 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
REVIEW ARTICLE How to Develop a Core Curriculum in Clinical Skills for Undergraduate Medical Teaching in The School Of Medical Sciences at Universiti Sains Malaysia? Shahid Hassan Department of Otolaryngology & Medical Education,
School of Medical Sciences, Universiti Sains Malaysia, Health Campus,
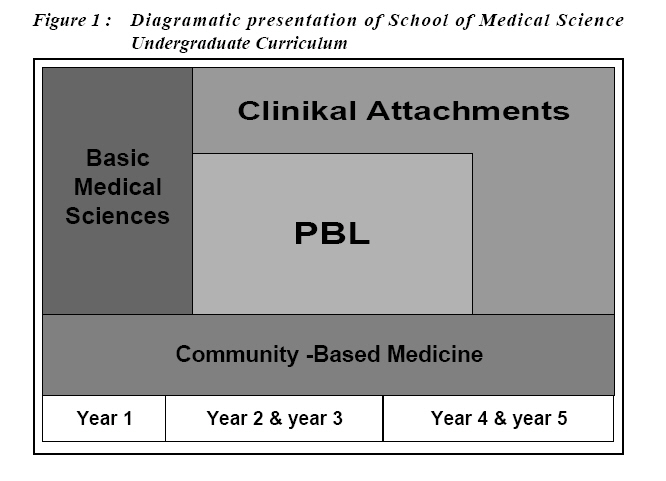
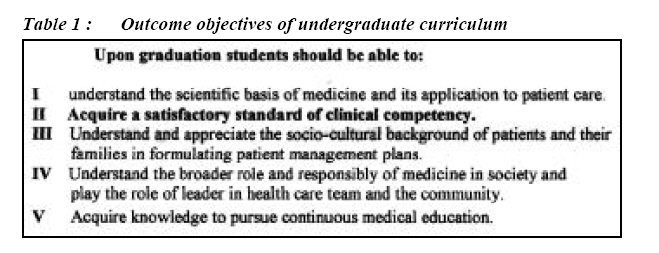
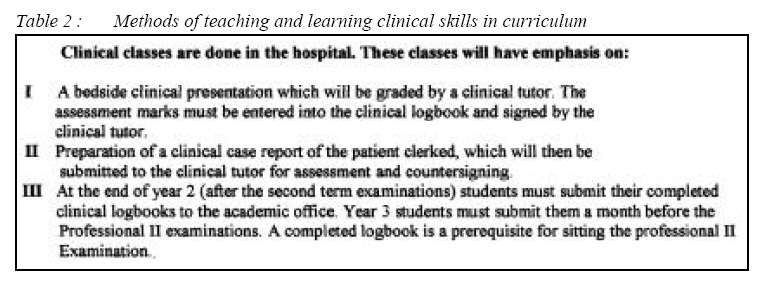
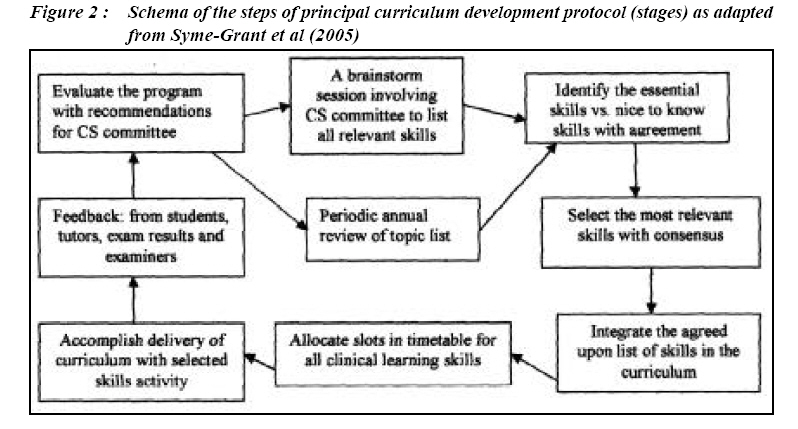
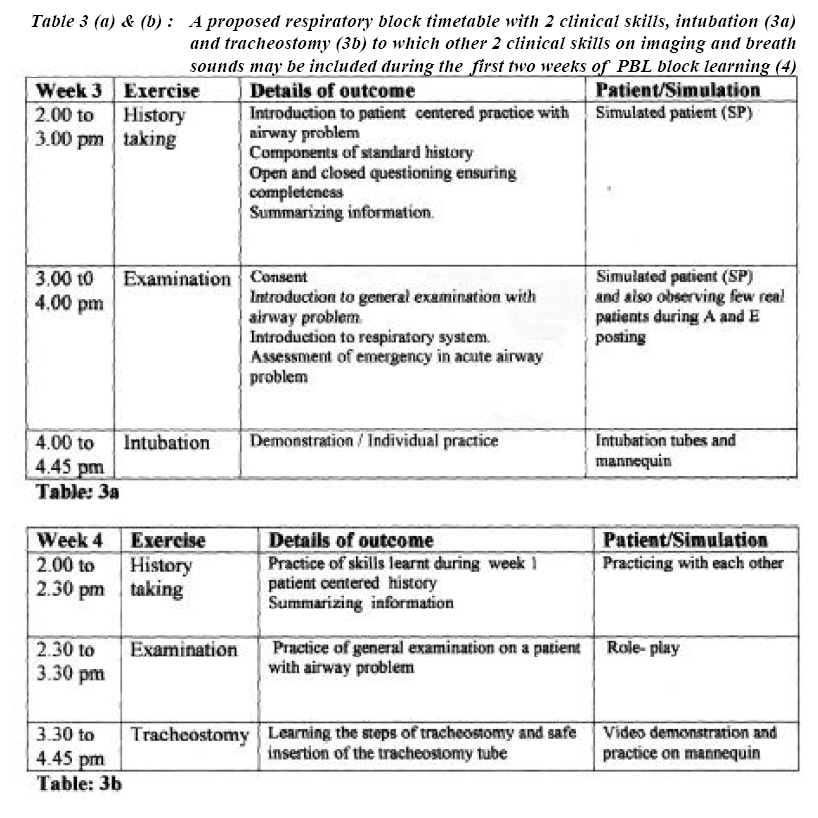
16150 Kubang Kerian, Kelantan, Submitted-6.11.2005, Accepted-15.12.2006 Code Number: mj07018 Clinical skills program as a laboratory method is a valuable adjunct to other forms of undergraduate medical training. This article describes the process of developing a core curriculum in clinical skills based on the Dundee model for a clinical skills centre. The School of Medical Sciences, in Universiti Sains Malaysia (USM) has been provided with a well equipped skills centre. However, the PBL curriculum in the undergraduate medical program in the school needs to be integrated with a clinical skills lab program. This is to counter the general feeling that the contribution of PBL is insignificant in terms of building clinical competency in an integrated system such as that used in USM compared to the traditional curriculi of other medical teaching institutions in Malaysia. Integrating clinical skills laboratory training with the PBL curriculum will provide evidence of PBL as an effective and innovative method for teaching and learning in Malaysia. Key words : Clinical skills, skills lab, core curriculum, integrated clinical skills program Introduction Core curriculum and outcome objectives and the use of problem-based learning with self directed experiential approach is the adoption of adult educational principle used by many medical institutions. The outcome objectives of a curriculum provides the blueprint against which the results of the training can be judged. Attaining a satisfactory standard of clinical competency is the objective of every medical education curriculum at undergraduate as well as postgraduate levels globally. The external drive for clinical skills training comes from recommendations by medical professional bodies, an increase in student numbers, and the fact that patients’ nowadays are less tolerant of being examined by novices. The internal drives are sociopolitical and cultural influences, problem based learning approaches and a move from hospital to community and primary health centers in healthcare practice (1). Changes in the health care profession, community needs and innovative learning strategies in medical education were the motivating factors 25 years ago behind the creation of the School of Medical Sciences (SMS) at Universiti Sains Malaysia. The ultimate objective of SMS was to produce doctors that have a different approach and attitude from that being produced by the other two institutions utilizing traditional curricula at that time (2). The curriculum adopted for SMS was based on a PBL method of learning and community-based medical education using the Community and Family Case Study (CFCS) program (Figure 1). This new curriculum demanded students to master a range of prescribed clinical skills to be able to utilize and feel self-sufficient while working in community away from the institution and faculty supervision. If the curriculum is the constitution of an educational program then the outcome objective is the backbone of the curriculum. The outcome objectives of the SMS curriculum stated in Kurikulum Asas Semakan 1996 (Table 1) expects that upon graduation students will acquire a satisfactory standard of clinical competency. However, the method to be adopted for clinical skills learning as elaborated in the “Guidance and Objectives of Phase II of Sidang Akademic 2005/ 2006” (Table 2) emphasizes that these clinical skills will be acquired through a hospital teaching on real patients. SMS is the