 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
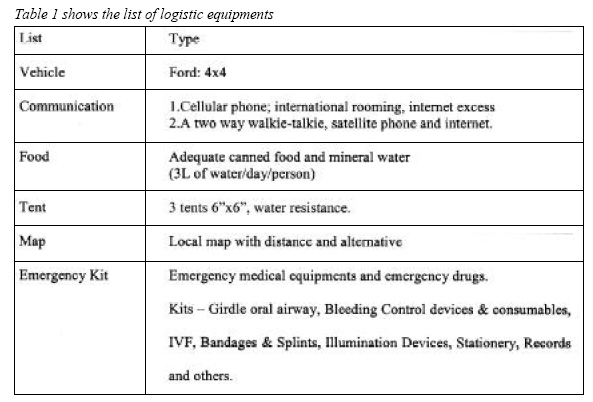
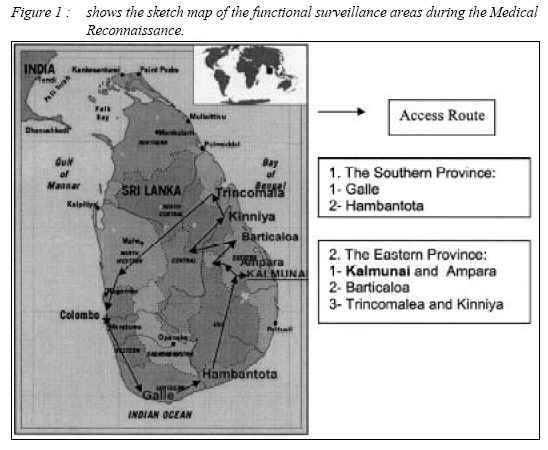
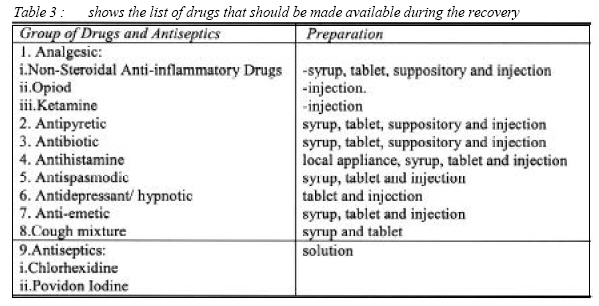
SHORT COMMUNICATION POST-IMPACT DISASTER SURVEILLANCE - A MEDICAL RECONNAISSANCE TEAM AT TSUNAMI-STRUCK SRI LANKA Nasir Mohamad, Nor Hidayah Abu Bakar, Nik Arif Nik Mohamed, Kamarul Aryffin Baharudin, Abu Yazid Md Noh, Rashidi Ahmad, Nik Hisamuddin Nik Abd. Rahman Emergency and Trauma Research Group, Department of Emergency Medicine, School of Medical Sciences, Universiti Sains Malaysia, Health Campus 16150 Kubang Kerian, Kelantan, Malaysia Corresponding Author : Dr. Nasir Mohamad MD (USM), MMed (Emergency Medicine) USM Department of Emergency Medicine, School of Medical Sciences, Universiti Sains Malaysia, Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Tel: +609-7663353 Fax: +609-7663353 email: nabil_mohamad@yahoo.com Submitted-20-02-2005, Accepted-03-12-06 Code Number: mj07016 Emergency Medicine and Disaster Medicine are two specialties which are similar in the multidisciplinary involvement during the acute phase of the disaster. Recently, there was an increase in the number of disasters in the world but not many physicians are familiar with the principles for dealing with such situations, the unique organizational demands, coordination and the urgent need for medical assistance and relief. This case report delineates our experiences at a tsunami disaster area and the approach to setting up a medical relief team in the affected area. A medical reconnaissance team comprising of an emergency doctor from Hospital Universiti Sains Malaysia (H.U.S.M) and two MERCY Malaysia members was assembled. The team flew to Colombo on day 5 after the tsunami with medical supplies and related materials. The mission started from December 31st 2004 until January 8th 2005. Our surveillance area covered the Southern and Eastern Province with a total distance of 1700 km along the coast. The strategies employed during this medical reconnaissance included risk analysis, devising a resources matrix, developing lines of communication and rapport with other relief teams, Sri Lankan government agencies, and local and international non-government organizations. As a result, our team was able to set up a medical relief camp and distribute the relief items to the tsunami victims. In conclusion, the Disaster Emergency Medical Assistant Team (DEMAT) from H.U.S.M and MERCY Malaysia were able to set up and provide medical relief with our limited resources to a large scale disaster situation. Keywords : medical reconnaissance, tsunami Introduction On 26th December 2004, exactly a year after the disaster in Bam, Iran, the biggest earthquake in the past 40 years measuring 9.3 on the Richter scale, triggered a tsunami which struck countries in between the Australian and Eurasian plates in the Indian Ocean. This disaster was totally different from Bam, Iran in that the epicenter of the earthquake was below the sea, hence resulting in a Tsunami (1, 2). Following the release of such a tremendous amount of mass and energy contained in a tsunami, the giant wave damaged structures and more than 150,000 people listed as missing and millions of people becoming displaced. Eleven Asian countries were affected. A few areas such as Banda Aceh, Sri Lanka, Phuket, Maldives, Myanmar, Malaysia, Bangladesh, and India were badly affected. In Sri Lanka alone, there were nearly 100,000 families displaced, with 88,500 houses destroyed and a death toll of approximately 31,000 (3, 4). Disasters are considered as low-probability but high-impact events. It disrupts the normal life of the population. The World Health Organization (WHO) defines a disaster as “a sudden ecological phenomenon of sufficient magnitude to require external assistance” (5) Each disaster follows a general pattern in its development which is often repeated throughout nature. It can be divided into the phases of impaction, then rescue and finally recovery. With time, it is preceded by prodromal or warning and subsequently quiescent level (5, 6, 7). Sequence of the EventsMERCY Malaysia, a non-governmental organisation from Malaysia and Disaster Emergency Medical Assistant Team (DEMAT) from H.U.S.M had made a step forward by forming a medical reconnaissance team. This comprised of three members including an emergency doctor from HUSM and two Mercy Malaysia personnel. The team flew from Kuala Lumpur International Airport to Colombo on day 5 of the disaster. Our aim of this mission was to set up a medical relief and humanitarian aid camp. The main objective of the mission was to carry out risk analysis of the disaster area before a medical relief camp could be set up. The mission took 9 days starting from December 31st 2004 until January 8th 2005. Our area of surveillance covered a distance of 1700 km, along the coastline. The Southern Province included Galle and Hambantota while the Eastern Province included Kalmunai, Ampara, Barticaloa, Trincomalea and Kinniya. The materials and logistic equipments are listed as below. (Table 1) ResultsThe MERCY and (DEMAT), HUSM from Malaysia were able to set up a medical relief camp and distribute the relief items to tsunami victims at the affected areas, especially in the districts of Ampara, which is located in the Eastern Province of Sri Lanka. We are managed to see more than 100 patients a day. The common diseases encounted were post traumatic stress