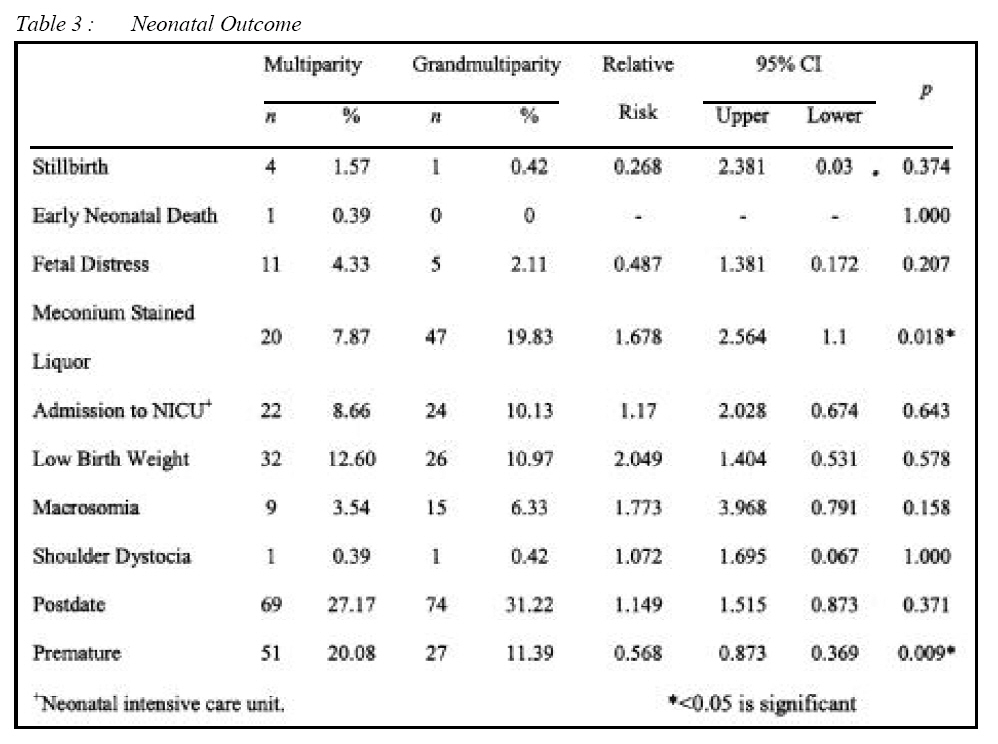
Malaysia. Submitted-10.10.2004, Accepted-24.11.2005 Code Number: mj06023 The aim of the study was to assess the outcomes of grandmultiparous women receiving the current obstetric care in Maternity Hospital Kuala Lumpur. Recent data regarding some of the complications are conflicting and the significance of grandmultiparity is now in question. Therefore, a retrospective cohort study of 237 grandmultiparous and 254 multiparous women were undertaken. Chi-squared and t test were used (P<0.05) where appropriate. The results revealed that grandmultiparous women tend to be Malays, age above 35, have late antenatal booking and suffered from anemia and non-proteinuric hypertension. There was no significant difference in diabetes and glucose intolerance, ante partum and post partum hemorrhage. There was a significantly lower risk of first and second-degree perineal tear, and prolonged first stage of labor. There was a significant increased in induction of labor but there was no uterine rupture and no increased in Cesarean Section. There was an increased in meconium stain liquor but there was no increased risk of fetal distress. The fetal outcome was good and there was no tendency to macrosomic infants or shoulder dystocia. With adequate care, the maternal fetal outcome of grandmutiparous women is good and comparable to the multiparous women. Anemia is still common and patient education is important to overcome this problem. Key words : Grandmultiparity, maternal fetal outcome, Malaysia Introduction Grand multiparity, dubbed the dangerous multipara by Solomon et al. (1934) (1), has been shown to be associated with a variety of complications such as anemia, hypertension, unstable lie, malpresentation, late engagement of fetal head, rapid labors, macrosomia, preterm labor, uterine rupture and post partum hemorrhage (PPH). PPH is usually precipitated by uterine atony and Ijaya et al. (2003) (2) found the increase by two folds compared to lower parity. This life threatening complication compounded with anemia made grandmultiparity a significant risk factor, as it can lead to maternal death (3). However, even though PPH is increased, (4-8) surprisingly there werestudies that reported no increased in incidence (9-11). In addition, there were also conflicting data on the risk of anemia. There were studies that showed an increased incidence (4,12-14), and a study that showed no difference (15) and there were even studies that showed a reduced incidence (8). Moreover, malpresentation was another complication reported where Babinszky et al. (1999) and Ozumba and Igwegbe (1992) showed that there was an increased incidence (5,13) but there were reports that showed there was no difference (9,16,17). Furthermore, there were reports of an increased in macrosomic babies (5,8-10) but Ozumba and Igwegbe (1992) showed no difference (13). Hypertension was increased (8,10,13,14) however, there were reports of no increased incidence (4,9). In addition, Abu-Heija and Chalabi Hel (1997) showed an increased incidence of pre eclampsia (16) while Toohey et al. (1995) found no significant difference (17). Recent data regarding some of the above complications are conflicting and the significance of grandmultiparity is now in question (16,17).These conflicting data probably reflects the wide range of factors that may not be related to parity but is a consequence of other variables. For example, macrosomia is associated with maternal weight, genetics and ethnicity. Hypertension is associated with age and grandmultips tend to be older women. The availability of oxytocics, and blood bank facilities and active management of third stage may make PPH less prevalent in these grandmultips. Moreover, there is a tendency towards smaller families as women are more educated and career orientated where the availability of contraception makes grandmultiparity less prevalent. In Malaysia, grandmultiparity is still common and this is probably due to various factors. The government of Malaysia is encouraging women to increase their family size in line with the policy to increase the population of Malaysia. Religious and cultural beliefs also play a role. However, grandmultiparity is associated with PPH, which is the leading cause of maternal death in Malaysia (3). Thirty to 40% of PPH related mortality in Malaysia occurred in patients with parity of more than five. Therefore, grandmultiparity may still be a significant risk factor in this country (3). However, with the improvement of maternal child health services and