first medical school in Malaysia that has adopted an innovative curriculum. It features integration; a problem based learning approach and community orientation. It is committed to produce community-inspired practitioners who are able to look at problems holistically and apply solutions to those problems at individual as well as at community (2) level. The curriculum introduced many years ago was aimed at producing doctors who become competent in clinical skills rather early in their training to cope with community postings under the CFCS program where they are expected to work independently without direct supervision. Are we really producing such role-model medical graduates compared to those produced by medical schools practising traditional curricula? Incidentally the pattern of hospital-based clinical skills training of our graduates and those following traditional curricula are similar except that USM graduates are exposed to clinical skills methods as early as in year 2 (Phase II) at which point problem-solving teaching have yet to be started. At this stage, the students’ learning curve have just started and a full blown clinical exposure at this stage may have negative effects. Though an early clinical exposure of undergraduates is considered mandatory for PBL, it definitely demands a guided clinical environment to avoid students from suffering reality shocks due to insufficient preparation for adequate work-up of real life patients in clinics. This guided environment is best provided by clinical skills lab methods in a clinical skills center (CSC). CSC provides a useful clinical environment especially when clinical teaching is introduced early in the curriculum as it has both horizontal and longitudinal integration in an innovative curriculum (4). How can this training requirement be achieved through an effective clinical skills centre in School of Medical Sciences is described in this article. Identifying the problem in PBL curriculum of SMS Clinical skills program involves the second and third phases of the SPIRAL curriculum of SMS. However, the teaching through Phase II is horizontally integrated to the physiological system and this in turn runs vertically through out the five years of the curriculum. In the morning students attend system integrated lectures followed by PBL tutorials. Afternoons are devoted to wards and outpatient teaching while reserving some time for self-directed learning. Organizers at the skills centre, somehow manages to squeeze little time out of the schedule in the afternoon to offer training in a few selected clinical skills. The question is that do this arrangement provides enough time for skills training in a lab setting? For instance in the respiratory block, do we teach students on those skills, with adequate supervision, and then provide them with further time to practice those skills as independent learning? This is important for a skills lab method of learning. We must aim to ensure that training in the clinical centre is timed well to introduce each skill effectively as preparation for subsequent clinical attachment. Once we achieve this objective, we will be in a position to claim that an effective integration of PBL with that of clinical skills methods has been achived successfully. Presently USM students in Phase II follow a training program in the skills lab in which the CSC attempts to achieve the objectives of the organ system block teaching. The obvious major problem is the lack of integration of our PBL curriculum with such clinical skills training program although the skills centre are very well equipped. This lack of intergration appear to make the efforts of the CSC as isolated from the flow of the curriculum. We must be reminded that a clinical skills lab is primarily a learning method. A well-designed program developed for the clinical skills centre and integrated with PBL will help to fill the gap between theory and practice and contribute greatly to the effectiveness of a medical curriculum. Developing a core curriculum