 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
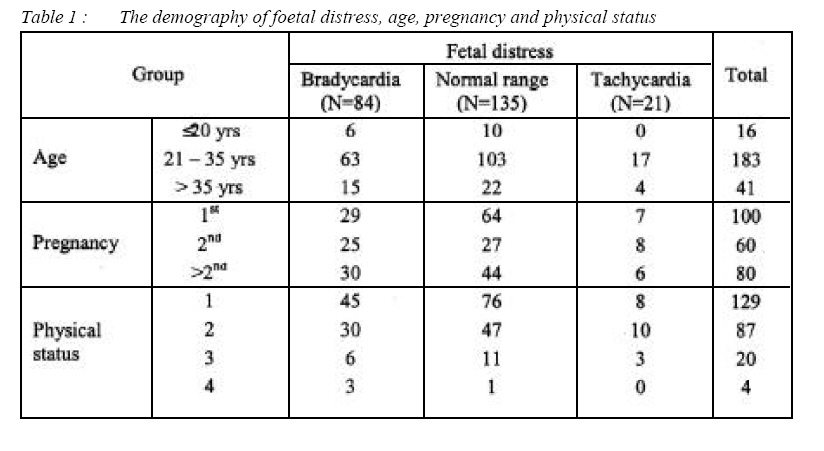
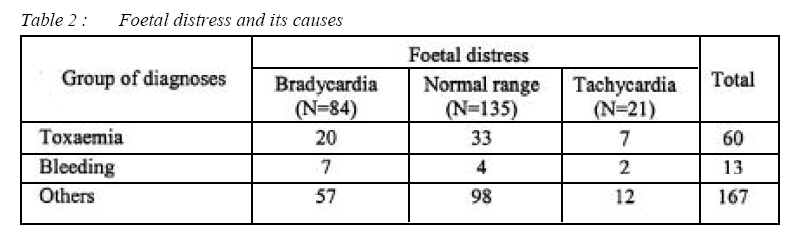
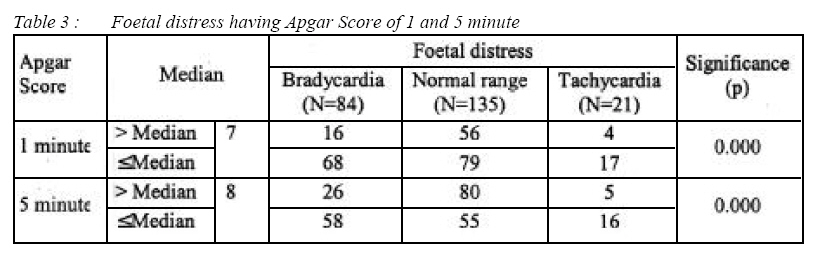
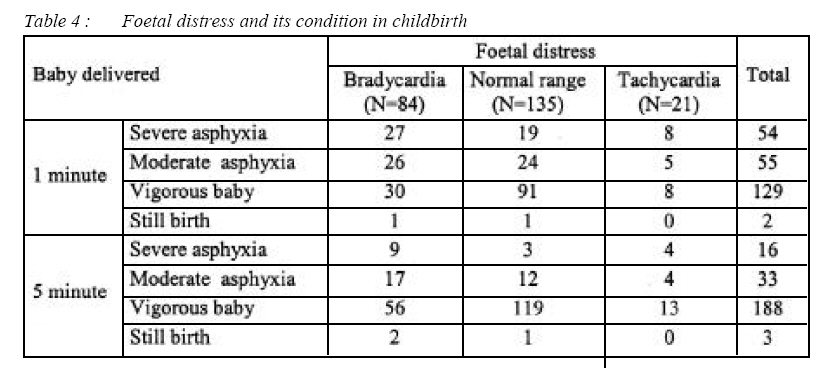
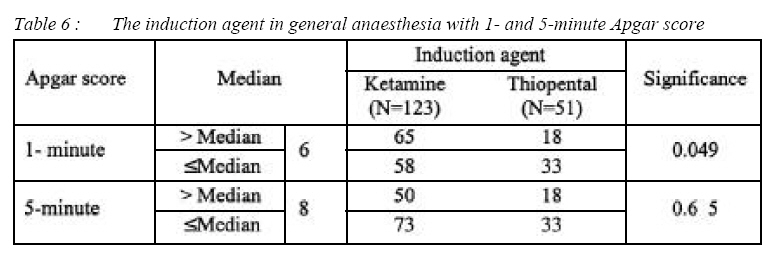
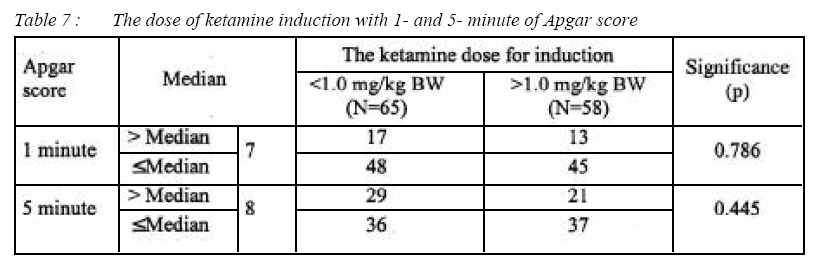
ORIGINAL ARTICLE Evaluation of Anaesthesia Methods in Caesarean Section for Foetal Distress Sri Wahjoeningsih & Widowati Witjaksono* Department of Anaesthesiology and Reanimation, School of Medicine, Airlangga University, Dr Soetomo Hospital, Jl. Prof. Dr. Moestopo no.47, Surabaya 60128, Indonesia Submitted-20-02-2005, Accepted-03-12-06 Code Number: mj07024 The purpose of this study was to evaluate the anaesthetic technique for Caesarean section which was appropriate for the clinical situation. This retrospective study was conducted on 240 patients undergoing Caesarean section with indications of foetal distress during a 3-year period (2002-2004). The data were reviewed from the patient’s medical record of the Department of Anesthesiology, Dr Soetomo Hospital, Surabaya. The patients were divided into three groups, according to the criteria of foetal heart rates. The success of the anaesthesia methods was determined by assessing the Apgar scores of the newborn baby. The results were analyse using Kruskal-Wallis and Chi-Square test. P ≤0.05 was considered as statistically significant. 1- and 5-minute Apgar score of the normal range group was significantly higher than that of the bradycardia group (p<0.05), but no significant differences was found between the normal range and the tachycardia group (p>0.05). Oneand five- minute Apgar scores of the sub-arachnoid block group were significantly higher than those of the general anesthesia group (p<0.05). One-minute Apgar score of the ketamine group was significantly higher than that of the thiopental group (p<0.05), but no significant differences in 5-minute Apgar score was found between the ketamine and the thiopental groups (p>0.05). We conclude that subarachnoid block is the choice of anaesthesia for patients undergoing Caesarean section for foetal distress’s diagnosed at PS 1 and 2 patients. General anaesthesia with ketamine Apgar score at one minute better than that of the thiopental. Key words : Obstetric anaesthesia, foetal distress, Caesarean section, emergency Introduction Obstetric anaesthesia differs from surgical anaesthesia because the patient may require hospitalization at any time, day or night and the time for preparation of surgery and anaesthesia may extend from hours to just a few minutes to save two lives, the mother and the unborn baby. The condition of both should be monitored carefully. Foetal distress is one of the indications to fasten the delivery process. The diagnosis of foetal distress is based on the foetal heart beats, whether they are fast, slow, irregular and whether there is meconium present during delivery (1). Foetal distress is present if the foetal heart rate is more than 160 beats per minute, below 100 beats per minute, or if has there is irregular heart rhythm (2). Foetal distress occurs in uteroplacental dysfunction as well as in maternal foetal and obstetric complications. Asphyxia may occured either antepartum or intrapartum, when there is transient decrease in uterine blood flow accompanying each uterine contraction. Contractions