socioeconomic status, the complications of yesteryear may not be reflected in today's modern obstetrics management of the grandmultiparous woman. Therefore, a current baseline data based on the local population is helpful to ascertain the prevalence and maternal and fetal outcome of the grandmultipara, which are the objectives of this study. This can throw some light into the complications of the local population receiving the current obstetric care. MethodologyThis study was conducted in Kuala Lumpur Maternity Hospital (MHKL). A total of 716,681 deliveries had been conducted in this hospital from 1963 to 1999, making MHKL one of the largest and busiest maternity hospital in Malaysia with around 24,000 deliveries yearly (18). It also serves as a referral center for numerous government antenatal clinics, private hospital and also private clinics around Klang Valley. This was a retrospective cohort study conducted within a 3 months period between 1st of January 2000 to 31st of March 2000, in which a total of 3657 deliveries were carried out. Out of 3657 deliveries, 329 were grandmultips and this information was identified from the database of the records department of the hospital. The definition of grandmultiparity varied from parity of four, to five and six in various studies (4,8, 9,13). In this study population, grandmultiparity is defined as a woman who has already had five or more deliveries or fetuses of at least 28 weeks maturity. The cut-off point of 28 weeks was taken. The reason is the viability at this gestation is more than 75% but before 28 weeks the survival rate is poor and drops markedly to 50% (18). Abortions, vesicular moles and ectopic pregnancies were excluded. A total of 251 records were retrieved from the Records Department of the Hospital (retrievable rate of 76.29%). A total of 237 records were selected and reviewed as cohort group. The selected group was adjusted for confounding variables and non-booked cases, drug abuse and smoking were excluded. The control group comprising of parity 2 and 3 was selected randomly through SPSS random number task and were adjusted for the same confounding factors. Hence, a total of 254 records was selected and reviewed as control group. This study was also more selective in its control, as only parity 2 and 3 were included as control; parity 4 was excluded as it lies between grandmultiparity and multiparity. As there is no general definition of grandmultiparity, by selecting parity 2 and 3 as control, the control group is better defined. The obstetrics outcomes of these two groups were reviewed and compared. The definitions of the terms used are as follows. Gestational diabetes (GDM) is defined as carbohydrate intolerance resulting in hyperglycemia with onset or first recognition during pregnancy and diagnosed based on the 75 gm OGTT by WHO criteria (19). Impaired glucose intolerance (IGT) is diagnosed based on WHO criteria (19). The patients with hypertensive disorders in pregnancy in this study are divided into three groups i.e. pre-existing hypertension (HPT), non proteinuric HPT and pre-eclampsia (PE). Hypertension in pregnancy (HIP) is defined as a maternal diastolic blood pressure >90 mmHg (12.0 kPa) for two consecutive readings taken 4 hours or more apart or, one diastolic reading blood pressure was equal to or greater than 110 mmHg (14.7 kPa). PE is the development of hypertension and significant proteinuria after 20 weeks of gestation (20). Significant proteinuria is the presence of proteinuria of 0.3 gm/L over 24 hours or the presence of at least plus proteinuria on the dipstick. Anemia is defined as the hemoglobin level during pregnancy of less than 10.0 gm/dl (3). Premature rupture of membranes is the spontaneous rupture of membranes before spontaneous labor (20). Preterm labor is onset of labor before 36 completed weeks (20). Antepartum hemorrhage is bleeding per vaginally after fetal viability (20). Placenta previa is placenta implanted on the lower uterine segment (20) and confirmed by ultrasound. Abruption is hemorrhage resulting from the premature separation of placenta (20)and diagnosed clinically. Post-date is a pregnancy, which is more than 42 weeks calculated from the last normal menstrual period or from early ultrasound scan before 20 weeks (20). It includes all patients admitted for elective delivery for the indication of postdatism. Labor induction includes the use of syntocinon, prostaglandin and artificial rupture of membranes. The normal first stage is defined as labor starting from the onset of labor to full cervical dilatation (20). Prolonged first stage and second stage is defined as those recorded in the hospital case notes. The definition of PPH is bleeding per vaginally of more than 500 mls within 24 hours of delivery (20). Fetal macrosomia is defined as birth weight equal or greater than 4.500 kg (20). Low birth weight is defined as birth weight less than 2.5 kg (20). Perinatal mortality included fresh stillbirth and macerated stillbirth and early first week neonatal death (20). Statistical analysisThe maternal obstetrics outcomes and perinatal outcomes of grandmultiparity and controlled group were analyzed using the Statistical Package for Social Sciences program, SPSS 10.1 computer software. Relative risk was determined using risk estimation of SPSS 10.1 along with 95% confidence interval. Chi squared, Fisher Exact Probability Test and Students t test were performed where appropriate. P < 0.05 is considered to be of statistical significance. ResultsThere were a total of 3657 deliveries and there were 329 grandmutiparous women, which made the prevalence, nine percent. Out of 329 grandmultips, 251 case notes were retrieved. The non-retrievable records were due to loss, misplacement or unavailability during data collection. After adjusting for the potential confounding factors, a total of 237 grandmultips were selected and the case notes were reviewed. Two hundred and fifty four multiparous women served as controls and were compared with the grandmultiparous women. Most of the samples were Malaysians (83.46% multips and 89.45% grandmultips) even though Kuala Lumpur Maternity Hospital also receives foreign patients (Indonesians comprise 6.30% of multiparous patients and 9.28% of grandmultiparous patients). The majority of grandmultips were Malays (80.17%) and Chinese made up less than 1% (p <0.005). Most of the grandmultips were above 35 years old (59%) whereas most of the multips were below 35 years (84%, p <0.05), (Figure 1 & 2). Half of the grandmultiparous patients were booked at Kuala Lumpur Maternity Hospital (50.21%) and most of the multiparous patients were booked at peripheral community-based government clinics (53.15%). The grandmultips booked significantly later (mean=24.21 weeks) than the multips (mean=21.42 weeks; p <0.001). Pre-existing medical disorders e.g. hypertension and diabetes mellitus were not significantly different from the multips (p <0.05) except for a significantly higher proportion (p <0.05) of thyroid disease (Figure 3). Table 1 shows the antepartum complications found in the grandmultips compared to the multips. Non-proteinuric hypertension and anemia were significantly higher compared to the control group (p <0.05). However, although pre-eclampsia, gestational diabetes and impaired glucose tolerance were more frequent, they were not statistically significant (Table 1). There was no difference in antepartum hemorrhage, placenta previa, placental abruption and prelabour rupture of membranes between the two groups. Surprisingly, there was a lower number of malpresentation and the proportion was approaching statistical significance (p =0.05). Anemia was significantly higher with a relative risk of 2.618 (95% CI: 6.803; 1.057; p =0.043). In the intrapartum period, there were no patients with ruptured uterus or precipitate labor. In addition, there was a lower risk of prolonged first stage (Table 1). The mean first stage of labor duration was significantly shorter in the grandmultips (mean=3.03 hours) as compared to the multips (mean=4.54 hours; p <0.001). There was however, no difference in prolonged second stage of labour or in the mean second stage duration (multips, mean=16.31 minutes; grandmultips, mean=15.96 minutes, p =0.368). There was no significant difference in the mean blood loss in labor (p =0.368) and postpartum hemorrhage between the two groups (Table 1). There was also no significant difference in third degree tears, and retained placenta (Table 1). Grandmultips had a significantly higher intact perineum (44.73% in grandmultips vs 27.17% in multips; p=0.003) and they required fewer episiotomies (3.38% in grandmultips vs 23.23% in multips; p <0.05). They also had a lower risk of first-degree and second-degree perineal tears (Table 1). Grandmultips had a statistically higher risk of intervention as labor induction was increased with a relative risk of 1.321 (95% CI: 1.65; 1.057, p =0.014). However, there were no significant differences in the vaginal delivery, Cesarean section and instrumental deliveries between the two groups (Table 2). Grandmultips had a higher risk of meconium-stained