in clinical skills in SMS To develop the core curriculum in skills lab training we recommend the Dundee clinical skills centre model (5). As the first step in this model, we need to create a clinical skill curriculum development group. This group, which should include the skills lab co-coordinator, Phase II and III coordinators, block coordinators, some enthusiastic senior lecturers and clinicians, will be engaged in clinical skills model development. It is mandatory that all participating clinicians should be interested in undergraduate teaching and PBL as an education method. The group should work in a systematic manner in stages (Figure 2) as under. Step 1 (a and b): Brainstorming and Identifying skills. Each system in block teaching should periodically identify clinical skills related to its teaching. This stage must be imaginative and inclusive. Subsequently the group will set the priority of clinical skills in terms of “need to know” vs. “nice to know”. History taking and examination should rank higher in the list of competency components. The horizontal and vertical integration of clinical skills should always be kept in mind together with USM’s SPIRAL concept of the curriculum e.g. advance procedural skills such as terminal illness can be taught in subsequent years rather than in the beginning of Phase II teaching. There has to be a consensus in defining essential clinical skills for each block teaching. Step 2: Best updated clinical skills A senior practicing clinician in that particular discipline should be invited to comment on the prioritized list, keeping updated clinical skills in view. He may also help to identify an appropriate person to develop the protocol together with a demonstration model. Guidance from the outcome objective of USM curriculum should be used to align clinical skills with undergraduate teaching. Step 3: Curriculum Integration This is one of the most important steps in which the curriculum development group will carefully integrate the PBL teaching in each block with clinical skills whilst keeping an eye on the overall teaching of years 2 and 3. Areas of duplication must be avoided whilst maintaining the horizontal integration within blocks. Vertical integration at various phase levels should be decided at brainstorming sessions of the curriculum development group where everybody must be present. Step 4 (a and b): Timetabling and Teaching methodology This is the most important stage of curriculum development and needs good coordination between the skills lab, Phase and block coordinators to optimize teaching of clinical skills in conjunction with block teaching. This will ensure appropriate sequencing and time allocation for each skill. The skills lab training must be guided by the detailed description of outcome of each skill to be trained. The mode to accomplish delivery of the curriculum with selected CS activity is also decided and agreed upon by all coordinators. Step 5 (a and b); Feedback and Evaluation The coordinator clinical skills committee will collect feedback from all stakeholders such as students, tutors, and examiners to evaluate the clinical skills training program. Recommendations can later be prepared based on the feedback for further consideration of committee members during the annual review meeting. Step 6: Periodic annual review Annual review of clinical skills program should be done by the curriculum development group based on the evidences drawn from the student’s feedback, examination results and visiting external examiners critique of the clinical teaching. All stages should be revised in an annual review meeting as a routine practice. To use this model we propose a clinical skills lab program in the respiratory block, which starts early in year 2 of Phase II teaching. Intubation and tracheostomy are identified as clinical skills to be taught in a comprehensive timetable (see Table 3). This block comprises of 4 weeks and follows the General block and the CFCS program. The first two weeks can be allocated to