decrease uterine blood flow and placental perfusion by means of external compression on uterine vascular bed. Borderline function of the placenta may be unable huider provision of adequate gas exchange during labour, because the presence of contractions decreases gas exchange. Foetal monitoring can effectively predict and diagnose foetal asphyxia during pregnancy and labour (3, 4). The Apgar score continued to be is widely used to assess newborns, although its value has been questioned repeatedly. The Apgar score system at 1 minute and 5 minute is in common use and gives information about the severity and prognosis of asphyxia. The 1-minute score correlates with survival, while the 5 minute score is related to neurologic outcome (1). The success of obstetric anaesthesia can be seen gauged through the baby’s Apgar score. Caesarean delivery is indicated in the presence of foetal distress for several reasons, as follow; failure of labour which progressed to cephalopelvic disproportion; malpresentation; deteriorating foetal status; non reassuring foetal heart rate; and maternal decompensation, haemorrhage, worsening preeclampsia/eclampsia (2). Classification of urgency Caesarian section is that proposed by Lucas (5). Category 1 Caesarean sections, are those where there is an immediate threat to the life of the mother or foetus, due to prolapsed cord, bleeding placenta previa, abruptions placenta with a life foetus, dire fixed foetal bradycardia and failed vaginal delivery. This may still allow time for the performance of regional block. An expert may be able to perform a spinal anaesthetic or top up an epidural anaesthesia within 15 minutes, but not to establish a new epidural anaesthetic. For category 2 Caesarian sections, where there is a threat to the mother or baby, but it is not immediate, there is usually time for regional block except in the most difficult of women. For categories 3 and 4, there are no time pressures on the choice of anaesthesia. Before the balance between technique and urgency can be successfully managed, it is important to have a good understanding of what regional anaesthesia must achieve. When choosing regional or general anaesthesia for Caesarean delivery, one must consider outcome of both the mother and the neonate. Maternal outcome studies have primarily focused on maternal mortality, and neonatal outcome studies have focused on umbilical cord pH, Apgar score, the need for ventilatory assistance at birth and neurobehavioral score. Regional anaesthesia is the preferred method for caesarean section in healthy women, however general anaesthesia is still necessary in selected cases. The frequency of general anaesthesia use is depend able on many factors which include the percentage of parturient who receive epidural analgesia, the percentage of highrisk parturient, and the skills of the managing anaesthesiologist. The choice of anaesthetic technique and the method of delivery must be appropriate to the clinical situation. If time is the limiting factor, sometimes general anaesthesia is necessary because it offer rapid induction, reliability, controllability, reproducibility, and avoidance of sympathectomy-induced hypotension. The morbidity and mortality associated with general anaesthesia, are in relation, pulmonary aspiration of gastric contents and difficulties with tracheal