 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
ORIGINAL ARTICLE Hospital Outcomes of Adult Respiratory Tract Infections with Extended-Spectrum B-Lactamase (ESBL) Producing Klebsiella Pneumoniae Li-Cher Loh, Nor Izran Hanim bt Abdul Samad, Rosdara Masayuni bt Mohd Sani, Sree Raman*, Tarmizi Thayaparan*, Shalini Kumar** IMU Lung Research, International Medical University, Kuala Lumpur, Malaysia;
*Department of Medicine, Seremban Hospital, Negeri Sembilan, Malaysia; **Department of Pathology,
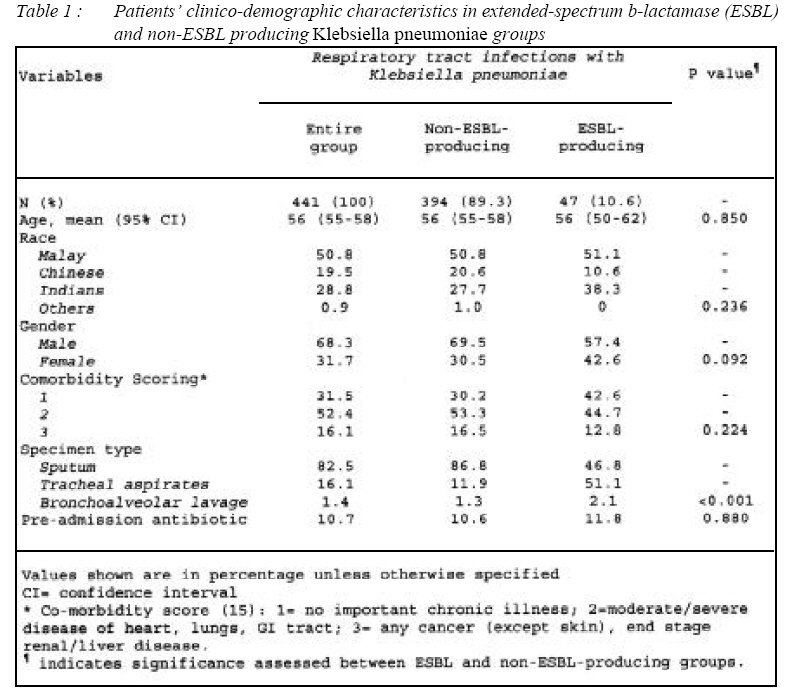
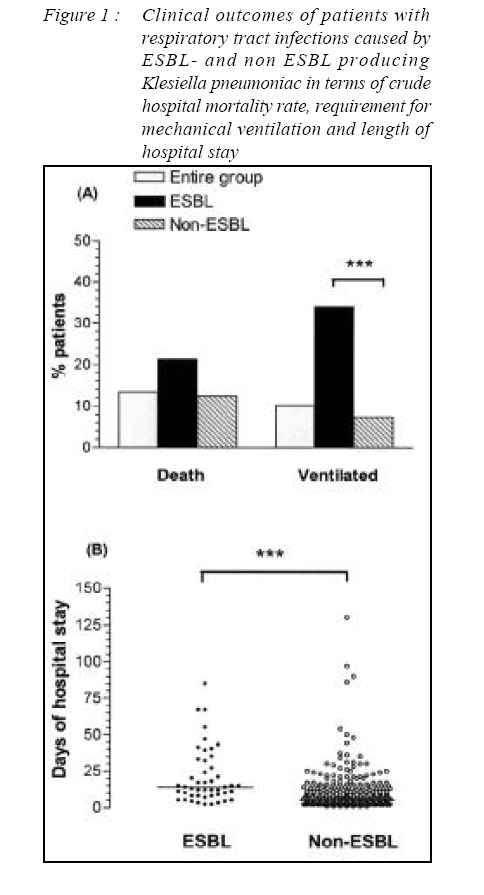
Seremban Hospital, Negeri Sembilan, Malaysia Submitted-20-02-2005, Accepted-03-12-06 Code Number: mj07023 Klebsiella pneumoniae ranks high as a cause of adult pneumonia requiring hospitalization in Malaysia. To study whether extended-spectrum b-lactamase (ESBL) producing K. pneumoniae was linked to hospital outcomes, we retrospectively studied 441 cases of adult respiratory tract infections with microbial proven K. pneumoniae from an urban-based university teaching hospital between 2003 and 2004. 47 (10.6%) cases had ESBL. Requirement for ventilation and median length of hospital stay, were greater in ‘ESBL’ than in ‘non-ESBL’ group [34% vs. 7.4%, p<0.001; 14 days vs. 5 days, p<0.001 respectively] but not crude hospital mortality rate [21.3% vs. 12.4%, p=0.092]. There was a four-fold increased risk of requiring ventilation [4.61 (2.72-7.85)] when ESBL was present. Our findings support the association of ESBL producing K. pneumoniae with adversed hospital outcomes and reiterate the need for vigilance on the part of treating clinicians. Key words : extended spectrum beta-lactamase, ESBL, Klebsiella pneumoniae, hospitalization, respiratory tract infections, mortality, Malaysia Introduction Klebsiella pneumoniae, the most clinically important of all Kebsiella species (1), ranks high as a cause of community-acquired pneumonia (CAP) in adult hospitalized patients in Malaysia (2,3,4). This appears unique as neighbouring countries in the region like Thailand (5) and Singapore (6) do not always share this finding. Extended-spectrum b-lactamases (ESBLs) is a problematic resistance mechanism that is commonly associated with K. pneumoniae. Since its first recognition in the United States in the 1980s, it is now reported worldwide (7) including in Malaysia (8). It poses important therapeutic dilemma in that most b-lactam stable antibiotics are ineffective towards ESBL producing organisms. Third-generation cephalosporins, in particular, have variable therapeutic efficacies (9) and are shown to have high propensity to induce the development of such resistance mechanism (10). Presence of ESBL producing K. pneumoniae infection has been shown to be associated with adverse clinical outcomes (11,12) and in the treatment of any pneumonia, appropriate choice of empiric antibiotics is important and has been shown to affect outcomes (13,14). In view of the prevalence of K. pneumoniae in hospitalized adult pneumonia cases in Malaysia and the lack of published data on the clinical impact of ESBL-producing K. pneumoniae in the context of respiratory tract infections, we carried out a retrospective observational study of patients with K. pneumoniae respiratory tract infections admitted to our university teaching hospital, to find out whether respiratory tract infections caused by ESBL producing K. pneumoniae affected clinical outcomes in terms of hospital mortality, requirement for mechanical ventilation and length of hospital stay. Methods & Patients Data collection Data on all respiratory specimens (i.e. sputum, tracheal aspirates, bronchial washing and