 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 15, No. 1, Jan 2008, pp. 23-30 ORIGINAL ARTICLE Histopathological Studies of Cardiac Lesions After an Acute High Dose Administration of Methamphetamine Arthur Kong Sn Molh, Lai Chin Ting, Jesmine Khan, Al-Jashamy K*, Hasnan Jaafar*, Mohammed Nasimul Islam School of Health Sciences, *School of Medical Science, Universiti Sains Malaysia, Health Campus,
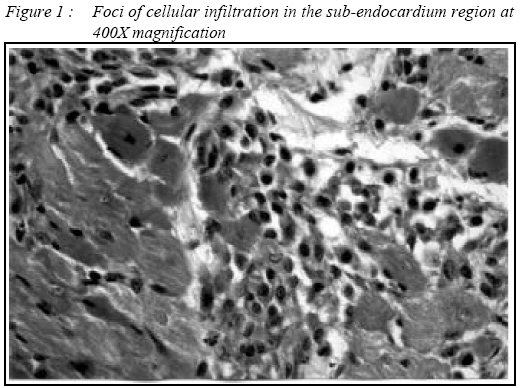
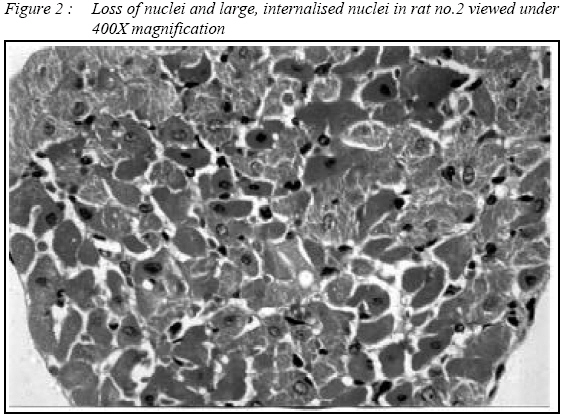
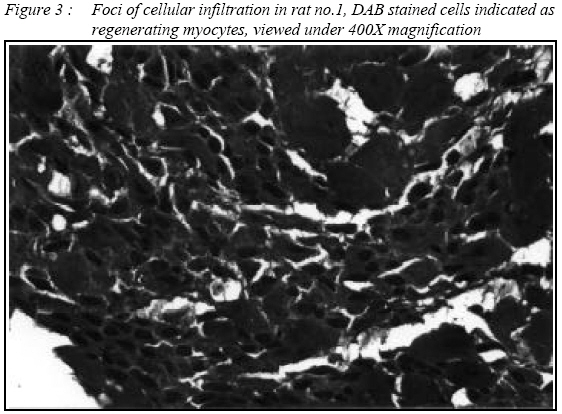
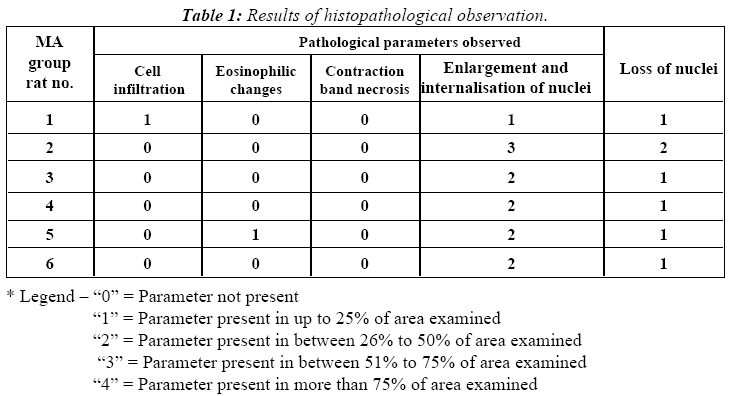
16150 Kubang Kerian, Kelantan, Malaysia Submitted-20-02-2007, Accepted-03-12-07 Code Number: mj08004 Eighteen male Wistar rats aged six weeks were divided equally into Methamphetamine (MA), Placebo and Control group. MA group were injected with 50mg/kg body weight of Methamphetamine hydrochloride (MAHCl) in normal saline, Placebo group were injected with normal saline only, while Control group not injected with anything. Five MA group rats died within four hours of injection and their hearts collected on the same day. Another MA group rat was sacrificed two days after injection. Placebo and control group were sacrificed at similar intervals. Collected hearts were studied for cardiac lesions under light microscopy using special staining and immunohistochemistry. Microscopic examination of the myocardium of the rats that died on the first day of injection showed loss of nuclei in some myocytes, indicating cell death. Some areas in the sub-endocardium region showed internalization and enlargement of myocyte nuclei, consistent with regeneration of cells. There were very few foci of necrosis observed in these samples. The heart samples from the single rat that survived injection for two days showed foci of infiltration of macrophage-like cells that were later revealed to be regenerating myocytes. There were also spindle-like fibroblasts, macrophages and a few leucocytes found within these foci. The overall appearance of the myocardium did not indicate any inflammatory response, and the expected signs of necrosis were not observed. These results suggest a need to re-evaluate the toxic and lethal dosages of MA for use in animals testing. Cause of death was suspected to be due to failure of other major organs from acute administration of MA. Death occurred within a time period where significant changes due to necrosis may not be evident in the myocardium. Further investigations of other organs are necessary to help detect death due to acute dosage of MA. Key words : MA, acute dose administration, cardiac lesions, myocardium. Introduction The use of MA along with other “designer” drugs have seen a dramatic increase beginning from the 1990s, as more drug abusers seek cheaper, more potent alternatives to the “traditional” stimulants such as cocaine (1–3). The stimulant and euphoric effect of MA is similar to cocaine, bringing about similar behaviour in animal tests of MA and cocaine. MA in the form of hydrochloride crystals are volatile and smokeable, bringing an immediate euphoria that lasts longer than cocaine (1, 4). Cardiovascular symptoms related to MA toxicity include chest pain, palpitations, dyspnoea, hypertension, tachycardia, atrial and ventricular arrhythmias, and myocardial ischaemia (1, 4–9). MA abusers often go through a repeated pattern of frequent drug administrations (binge) followed by a period of abstinence. This pattern of chronic MA abuse can significantly alter cardiovascular function and cardiovascular reflex function and produce serious cardiac pathology (10). However, tachyphylaxis occurs with MA abuse, with long-term abusers being able to tolerate higher doses with fewer symptoms. MA has been known to cause death at an ingested dose as low as 1.5 mg per kg body weight, while long-time abusers developing drug tolerance may use as much as 5,000 to 15,000 mg per day (1). MA sold in the streets is usually mixed with other stimulants such as cocaine, phenypropanolamine hydrochloride, Damphetamine, ephedrine, or pseudoephedrine, and also with other adulterants such as lead, caffeine and baking soda (1). This discrepancy in the purity of MA available leads to the question whether the abuser may be taking high dosages far too toxic to the body, which may result in sudden death of the abusers. Given the pattern of MA abuse, previous studies have focused largely upon the chronic