intubation. This has led to a perception that anaesthetic risk is greater with general than regional the anaesthesia (1, 6). The baby can be affected directly by transplacental drug transfer or indirectly by alteration of foetal-placental perfusion, or both. The risks of direct effects from placenta transfer are greatest with general anaesthesia, because maternal drug exposure is greater, but it might also occur with epidural anaesthesia, particularly when a preexisting labour epidural catheter is topped up for caesarean delivery (1). The purpose of this study is to evaluate the choices of anaesthetic technique for Caesarean Section in accordance with patients clinical conditions. Materials and Methods This survey was a retrospective study performed on 240 patients having Caesarean section for foetal distress undertaken in Dr Soetomo Hospital at Surabaya in the period of 2002-2004 (3 years). The medical record’s were reexamine and the patients’diagnoses, the choice of anaesthesia, the ASA physical status of the patients, medical induction, and the babys, Apgar scores were recorded. Anaesthesia was performed by a resident anaesthetist under supervision from the anaesthetic consultant of the anaesthesiology department. Patients were divided into three groups accordingly to the criteria of the number of the foetal heart beats: The first group was bradycardia group (n = 84) whereby the foetal heart beats were less or equal to 100/min, the second group normal group ( n = 135 ) was one having normal threshold of foetal irregular heart beats, it was 101 – 160/min and/or accompanied by a divergence in the NST picture, and the third group was tachycardia group ( n = 21 ) having more than 161/min of foetal heart beats. The statistical analyses obtained was based on the Kruskal-Wallis, Chi-Square and median tests. The difference was considered as significant if the p value was ≤0 05. Results The demographical characteristics of the 240 patients who underwent having Caesar an section as a result a diagnosis foetal distress is shown in Table 1. In 76.25% g th patients of were between 21 and 35 years of age, while 17.08% of the patients were more the of 35 years old. Patients 53.7%, physical status of ASA 1, 36.25% patients had ASA 2 physical status. While 41.67% of the patients were primigrarid while 25.00% of the patients were intheir second pregnancy. A diagnosis of foetal distress due to toxaemia cousitited 25.00% of patients while those with bleeding conotituted only 7. 08% (Table 2). The Apgar score of 1 - 5 minutes was of group having heart beats significantly higher than normal threshold (p<0.05) compared to the group of bradycardia. In groups of normal threshold there was not any significant difference of Apgar score of 1 5 minutes (p>0.05) to tachycardi group (Table 3). 22.50% of babies having 1 minute Apgar Score and delivered through Caesarian section of with fetal distress diagnose would suffer from serious or severe asphyxia and after resucitation was undertaken, the percentage decreased to 6.67% and only one (1) baby (0.42%) died (Table 4). The analyses result as seen on Table 5 shown that 1 and 5 minute Apgar score of the group of subarachnoid block was significantly higher compared (p<0.05) to that of the group of general anesthesia. The use of ketamine or thiopental induction on 1-minute Apgar score