bronchoalveolar lavage) that cultured K. pneumoniae between January 2003 and December 2004 from our 800-bed urban-based university teaching hospital and their patient details were downloaded from hospital computer. Medical records of these patients were then retrieved and reviewed for eligible cases. Included were adult patients (≥12 years of age) who received antibiotic treatment for respiratory tract infections diagnosed on clinical (plus or minus) radiological grounds and in whom respiratory isolates cultured K. pneumoniae. For the purpose of this study, we did not seek to make any distinction between community- and hospital-acquired cases. Data was collected using a standardized form and consisted of individual patient, clinicodemographic details, antibiotic in vitro susceptibility results, and clinical outcomes in terms of crude hospital mortality rate, requirement of mechanical ventilation and length of hospital stay. Co-morbidity scoring (15) was carried out by an investigator (LCL), without the knowledge of patient groups. The study protocol was approved by local university research and ethics committee (International Medical University Research and Ethics Committee, number 065/2004). Klebsiella Pneumoniae K. pneumoniae was identified by standard microbiological culture technique to the level of species. All enterobacteriaceae cultured were tested for susceptibility to a panel of 6 to 9 antibiotics prespecified by the Ministry of Health Malaysia (Personal communication, Hj Abd Jalil Mohd, Microbiology Unit), and tested for extendedspectrum b-lactamases, using a double-disc synergy test. Statistical analysis For analysis, patients were divided into two groups according to presence of ESBL. Differences between groups were assessed by Chi-Square tests for categorical, and t tests or Mann Whitney tests depending on the normality of continuous data. Odd ratios with 95% confidence interval were calculated to determine their relative risks. All computation was made using statistical package SPSS version 11.5 for Windows (Chicago, Illinois, USA). In all cases, statistical significance was defined at the 5% level and assessed based with two-tailed tests. Results Of the 441 eligible patients with documented respiratory tract infections and K. pneumoniae cultured from respiratory specimens, 47 (10.6%) had ESBL-producing strains. The clinico-demographic features are described in Table 1. Both groups were comparable except for type of respiratory specimens from which the organisms were isolated. The overall rates for hospital mortality and requirement for mechanical ventilation of patients with K. pneumoniae were 13.4% and 10.2%. The mortality rate during hospital stay of patients with ESBL and non-ESBL producing K. pneumoniae were 21.3% and 12.4% respectively (p=0.092). The percentage of patients requiring mechanical ventilation were 34% and 7.4% respectively (p<0.001). The median length of hospital stay in patients with and without ESBL producing K. pneumoniae were 14 (Interquartile range25-75, IQR25-75: 8-32) and 5 (IQR25-75: 3-10) days respectively (p<0.001) [Figure 1]. There was a four-fold increased risk of requiring ventilation [4.61 (2.727.85)] when ESBL was present. Discussion We have shown that in adult patients with respiratory tract infections ESBL producing K. pneumoniae, is associated with more adversed hospital outcomes in relation to the need for mechanical ventilation and having extended hospital stay when compared to non-ESBL. The association between ESBL producing K. pneumoniae and adversed clinical outcomes is well documented. In an international prospective study of 455 bacteraemic patients (16), Paterson et al showed that ESBL-producing K. pneumoniae was associated with high mortality with failure of correct antibiotics. In another recent study of 133 ESBL producing K. pneumoniae and Escherichia Coli bacteraemic patients (17), Kang CI et al showed that appropriate antibiotics, not necessarily those that were empirically instituted, was clinically important. In fact, they showed that delay in appropriate definitive antimicrobial therapy was not associated with higher mortality if antimicrobial therapy was adjusted appropriately according to the susceptibility results. However, very few studies to date have investigated clinical outcomes in the context of pneumonia. Our results add to the existing literature, the evidence of association between ESBLproducing organisms and adversed clinical outcomes in patients with pneumonia. Apart from the inherent weaknesses of a retrospective study, our study protocol had not included other clinical parameters (18), such as oxygenation status, blood urea, the presence of confusion, radiological extent of pneumonia, in the assessment of hospital clinical outcomes between ESBL and non-ESBL groups. Nevertheless, our data have taken into account the two key parameters of age and co-morbidity in severity assessment of any pneumonia. Furthermore while ESBL cases our overall sample size of K. pneumoniae cases is relatively large. Also it noteworthy, that our study did not make any distinction between pneumonia and respiratory tract infections because the retrospective nature of the study could not allow us to be confident in such distinction. We are however confident from our data that these were patients treated for respiratory tract infections. Another important concern is whether ESBLs isolated from tracheal aspirates included in our analysis would inherently bias the findings towards adversed hospital outcomes since they represent more critically ill patients on ventilators. In a separate further analysis using sputum cases alone, we could show that the findings were the same i.e. ESBL group had a significantly higher rate of mechanical ventilation (13.3% vs. 2.8%; p=0.03) and longer hospital stay (median days: 15 vs. 6; p<0.001). In view of this, we are confident that our conclusions have not been significantly altered by this factor. Although the prevalence of K. pneumoniae in clinical respiratory isolates of our hospital has increased over the years (unpublished data), the prevalence of ESBL producing K. pneumoniae remains low (<15%). In this study, about 10% of K. pneumoniae cases were ESBL producing. Such findings like ours provide local benchmark data for the country and the region. However the local epidemiology data are likely to vary from one setting to another. A study (18) of all 570 clinical isolates from four medical centres in Malaysia and two medical centres in Singapore showed a prevalence of ESBL producing K. pneumoniae of between 36.7% and 38%. It is obvious that continuing national and regional surveillance and research will be continually needed to monitor patterns in order to develop appropriate healthcare policies and control (19). Acknowledgements This study is funded by International Medical University internal research fund (IMU 065/2004). The authors wish to thank Mr Haji Abdul Latiff Mohamed, Senior Microbiologist, Microbiology Unit, Department of Pathology, Seremban Hospital, and staff in medical records of Seremban Hospital, for their kind assistance in retrieving the relevant data. Reference
© Copyright 2007 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj07023t1.jpg] [mj07023f1.jpg] |
| |||||||||

{kind=link}
{kind=link}