 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
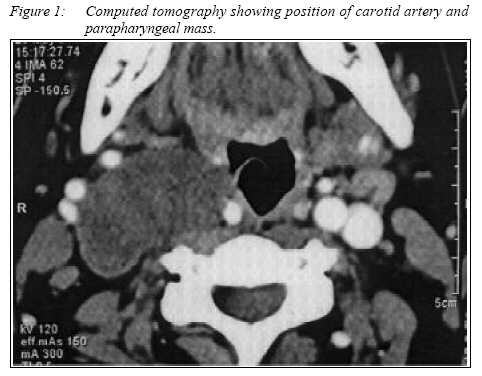
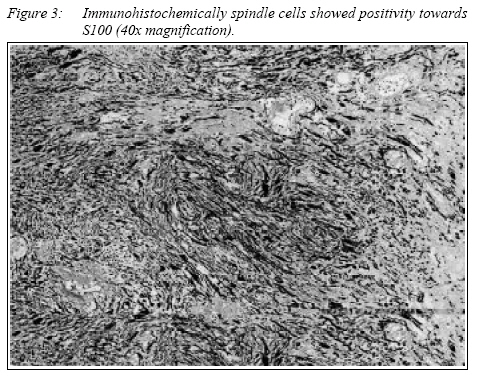
CASE REPORT ANCIENT SCHWANNOMA OF THE CERVICAL SYMPATHETIC CHAIN : A CASE REPORT Primuharsa Putra Sabir Husin Athar, Norleza Ahmad Norhan1, Megat Shiraz Megat Abdul Rahman2 Ear, Nose & Throat-Head & Neck Consultant Clinic,
Seremban Specialist Hospital, Seremban, Negeri Sembilan, Corresponding Author : Dr. Primuharsa Putra Sabir Husin Athar MD (UKM), MSurg ORL-HNS (UKM), AM (Mal), FAAO-HNS (USA). Ear, Nose & Throat-Head & Neck Consultant Clinic, Seremban Specialist Hospital, 70200 Seremban, Negeri Sembilan Darul Khusus, Malaysia. Tel: 06-767 7800 Direct line/Fax:06-7653406 E-mail: putrani@ssh.kpj.com.my Submitted-20-02-2004, Accepted-03-12-06 Code Number: mj07015 Schwannoma of the cervical sympathetic chain is an extremely rare nerve tumour. We report an unusual swelling in a 41-year-old female who presented with an asymptomatic solitary mass in the right parapharyngeal space. Clinical examination and computed tomography showed displaced carotid artery in an antero-medial direction. Surgical excision of the lesion was carried out and histological examination revealed an Ancient Schwannoma. Keywords : Ancient Schwannoma, Cervical Sympathetic Chain, Case Report Introduction It is estimated that 40 to 50 percent of schwannoma occurs in the head and neck region. Schwannoma arising from the cervical sympathetic chain is very rare and approximately 57 cases have been reported (1). Case Report A 41- year - old Malay female presented with 20 years history of painless right upper neck swelling. It was gradually increasing in size. There was no associated symptoms of dysphagia, odynophagia, hoarseness, dyspnoea, upper limb weakness or numbness. Examination revealed a vague mass deep to sternocleidomastoid measuring 3 x 4 cm in the upper third of the right neck. Carotid pulse was palpable in an antero-medial direction. It was firm, mobile, non-tender and non-pulsatile. There was no bruit or any cranial nerve palsies. Oropharyngeal examination showed the right lateral pharyngeal wall was pushed medially. Other examinations were unremarkable. Fine needle aspiration produced insufficient material for cytological examination. Computed tomography revealed a soft tissue mass in the right parapharyngeal space pushing the lateral pharyngeal wall medially. Carotid artery was displaced antero-medially as shown by clinical examination (fig. 1). In view of the possibility of nerve in origin, risk of nerve injury was explained to the patient preoperatively. Intraoperatively the mass was exposed through a cervical incision. It was found to be situated deep to the carotid artery and jugular vein. After identifying the vagus nerve, hypoglossal nerve and accessory nerve, the mass was bluntly dissected from the carotid artery and jugular vein. The mass was seen clearly arising from the cervical sympathetic chain. As the nerve encroached the mass posteriorly, it was seen splayed out and became so thin. The mass was excised completely with an intact capsule. Post-operatively a right sided Horner’s syndrome was observed. Histologic examination showed spindle cells, loosely arranged and occasional cells with bizarre, hyperchromatic nuclei but no mitotic figures (fig. 2). Immunohistochemical assay revealed positivity to S100 (figure 3) and Vimentin, but are negative for CK, EMA, desmin, smooth muscle actin and CD34. The final diagnosis was hyalinised schwannoma (Ancient schwannoma). Discussion Schwannoma is a benign, slow growing, solitary tumors of schwann cells. They are well encapsulated and characteristically running along or attached to the peripheral, cranial or sympathetic nerves except in the optic and olfactory nerves, which lacks schwann cells sheath. The specific details of their genesis is not known. Microscopically, schwannomas have a distinctive pattern of compact cellularity arranged with palisading nuclei (Antoni A pattern) alternating with a more loosely arranged hypocellular pattern (Antoni B pattern) (2). Occasionally schwannomas may present with hyperchromatic areas and bizarre nuclei. These cellular changes reflecting degeneration are typical of the so-called ancient schwannoma (3). Neurilemmomas occur at any age, but majority between 30 and 60 years of age (4). In the neck, the vagus nerve is the most commonly involved nerve, followed by the cervical symphathetic nerve (5). Schwannoma of cervical symphathetic chain are extremely rare and usually present as masses in the parapharyngeal space. The presence of Horner’s syndrome before resection is rare (6) and this only indicates cervical symphathetic chain involvement, not the nerve of origin (7). Horner’s syndrome is quite common in the postoperative period and usually resolved over time (6). Preoperative FNAB is not often precise as shown in this case. A contrast-enhancing CT or magnetic resonance image is the cornerstone of pre-operative planning. Angiography is indicated for those masses that enhance on imaging studies, including neurogenic tumors and paragangliomas. The presence of vascular displacement is helpful in determining tumor origin. Anteriorly displaced internal carotid artery is characteristic of neurogenic and vagal paraganglioma, whereas salivary gland tumors generally cause posterior displacement (2). In our case, CT scan revealed a displaced carotid artery in the antero-medial direction. This finding is consistent with our clinical examination. Vagal schwannoma typically results in an increased distance between the internal carotid or common carotid artery and the internal jugular vein, whereas tumors that arise from the cervical sympathetic chain do not7. Surgical excision is the treatment of choice for these tumors (8). Cautious surgical treatment include extracapsular ‘peeling’ or even intracapsular enucleation of the tumor from the nerve in an effort to preserve the function of the nerve. If the lesion is known to be a schwannoma, it is possible to open the capsule and shell out the tumor, thereby leaving the capsular nerve fibres undisturbed and possibly avoiding functional deficits (9). In this case, however, the tumor apparently was too intimately associated with the cervical sympathetic chain to preserve the function of the cervical sympathetic fibers. A graft was not attempted in this case. References
© Copyright 2007 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj07015f3.jpg] [mj07015f1.jpg] [mj07015f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}