showed that there was significant difference (p<0.05), while on 5-minute Apgar score there was not any significant difference (p>0.05) (See Table 6). The use of ketamine dose of less than 1 mg/ kg bodyweight and more than 1 mg/kg BW in fact, did not show any significant difference (p>0.05) towards the Apgar score (Table 7). The average dose of <1.0 mg/kg BW was 0.90 (±0.13) mg/kgBB, and one of >1.0 mg/kgBB was 1.17 (±0.10) mg/kg BW. Discussion The management of foetal distress is one of the challenging tasks for both the obstetrician and anaesthesiologist. The consequences of unrecognized or poorly managed perinatal emergencies can be devastating, ranging from neurologic impairment to intrauterine foetal death. Perinatal asphyxia at term remains a significant cause of infant death and development impairment. The choice of anaesthesia in these critical situations consist of general anaesthesia with rapid-sequence induction. The latest recommendation of the German Society for Gynacology and Obstetrics demands 20 minute time frame for decision-to-delivery time (1). Sub arachnoid block was done on 27.5% of total patients having Caesarean section with the diagnosis of foetal distress, 96.96% patients of PS 1 and 2 out of sub arachnoid block done. The Apgar score at 1 minute was 50.00% above the median, while at 5 minutes was 65.15% above the median. The Apgar score at 1 minute and 5 minutes were significantly higher compared to those of general anaesthesia (p<0.05). Patients having toxaemia of pregriang have decreased uteroplacental perfusion, resulting foetal asphyxia that worse the condition of the delivered baby. A hypertensive mother already has divergence in the circulation to placenta affecting the flow to uterus, so this condition would also affect the foetal condition. The presence of limited function of perinatal placenta will cause disability to keep the gas exchange of foetal asphyxia (1). A third (33.33%) of the total foetus in womb suffered from bradycardia and 11.67% suffered from tachycardia. Babies born with severe asphyxia were 38.33%, stillborn 1.6% (1 baby) and after resucitation the 5minute Apgar score showed improvement that only 10% of the baby still remained in severe asphyxia. Bleeding causing hypotension would decrease cardiac output leading to reduced uterine blood flow. This change will affect the process of oxygenation of the fetus. In this research, it was found that the fetus having bradycardia was 53.85% and having tachycardia was 15.38%. Babies delivered by bleeding mothers were 53.85%, having severe asphyxia and after resucitation the 5-minute Apgar score was still 23.08% having severe asphyxia. Fifty one (21.25%) of patients were given thiopental induction of 3.80 (±0.99)mg/kg BW dose. The preferred dose of thiopental was 4 mg/kg BW. The thiopental was both negative inotrope and vasodilator, however, this dose was unlikely to have an adverse hemodynamic effect on the normal pregnancy. The dose may result in significant decline in cardiac output and blood pressure in hypovolemic patients (7, 8). Thiopental appeared in the foetal blood within 45 seconds after administration into the mother with peaking level at most within 3 minutes. The Apgar score of new born babies (neonates) which is induced by 1 mg/kg BW ketamine was similar with the Apgar score of neonates which is induced by thiopental 3mg/kg BW.