liquor (RR=1.678, 95% CI: 2.564; p =1.404), but there was no significant difference in postdatism between the two groups. In addition, there was no significant difference in fetal distress and admission to the neonatal intensive care (Table 3). There was also no significant difference in babies with macrosomia, shoulder dystocia or low birth weight (Table 3). Even though the grandmultips were at a significantly lower risk of preterm deliveries, there was however no significant difference in the mean birth weight (multip, 3.19 kg; grandmultip, 3.16 kg; p=0.821) (Table 3). There were too few stillbirths and early neonatal deaths to make any statistical comparison between the two groups (Table 3). DiscussionMost of the grandmultiparous women were Malays and there were a very small number of Chinese. This was reflected by the cultural differences and beliefs between these two ethnic groups. As expected, the grandmultiparous women were much older than the multiparous women. In spite of more patients being in the older age group there was no increase in pre-existing medical disorder except for thyroid disease. Patients with pre-existing medical disorders were often discouraged from having large families and were advised to complete their family as early as possible. These patients were usually counseled for contraception or sterilization. Anemia was still a common problem in these patients (RR=2.681, 95% CI 6.803; 1.152). Lower socioeconomic status and poor spacing, were factors associated with increasing parity. Repeated childbearing depleted the iron store and predisposed to anemia. There were increased iron requirements of about 6mg/day and in addition, there was a need for nearly 1 mg more to compensate for maternal excretion, which made the requirement of a total of 7mg of iron per day (21). This finding of increased anemia was similar to the Malaysian study by Tai and Urquhart (4) and other studies (4,11-14,16) but it contradicted Seidman et al. (1988), which reported no difference in their patients. Even though prophylactic iron and folic acid were given to patients in Malaysia, unfortunately most grandmultiparous women tend to have their bookings later, and hence most of them were already anemic during the first antenatal visit. In developed countries, even though the outcome of the grandmultiparous women was good, there was still a significant association with anemia (12). Non-proteinuric hypertension was significantly higher in this study population as the grandmultiparous patients were in the older age group, i.e., 60% of patients were above 35 years as compared to only 15% in the multips (Figure 3). The reported higher proportion was similar to the findings by several studies (8,10,13,14). However, when matched for age, Bugg et al. (12) did not find any increased risk. In addition, pre-eclampsia, which was a disease of the primip, still occurred in the grandmultips in the Malaysian population but it is not statistically significant compared to the multips (Table 1). There was no difference in gestational diabetes and impaired glucose tolerance although previously reported by others as common complications (6,8-10,15). Moreover, although previous papers reported an increased incidence of malpresentation (5,13), ironically the results of this study showed a lower risk of malpresentation, which contradicted the above papers. Furthermore, most of the previous papers reported an increased risk or no significant difference in prematurity (6, 8, 10, 14) but on the contrary, this study revealed a lower risk among the grandmultiparous women. There was also no significant difference in antepartum hemorrhage as reported by previous studies (6, 9,11,14). In addition, it was also found that there was no significant difference in the complications of placenta previa (4,5,10,13,16) and placental abruption similar to previous reports (10,16,17). The incidence of induction of labor varies widely according to the practice of the obstetrician. Ironically, the induction rate was higher in grandmultips. It is not surprising as there was an increase in non-proteinuric hypertension in the grandmultips. However, in spite of this, there were no patients with ruptured uterus and there was no increase in cesarean section rate. Induction of labor needs to be carefully carried out, as the use of oxytocics in patients with high parity is associated with uterine rupture (22). However, the use of mechanical means to dilate the unfavorable cervix is an option so as to avoid uterine hyperstimulation from prostaglandins in these