 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
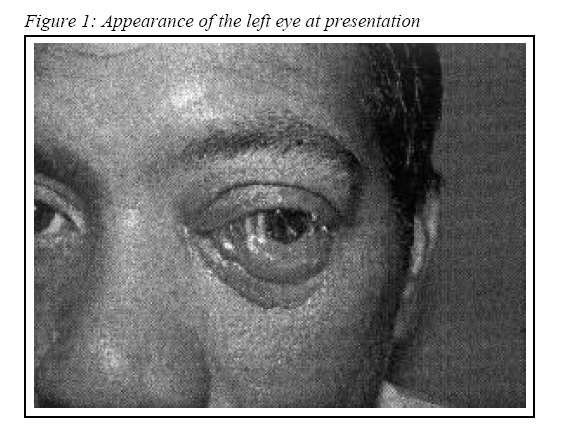
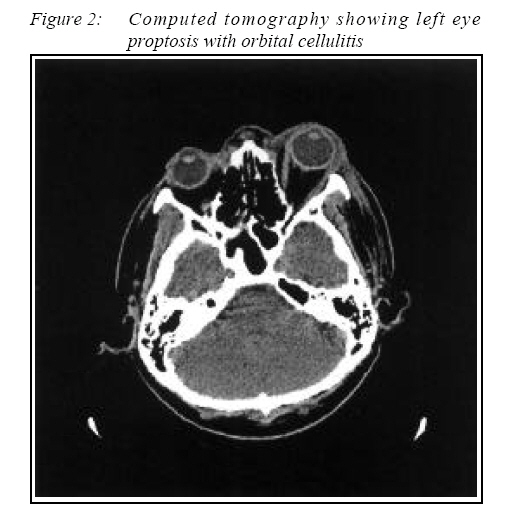
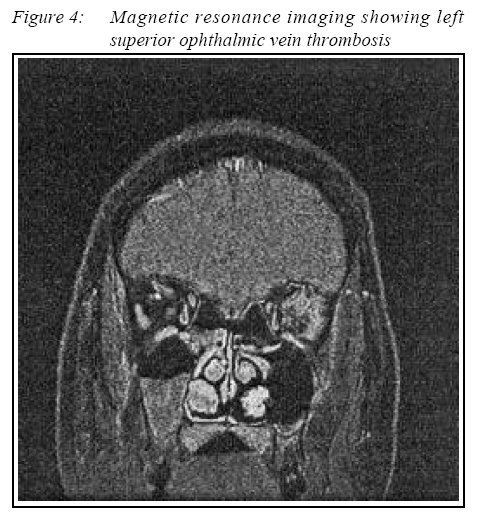
CASE REPORT Dental Infection Presenting with Ipsilateral Parapharyngeal Abscess and Contralateral Orbital Cellulitis – A Case Report Zunaina Embong, Shatriah Ismail, Asokumaran Thanaraj, Adil Hussein Department of Ophthalmology, School of Medical Sciences, Universiti Sains Malaysia, Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Submitted-20-02-2005, Accepted-03-12-06 Code Number: mj07028 A 43 year-old man presented with pain on the right tooth for three days duration. Computed tomography showed left orbital cellulitis and right parapharyngeal abscess. There was also evidence suggestive of a dental abscess over right upper alveolar region. Magnetic resonance imaging revealed left superior ophthalmic vein thrombosis. Emergency drainage of the right parapharyngeal abscess was performed. Right maxillary molar extraction revealed periapical abscess. Left eye proptosis markedly reduced after initiating heparin. Key words : Maxillary molar abscess, cavernous sinus thrombosis, superior ophthalmic vein thrombosis. Introduction Dental infection may cause sinusitis, orbital cellulitis, parapharyngeal abscess, mediastinitis and pericarditis (1, 2). However, maxillary molar abscess with contralateral orbital cellulitis and superior ophthalmic vein thrombosis is an unusual presentation. Case Report A 43 year-old Malay man presented with a history of pain on his right tooth for three days duration. He also experienced pain over the right jaw which was associated with low-grade fever. However, he reported no facial pain or pain over the maxillary region. Two days after having right toothache, he developed a left orbital swelling, which was progressively increase in size and associated with pain. The left eye was red with marked tearing. The vision of the left eye was progressively getting worse. The left orbital swelling was not associated with discharge, difficulty in swallowing, neck pain or fits. There was no history of trauma and no significant past medical or surgical history. Eye examination showed visual acuity in the right eye was 6/6. Visual acuity in the left eye was perception to light. There was relative afferent pupillary defect in the left eye. The left eyelid was swollen and partially covered the eye. There was 6 mm proptosis of the left eye with no obvious mass of the orbit seen. The conjunctiva was chemotic and injected with clear cornea (Figure 1). The eye was warm and tender. The proptosed eye was nonpulsatile and elicited no bruit. There was painful ophthalmoplegia. The anterior chamber examination was normal and the intraocular pressure had increased to 29mm Hg. Fundoscopy showed choroidal striae at the posterior pole with normal pink disc. The retinal vessels were normal. The right eye was normal and not proptosed. The anterior segment and the fundus were also normal. Maxillary and frontal area was normal and non-tender. General examination revealed an illlooking patient who was afebrile with stable vital signs. However, he was conscious and alert. There was no neck stiffness or weakness of both upper and lower limbs. Systemic examination was unremarkable. Diagnosis and Treatment A diagnosis of left eye orbital cellulitis was made. The patient was immediately started on intravenous ceftazidime one gram 12 hourly and intravenous vancomycin one gram 12 hourly after taking blood for culture and sensitivity. Guttae ciprofloxacin every 2 hourly and topical timolol 0.5% every 12 hourly was instilled to