effect of MA intake to major organs, such as the brains and the heart, by using animal testing (6, 9, 11–13). However, there is a lack of research into the effects of acute dose intake of MA, especially pertaining to the heart. Sudden death due to acute MA intoxication has been suggested to be similar to acute myocardial infarction, where pathological changes to the myocardium generally are hard to detect, even under light microscopy (14). Thus, there is a need to review the effects of acute dosages of MA intake to the heart through microscopic studies in rats, which can help medical examiners differentiate myocardium changes due to acute MA intake from those of other cardiovascular diseases. Materials and Methods Eighteen male Wistar rats aged of six weeks were reared in the animal house of Universiti Sains Malaysia, Kubang Kerian, Kelantan under standard atmospheric conditions in three 12 (w) X 24 (l) X 8 (h) inch cage. Each cage was labelled according to the three groups the rats were divided into, namely the Control, Placebo, and MA injected groups. The weight of the rats ranged from 102.6 – 123.1 grams. Control Group The six rats in this group were kept under normal rearing condition, fed with standard laboratory chow and tap water ad libitum until six weeks of age. The rats were fasted for 24 hours before being sacrificed according to similar time intervals as the MA-injected group, and their hearts were collected. Placebo Group The six rats in this group were kept under normal rearing condition, fed with standard laboratory chow and tap water ad libitum until six weeks of age. Each rat was then injected intraperitoneally with 0.3ml of 0.9% (w/v) saline each. The rats were then fasted for 24 hours after injection before being sacrificed at similar time intervals as the MA-injected group and their hearts were collected. MA Injected Group The six rats in this group were kept under normal rearing condition, fed with standard laboratory chow and tap water ad libitum until six weeks of age. Each rat was then given an intraperitoneal injection of MAHCl dissolved in 0.9% (w/v) saline, the volume of which was adjusted according to body weight so that the final dosage received by each rat was approximately 50mg/kg. The rats were fasted for 24 hours before being sacrificed and their hearts collected for pathological observation. A total amount of 50 milligrams MAHCl used in this experiment was obtained from the Department of Chemistry Malaysia (JKM), Petaling Jaya, as MAHCl is a restricted substance classified under Section 39 (B) of the Dangerous Drugs Act 1952 in Malaysia, whereby possession, import or sale of the substance is strictly prohibited and punishable by Malaysian law. Moreover, this is an export forbidden item. As such, only the JKM is authorized by the Malaysian government to provide chemicals classified as restricted substance under Malaysian law for use in laboratory and scientific studies. The purity of the MAHCl obtained has been assayed and certified as to be of a minimum 99% pure, as stated in the certification report provided by the JKM. The dosage of MA given was calculated based on previous studies (15) so as to induce observable effects on the rats and to let the rats survive for at least 24 hours after injection. However, rats No.3, 4, 5, and 6 of MA group died after two hours of injection while rat No.2 died four hours after injection. The hearts of these rats were collected on the same day. Rat No.1 survived for 48 hours after injection before being sacrificed. The rats in the Control and Placebo groups were also sacrificed at similar intervals as the deaths that occur in the MA injected group rats. The rats were sacrificed by confining them in a glass chamber saturated with chloroform (except the rats from the MA injected group that died a few hours after injection). A small sample of the free upper left ventricle walls from each heart was taken and preserved in 0.9% (w/v) saline for future use in electron microscopy methods. A section of the upper levels of both ventricles from each heart were collected and preserved in 10% (w/v) formalin for paraffin embedding while the adjoining section was harvested for frozen sectioning. The sections of ventricles preserved in 10% (w/v) formalin were then processed in a tissue processor and embedded in standard paraffin blocks. The frozen sectioned ventricle samples were stained with