patients. There is a need for further research to be performed in this direction. The shorter duration of labor in grandmultips in these patients was due to the shorter first stage of labor (P = <0.001) rather than second stage, as this remains constant in both groups (Table 1). Therefore, if prolonged first stage of labor should occur, underlying cephalo-pelvic disproportion should be excluded before augmentation with oxytocics, as birth weights tend to increase with increasing parity and the injudicious use of these agents can cause uterine rupture (22). Even though birth weight increases with increasing parity, there was no significant increase in macrosomia and or shoulder dystocia in these patients. The grandmultipara had a significantly higher intact perineum due to the laxity, therefore, they required fewer episiotomies and were at lower risk of vaginal tears and laceration. The perinatal outcome was comparable, even though the grandmultipara had a higher risk of meconium-stained liquor (MSL) (RR=1.678, 95% CI: 2.564; 1.404, P=0.018) (Table 3). Babinski et al. (5) had reported similar findings of increased MSL. The reason for the increased was unexplained as there was no significant difference in post date pregnancy between the two groups in this study. However, the period of amenorrhea is still calculated from the last normal menstrual period as routine early scan for dating is not performed in all patients since this hospital caters for an average of 24 000 deliveries a year and in addition, most grandmultipara come for late booking. Surprisingly, there was no significant difference in postpartum hemorrhage (Table 1). There was also no significant difference in the mean blood loss in labor. Even though there were studies that reported no difference in incidence (9-11,16) other studies found an increased incidence of PPH (4-8). Fuch et al, (23) reported the increased risk of four times and Munim et al. (24) reported an increased incidence by 3 times. The current practice in MHKL is to give intramuscular syntometrine to all patients in the third stage of labor unless contraindicated. However, in the grandmultipara, prophylactic intravenous oxytocics infusions are also given after delivery and patients are monitored closely in the labour room post partum. Early breast-feeding is also practised. Moreover, the current practices of anticipating PPH in the management of these grandmultiparae are in place. When in labor, steps are taken to place an intravenous line, group and cross match blood and actively manage the third stage. There is an emergency red alert system and staffs are regularly trained to deal with this problem. The limitation of the study was that it was a retrospective study and not all the data were retrievable. This study reflected the performance of the grandmultipara women in MHKL, a referral center in the heart of a cosmopolitan city. Further studies should also be performed in the east coast of Malaysia where the population is rural and extreme grandmultiparity (more than gravida ten) is common. Most of the recent papers concluded that the outcome of grandmultiparity had tremendously improved given that they received adequate antenatal care (5, 9,10,12,17), which is similar to the findings in this study. However, anemia is still a common problem even in the developed country (12). The reasons could be due to poor spacing, late booking and low socio-economic status. Efforts should be made to overcome anaemia in these patients in view of the current findings of fetal origin of adult diseases. ConclusionIn conclusion, the maternal fetal outcome of grandmutiparous women is good and comparable to the multiparous women. The protocol used in MHKL on the management and anticipation of PPH should be explored and further prospective studies performed to compare the outcome with other hospitals. AcknowledgmentsThe Ministry of Health Malaysia, the Director General of Health Malaysia, the Director of Hospital Kuala Lumpur, the Head of Department of the Obstetrics and Gynecology and all doctors and staff of the Obstetrics and Gynecology Department of MHKL for their support and cooperation during the period of the project. Noor Aisyah Bt Abdul Mutholid, Hazlinda Abdul Razak, Noranida Salehudin, and Faizah Ahmad for their technical assistance. This project did not receive any funding. References
© Copyright 2006 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj06023f3.jpg] [mj06023t3.jpg] [mj06023f2.jpg] [mj06023t1.jpg] [mj06023t2.jpg] [mj06023f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}