the left eye. Urgent computed tomography finding was compatible with left orbital cellulitis (Figure 2) and revealed right parapharyngeal abscess (Figure 3). There was also evidence suggestive of tooth abscess over right upper alveolar region with bilateral maxillary and posterior ethmoidal sinusitis. However, the cavernous sinus area was not clearly visible. An emergency drainage of the right parapharyngeal abscess and bilateral antral washout was performed by an otorhinolaryngologist. Right maxillary molar extraction was done by the dental team revealing a periapical abscess. Culture from the drainage and blood showed scanty mixed growth. Intravenous metronidazole 500mg was subsequently added to give a better coverage of the anaerobes. Magnetic resonance imaging revealed cavernous sinus thrombosis with left superior ophthalmic vein thrombosis (Figure 4). The patient was then started on subcutaneous heparin 5000 unit 12 hourly after reviewed by a neurologist. Two days after initiating heparin, the proptosis was markedly reduced with regression of the lid oedema. However, the visual acuity has not improved. Patient was discharged after having completed two weeks of intravenous antibiotics and was placed on long-term warfarin for one year. Discussion Infection of maxillary molar may become lifethreatening through airway compromise or threatened vision by rapid spread involving the orbital area. Parapharyngeal space is a critical area in the neck which may be easily infected by a dental infection (3, 4). Infection of the maxillary molar may spread through local tissue planes or venous channel to involve parapharyngeal space; resulting in the development of a parapharyngeal abscess. A dangerous complication of parapharyngeal abscess includes airway obstruction due to medial bulging of the pharyngeal wall and supraglottic oedema. Other complications of maxillary molar infection include maxillary sinusitis, pansinusitis, orbital cellulitis, and cavernous sinus thrombosis (5, 6). Maxillary sinusitis may result from extension of maxillary molar infection or from perforation of the sinus floor during extraction of diseased maxillary teeth (6). This is because the root of the molar teeth in the upper jaw lies close to the floor of the maxillary antrum and may even protrude into it. Maxillary sinusitis may lead to cavernous sinus thrombosis (7) via thrombophlebitis of infraorbital vein. Dental infection is a well-reported cause of cavernous sinus thrombosis and it is believed that the most frequent route of spread is through the pterygoid plexus (4). Cavernous sinus thrombosis also can occur following acute ethmoiditis (7, 8). The spread of infection through valveless superior ophthalmic vein reaches the cavernous sinus (9). Involvement of the contralateral eye, indicates spread from the original side of infection through the intercavernous sinuses to the opposite cavernous sinus (7, 8, 10). The infection presumably gained access to the contralateral eye through valveless venous channels in a retrograde fashion. Other possible explanation for the presentation of contralateral orbital cellulitis in this patient is that the infection may spread from the ethmoidal sinus since this patient has bilateral ethmoidal sinusitis. Orbital complications are usually secondary to ethmoiditis (8, 11, 12) especially in children (13). Reddy reported that orbital cellulitis secondary to ethmoiditis in 25%, maxillary sinusitis in 10% and ethmoid and maxillary sinusitis in 30% of patient (10). The thin lamina papyracea divides the orbit from the ethmoidal sinus and permits infection to spread with relative ease. Infection