study breath sounds, imaging in respiratory diseases and some core skills (if desired) pertaining to investigations like arterial blood gases and pulse dosimeter. These core skills and tracheostomy can alternatively be taught later in the curriculum as advanced skills in Phase III if not accommodated during these 4 weeks. Week 3 and 4 will discuss the patient with airway problem and its management (Tables 3a and b) A finalized list of competences considered as essential for this block is listed as follows : history taking, general examination (hand, face, tongue etc), examination of the chest and respiratory system, imaging, assessment of airway emergency, completing laboratory request forms and intubation and tracheostomy. Realizing the importance of early exposure to clinical methods in year 2, the teaching will be designed to concentrate in fundamental aspects of the core curriculum (see Table 3). Thus the time allocated for history and examination therefore will be greater compared to completing laboratory forms and understanding investigation procedures. Later in the program more core skills may be included for example, to discuss investigations like arterial blood gases, pulse oximetery and others. Once the objective of mastering basic skills in the respiratory block is achieved it can be applied to a wide range of situations with real patients during subsequent clinical postings. Discussion It has been observed that the best outcomes are achieved when PBL is integrated with a clinical skills lab program in the timetable since many students find learning procedures on real patients very stressful (6). Therefore the lack of a welldesigned skills lab program for training in soft skills such as history taking and application of examination methods will inhibit them from performing the task well. This will in turn result in poor understanding of the educational value of any innovative program. This is specially likely to happen when students in their early clinical teaching is exposed to clinical practice with real patients in wards or outpatient clinics. The PBL curriculum, if modified as proposed, will be unrecognizable in the traditional sense as the results of the teaching will than be seen as attainment of measurable outcomes rather than the mere going through of an organ system or discipline-based blocks. Performance of good clinical skills are not limited to medical students, they are also expected of residents of internal medicines (7). The increased use of simulation technology to supplement skills training with repetitious, standardized training would appear to be a logical solution to the problem. Several key organization have recognized the role of simulation technology in medical education and have recently implemented guidelines or programs to foster its development (8). Despite the availability of devices with advanced simulation technology many medical schools fail to employ such devices to teach and evaluate learners’ skills (9). The mere presence of these tools is not enough. Evidence based outcome must guide medical educators who are willing to bring effective change. Outcome objectives of problem based learning perhaps may also be best achieved by integrating PBL with clinical skills lab training as experienced by the University of Maastricht medical education program for undergraduate students (10). Outcome-based medical education in itself is an innovative model, which provides a powerful performance-based approach at the cutting edge of curriculum development (11). In PBL we have adopted an organ system approach which uses clinical scenarios as triggers. In each PBL block students undergo collaborative learning which promotes discussion, self directed learning and acquisition of knowledge without the presence of real patients during each small group sessions. There is a gap in the acquisition of knowledge and its application (practice on patient) unless an exposure to relevant patient is achieved either through an immediate encounter of real patients