disorder (PTSD) (50%), wound infection (20%), upper respiratory tract infection (10%) and others 20% includes headache, acute dysentery, food poisoning, skin infection and myalgia. A very tight surveillance schedule was produced so as to assure that the affected areas were well assessed (Figure 1 and Table 2). The focus was mainly on the areas that were most in need of relief services. DiscussionThe most difficult part during the disaster assessment was the badly damaged infrastructures. As a result of the large scale damage to buildings, transport networks and communication lines, the coordination of relief was very poor and ineffective. The most commonly encountered problem associated with any disaster is a breakdown in communication. This communication breakdown was due to the sudden increase in the volume of transmission and the need to communicate between the victims, responders and witnesses of the disaster. Subsequent shortages of personnel and supplies limited the rescue phase (8). The provision of health care in these scenarios requires professionals who understand the complex international humanitarian system and how it functions. This includes a working knowledge of the major participant bodies, international humanitarian law, epidemiology, malnutrition and communicable diseases, gender reproductive issues, public health infrastructure, logistical needs and transportation, field security, negotiations and mediation skills, and a critical understanding of psychosocial and cross-cultural issues (9) It was the 5th day after the tsunami struck when our team arrived. The period of urban search and rescue (USAR) and confined space medicine (CSM) was already over. It was now the period of recovery. An understanding of the disaster environment and knowledge of CSM will enhance the survival of and reduce morbidity in the extricated patient. Assessment needs to begin as soon as possible to maximize survival potential (10). Meeting with local government authorities such as the Sri Lankan Ministry of Health in order to highlight our presence and get our organization registered was the most important step. We also gathered all the information regarding the current situation of the disaster sites, the number of relief organizations involved, the types of relief aids that were needed, data on the relief camps and displaced people, information on any epidemics or outbreaks of communicable diseases, logistical and safety issues (11, 12, 13). Subsequently, a meeting with all international and local relief agencies was done. It was coordinated by the United Nation representative. It was a daily meeting, usually scheduled at the evening or night time. During these sessions, risk analyses and resource matrixes were evaluated. Our targeted areas were the southern and eastern costal areas which were badly affected. A route to be taken was planned with a tight schedule and expected time of arrival (Figure 1 and Table 2). With our experienced members, the mission went on smoothly. We were moving onto public health issues and communicable diseases. We selected Kalmunai as our preferred site for the medical base camp. The decision for selecting Kalmunai was based on the current status of health services, the numbers of displaced people at relief camps, the accessibility and availability of logistics and finally, the good coordination with the local government agencies. Most of displaced people (50%) suffered from post traumatic injuries and post traumatic stress syndrome (PTSS) .There was no large scale outbreak of infectious diseases because early preventive measures were undertaken by the local and international health organizations such as immunization, clean water and food supplies and proper clean sanitation. There were only isolated cases of acute dysentery, upper respiratory tract infections, wound infections, skin infections and other infections of the sort that were spread by fecal-oral routes. Early medical attention should be stressed on primary health care like emergency medicine and family medicine during the acute phase with a good support from public health services. The drugs that should be made available during this phase were also depending on the common encountered diseases (Table 3). Later, the emphasis should shift to community-based medicine and psychiatric consultations during the intermediate phase and then, finally, to proper plans for the tertiary and quaternary phase later once the disaster area becomes more stable. The best place to learn Disaster Medicine is at the disaster site and the best teacher to teach Disaster Medicine is through one’s own experience. You never understand it until you experience it yourself. ConclusionIn conclusion, the strategies during medical reconnaissance in a disaster area are risk analysis, resource matrix, good communications, and establishing a good rapport with other relief teams, government agencies, and local and international non government organizations. Acknowledgement :The authors would like to thank the dean, School of Medical Sciences, Universiti Sains Malaysia and MERCY Malaysia. A special gratitude to Assoc. Prof Kamarudin Jaalam, Dr. Wan Asim Wan Adnan, Dr Kam Chak Wah (Hong Kong) and Dr Goh Sin Hiong (CGH, Singapore) for their support. References
© Copyright 2007 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj07016f1.jpg] [mj07016t3.jpg] [mj07016t1.jpg] [mj07016t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}