(1) Ketamine was induced on 123 (54.17%) patients having Caesarean section with fetal distres diagnose. The dose used was 1.47 (±0.50) mg/kg BW. Ketamine dose greater than 2 mg/kg is associated with neonatal depression (1). The regular dose suggested was 1.0 mg/kg BW but it had analgesic and hypnosis effects and still cause amnesia. In this research, there was significant difference (p<0,50) on 1-minute Apgar score between ketamine and thiopental inductions (Table 6). Patients having ketamine induction, 52.85% of those had 1-minute Apgar score above median, and those having thiopental induction were only 35.29% on babies delivered above the median. Ketamine was excellent in cases of severe fetal distress; 100% of oxygen can be administrated until delivery with low risk of maternal awareness and recall. The clinical study has already suggested to use the ketamine, with decrease incidence of maternal awareness when compared with administration of thiopental as single agent or combination of smaller doses of thiopental and ketamine. Ketamine rapidly croses the placenta, and reached its peak on fetus about 1.5 to 2.0 minutes after the induction (7, 8). In this research, it was found that the induction time of birth in ketamine induction was 6.35 (±2.89) minute while that of the thiopental was 7.39 (±2,91) minute. Chestnut (5) performed an observation at the umbilical cord, the blood gases and the pH of the same Apgar score after ketamine and thiopental inductions on the Caesarean section compared general anesthesia. He found that 1 mg/kg BW of ketamine induction for the Caesarean section would a higher neuro behaviour scoreof the baby compared to thiopental induction. The results obtained in this research supports the view that the ketamine is the most powerful induction medicine in obstetric anesthesia (5). It can be concluded from the research result that: 1) Subarachnoid block to the first choice of anaesthesia for patients undergoning Caesarean section due to fetal distress, it should be done on patients with plugsical status 1 and 2 because it produces better Apgar score of 1 and 5 minutes compared to general anesthesia; and 2) General anesthesia with ketamine induction in Caesarean sections due to foetal distress gives better Apgar score of 1 minute compared to that of the thiopental induction. Based on the explanation above, these suggestions should be recommended: 1) Many factors that causing foetal distress should be considered to determine the right way and the best choice of anaesthesia during Caesarian section 2) Preparation on the patients undergone Caesarian section should not be done only for the mothers but also for the foetus covering foetal resuscitation, adequate infusign, oxygenation and setting position to reduce pressure on vena cava inferior 3) The problems that can arise during general anaesthesia for Caesarian section should be anticipated before intervention prevent immediately if something happened 4) It needs the full cooperation of interdepartmental team work to manage critical condition in order to gain maximum result. References
© Copyright 2007 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj07024t1.jpg] [mj07024t6.jpg] [mj07024t3.jpg] [mj07024t2.jpg] [mj07024t7.jpg] [mj07024t5.jpg] [mj07024t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}