in the clinic or ward (which is difficult to arrange most of the time) or simulated patient/ mannequin in a CSL setting (which is always available). Furthermore, the probability of getting the type of patients relevant to the discussion points in the PBL trigger for specific clinical skills demonstration and practice may not be possible due to the unusual practice of haphazard and opportunistic clinical teaching. Learning through problem-based clinical scenarios in the early part of medical education (year 2) compared to clinical teaching in traditional medical education (year 3 and year 4) require at least a demonstration of clinical skills related to the problems discussed in the triggers. This can be achieved by clinical skills training coordinated with PBl in the timetable. This particularly will help clinical training of those students who have not yet undergone clinical exposure and prevent reality shock due to lack of experience. Learning the skills through CSC allows students to practice the clinical procedures as soon as they learn about it theoretically. Training with SP or mannequin allows mistakes and repetition of skills. This helps in building their confidence for subsequent handling of real patients. Additionally the collaborative and peer learning environment provide them with an instant feedback especially in the absence of supervision which is not very uncommon in our clinical setting. Increasing awareness of patient consumerism and decreasing number of patients in clinics are the other problems linked to a traditional clinical learning. A successful implementation of clinical skills program in Phase II will give us sufficient and adequate experience to expand our clinical skills program to Phase III and maybe even in Phase I as well. Though clinical teaching in Malaysia, like many other developing countries, uses hospitalbased clinical teaching with real life patients for undergraduate medical education, the ever increasing number of students in medical colleges results in failure to maintain a balance between the available resources (real patients) and the learners (medical graduates). This fact has been experienced in Europe and rest of the developed countries. The pre-clinical lab-based skills training will complement the ward and ambulatory clinical teaching to attain better motivation and pleasure of learning. The ideal PBL environment should have a learning task cycle comprising of PBL, skills lab and self-directed learning. The School of Medical Sciences, USM has been blessed with a wellequipped clinical skills centre where skills training program is being run on the basis of see-one doone. Though a skills lab is an expensive facility and a dream for many medical institution it has been established in School of Medical Sciences, USM with updated facilities. An adequate utilization of the clinical skills centre using a well-defined curriculum integrated with PBL is essential for maximum efficiency of our curriculum. Adopting clinical skills training integrated with PBL in Phase II (year 2 and year 3) as suggested above will not only define our core curriculum for clinical skills program but will also help to achieve the outcome objectives of the curriculum of the School of Medical Sciences and allow our students to acquire satisfactory standards of clinical competency. Conclusion The outcome objectives of the PBL curriculum can be achieved more efficiently if it is integrated with the clinical skills lab program and introduced in the preclinical years of medical education in Phase II at the School of Medical Sciences. This will facilitate a sound and safe clinical skills training of medical students prior to their exposure to real life patients in subsequent clinical years of Phase III and also during their internship training after the graduation. References
© Copyright 2007 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj07018t3.jpg] [mj07018f2.jpg] [mj07018f1.jpg] [mj07018t1.jpg] [mj07018t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}