may erode through the bone or pass through the numerous small valveless veins that perforate the bone (10, 12). Superior ophthalmic vein thrombosis is generally noted as a thickening of the superior ophthalmic vein as compared with the contralateral normal side. Thickening of the superior ophthalmic vein should be looked for as an important radiological marker of impending orbital complications (9). Orbital cellulitis can lead to serious complication include blindness, intracranial complications (1, 9, 10), and death (4). Optic nerve damage can occur either due to vascular compromise to the optic nerve, compressive optic neuropathy or due to inflammatory optic neuropathy (12). The most common bacteria isolated in orbital infection is Staphylococcus aureus (10, 14) and Streptococcus pneumoniae (14). Haemophilus influenza is a very commonly isolated pathogen in children (15). Streptococcus anginosus was reported as one of the virulent pathogens that cause necrotising orbital cellulitis (16). Bacteroides melaninogenicus is a pathogen implicated in neck abscess of dental origin (6). There was no organism isolated in this patient. One possible explanation is that the patient was started on antibiotics by the primary physicians before initial referral (13). Computed tomography is the diagnostic modality of choice for demonstrating cavernous sinus thrombosis. However, even with intravenous contrast, computed tomography often fails to demonstrate occlusion of the cavernous sinus (8). Magnetic resonance venogram, using presaturation to eliminate arterial signal is a more sensitive method for revealing cavernous sinus thrombosis (17). Optimal therapy for septic cavernous sinus thrombosis may include antibiotics, anticoagulant, corticosteroids and surgery. In general, a penicillinase-resistent penicillin, often with a third generation cephalosporin, is appropriate empiric therapy. Metronidazole may be added to the regime to optimize anaerobic coverage, especially when the process originates from a dental or otorhinologic process. When there is rapid progression of septic cavernous sinus thrombosis, initial therapy including vancomycin should be immediately administered (8). Early anticoagulant therapy was shown to reduce morbidity although there was no conclusive evidence for reduction in mortality (18). Anticoagulant therapy may prevent thrombus propagation, thereby enhancing antibiotic access to the septic thrombus, and may prevent thrombus extension, which leads to dural venous infarction and enhance recanalization through the thrombus (18). Therapy in this patient includes appropriate antibiotic coverage, drainage of parapharyngeal abscess and maxillary sinuses, extraction of infected teeth and administration of long-term anticoagulant. Conclusion Early identification of dental infection is necessary in order to avoid life-threatening and vision-threatening complications. Prompt treatment with heparin is critical in the management of superior ophthalmic vein thrombosis. Acknowledgement I am grateful thanks to Professor Jafri Malin Dato’ Abdullah, Head, Department of Neurosciences, USM, Malaysia, Dr. Dennis Lowe, Ophthalmic Surgeon & Consultant Neurologist, University of Sydney, Australia, Mr. Baharuddin Abdullah, Department of Otorhinolaryngology – Head & Neck Surgery, USM, Malaysia and Mr. Abdullah Pohchi, Maxillofacial Unit, USM, Malaysia for their contribution in the management of this patient. References
© Copyright 2007 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj07028f4.jpg] [mj07028f1.jpg] [mj07028f3.jpg] [mj07028f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}