 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
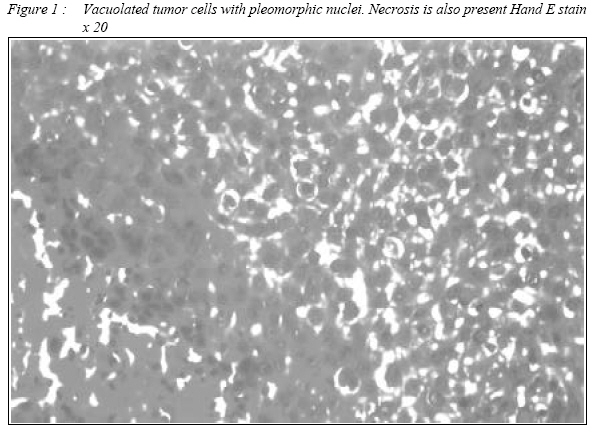
CASE REPORT SEBACEOUS CELL CARCINOMA OF SCALP -A RARE PRESENTATION Venkata Murali Krishna Bhavarajua*, S Ejaz Shamim*, V R Naik**, Shamsol Shaari*** *Department of Nuclear Medicine, Radiotherapy & Oncology, **Departemnt of Pathology, School of Medical Sciences, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia ***Department of Pathology, Hospital Kajang, Malaysia Corresponding Author : Dr. Venkata Murali Krishna Bhavarajua MD Dept of Nuclear Medicine, Radiotherapy& Oncology, School of Medical Sciences, Universiti Sains Malaysia, Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Tel: +609-7663214, Fax: +609-7653370 @ mail: drmurali@kb.usm.my Submitted-20-02-2004, Accepted-03-12-06 Code Number: mj07013 Sebaceous cell carcinoma of the skin is a rare malignancy of the skin appendages. Most commonly noticed in the orbital region. Extra orbital sebaceous cell carcinoma is extremely rare. The aggressive behavior of this tumor is still a matter of controversy. We present a case of sebaceous cell carcinoma in scalp region in young women. Keywords : sebaceous cell carcinoma, orbital, extra orbital, scalp, metastasis Introduction Sebaceous cell carcinoma (SC) is a rare malignancy of the skin appendages. SC is most commonly seen in the orbital region, extra orbital SC is very rare. So far only 150 cases of extra orbital SC were reported in the literature(1-2). The extra orbital SC commonly occurs on head and scalp due to the abundant sebaceous glands (3-4) the other sites involved by SC are external genetalia (5) extremities (6). The true SC is still a subject of discussion both from histopathological and clinical point of view due to its rarity and behavior pattern (7).The present literature is dividing in deciding the aggressive nature of extra ocular SC, Rulon and Helwig (8) noted no metastasis in their analysis of five cases. However the incidence of metastasis is less than 10% in extra orbital SC (9). Sebaceous cell carcinoma is a disease of 6th and 7th decade of life occurs in men and women equally (3).The incidence varies from 0.2% to 4.6% of all skin cancers, the incidence is about 0.6% in people below 20 years of age (10). We present an extra orbital SC in young female with extensive lymph nodal, bone and lung metastasis. Case ReportA 29 year old female mother of two children was referred to the oncology clinic of Hospital Universiti Sains Malaysia (HUSM) for further treatment from the general Hospital complaining of severe neck pain, head ache, awareness of nodule over the scalp. The neck pain was severe in nature with a history of restricted neck movement. The head ache was of one year duration associated with vomiting. The scalp nodule had been present at the same site 3 years earlier. A wide excision was done at a local hospital then and the histopathology reported the tumor as having a limited contact with the epidermis and extended into the dermis in columns. The architecture of the tumor was somewhat lobular. A few lumina resembling sebaceous ducts were present within the tumor. The tumor cells were cytologically malignant and there was variation in the diameter of the vacuoles within a given cell. This was reported as sebaceous cell carcinoma (Figure 1). The patient was asymptomatic for one year following the surgery but subsequently developed a recurrent nodule at the same site along with headache, not responding to analgesics. She was admitted to the General Hospital, Kota Bharu in Sept 2004 and underwent a CT scan of the brain and head and neck region. Tumor recurrence was seen in the occipital region with destruction of bone and local infiltration into the meninges (Figure 2).The patient was referred to the HUSM for further management. At examination although alert she was experiencing cervical neck pain. Proptosis of the right eye was noted. A nonhealing ulcer in the occipital region of the scalp was also seen. A detailed examination of the eyes and the CNS at presentation was not done due to poor cooperation from the patient. However she had a sixth and seventh nerve palsies on the right side. Multiple lymph node enlargement was noted in the cervical and supra clavicular regions. Fine needle aspiration cytology of the lymph node revealed a poorly differentiated carcinoma. A single fraction of 800 cGy external radiation was given to the thoracic spine for pain relief. The patient was reviewed a month later in the oncology clinic. She had significant pain relief from the radiation treatment. She was started on oral morphine for better pain control. Single agent chemotherapy with mitomycin-C was proposed she declined. A CT scan of the abdomen was planned to evaluate abdominal involvement or liver metastasis. A colonoscopy was deferred in view of her poor general condition. She succumbed to the disease three months after the presentation. DiscussionExtra orbital sebaceous cell carcinoma (SC) has a different behaviour compared to the orbital SC which is considered less aggressive than orbital SC (11). The clinical behavior and characteristics are still a mater of controversy in the literature (7). Mellette et al for instance found that the biological behavior of extra orbital SC is not different from the orbital SC (12). The other sites reported in the literature are the parotid and the submandibular glands, buccal mucosa, laryngeal and pharyngeal cavities, the trunk and the upper extremities and the external genitalia. The histological criteria for SC are high mitotic activity, nuclear pleomorphism, lobular architecture and foamy vacuolization of the cytoplasm (9). Histologically SC divided into three types sebaceous adenoma, basal cell carcinoma with sebaceous differentiation and sebaceous carcinoma (13). The present literature is divided on the aggressive nature and metastasis potential of extra ocular SC (5,8,14). Extra ocular SC is known to recur locally and spread to lymph nodes and visceral organs (15). Histologically the poor prognostic indicators are poor differentiation, presence of lymphatic or vascular permeation, presence of Pagetoid cells shown in histology and immuno histochemical staining (16, 17). The biological behavior of SC is still open for discussion as there are varied opinions about the incidence of local and distant failure in patients with extra orbital SC (18). Due to its rarity with only about 150 cases reported in the literature so far there is no single opinion on the aggressive nature of the disease. However the series by Wick, King and Hernandaz showed the distant metastasis occurred inpatients with extra orbital SC. The present case is different from that in the literature in that this malignancy occurred in the 3rd decade of life. The patient had recurrence of disease at the primary site one year after the initial surgery and very locally aggressive with bone, meningeal and regional lymph nodes infiltration. The lungs and vertebral columns were also involved with metastasis. The role of adjuvant treatment with radiation and chemotherapy after surgery is not clear in the extra ocular SC due to its rare presentation. We treated the patient with external radiation with a palliative intent and advised chemotherapy as the patient was young. We conclude that the extra ocular SC is an aggressive skin malignancy and needs to be radically treated by surgery followed by additional treatment depending on the prognostic features as discussed above. Patients with extra orbital SC have to be followed up closely for assessment of recurrence and distant metastasis. References
© Copyright 2007 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj07013f1.jpg] [mj07013f2.jpg] |
| |||||||||

{kind=link}
{kind=link}