Hematoxylin and Eosin (H&E) stain (commercial kit from Sigma Aldrich) for observation under light microscopy. The consecutive sections of paraffin embedded samples were stained using H&E, Masson’s Trichrome Stain (MTS) (commercial kit from Sigma Aldrich) and immunohistochemistry staining using rabbit anti-myosin (commercial kit from Calbiochem). For immunohistochemistry, the heart samples were treated with rabbit anti-myosin as the primary antibody, which was then reacted with biotinylated anti-rabbit immunoglobulin G (IgG) secondary antibody. Biotinylated horseradish peroxidise, avidin dehydrogenase, and hydrogen peroxide were then used to provide sites for binding of diaminobenzidine tetrahydrochloride (DAB) dye to the myosin molecules, and the nuclei of cells in the samples were counter-stained with Harris Hematoxylin. Any loss of staining of tissue using immunohistochemistry would indicate injury due to myocardial infarcts (16). The procedures for staining were sourced from the manuals of the commercial kits for each stain. The light microscopy assessments of the samples were conducted blindly by two observers to observe pathological changes highlighted in previous studies. Findings were confirmed while excluding artefacts through comparison with histochemical slides. The parameters observed for included eosinophilic changes, cellular infiltration, and contraction band necrosis. Comparison of H&E and immunohistochemistry results were used to assess distribution of myoglobin, while MTS was used to confirm any signs of fibrosis. The parameters of pathological changes observed were tabulated and graded using a scale of 0–4, where “0” signifies the absence of the parameters in the samples, or healthy myocardium; “1” indicating observed presence and distribution of the parameter up to 25% of the area examined; “2” indicating observed presence and distribution of the parameter between 26% to 50% of the area examined; “3” indicating observed presence and distribution of the parameter between 51% to 75% of the area examined; and “4” indicating observed presence and distribution of the parameter in more than 75% of the area examined. The Kruskall-Wallis test was used for statistical analysis in the SPSS version 11.5 software and a P value of <0.05 was considered significant. Procedure Fifty milligrams of MAHCl was dissolved in 2.5ml 0.9% (w/v) saline for the injection of the test group rats. The volume of MA infused saline injected into each rat was adjusted with the calculated concentration of MAHCl injected for each rat to be approximately 50 mg/kg body wt. Results Rat no.1 was injected with MAHCl earlier to observe the effect of the concentration of MA and the acceptability of the dose. This rat was subsequently sacrificed, 48 hours after the injection. The other rats were all injected with methamphetamine a day later. Rats no.3, 4, 5, and 6, died within two hours of injection, while rat no.2 died after four hours of injection. The hearts of these rats were collected on the same day after injection. Gross The hearts of the MA-injected rats were normal in size, without any signs of necrosis throughout the musculature. The hearts of the rats that died within 4 hours of injection were congested. The heart weight to body weight ratios were similar in all three groups. The hearts of the MA-injected rats had patent coronary arteries that were free of atheroma and their heart valves were normal. Light microscopy examination Hematoxylin and Eosin Staining (H&E) The sample from rat No.1 of MA group, which survived for 48 hours, displayed distinct foci of cellular infiltration (Figure 1), with clusters of macrophage-like cells having large nuclei and little cytoplasm evident in the sub-endocardium region. There were also presences of few leucocytes and fibroblast-like spindle cells. Certain areas also show loss of cross-striation and general disruption of the cellular ultra-structure. The samples from rat No.2 showed loss of nuclei in certain sub-endocardium regions, indicating dead cells, while other areas showed internalisation of large nuclei (Figure 2). The internalisations of the large nuclei are indicative of the myocytes’ regeneration process. In rats No.3, 4, 5, and 6, the heart samples showed little difference from control samples, except for the presence of large, internalised nuclei, indicative of regenerative cells. In rat No.5, the sub-endocardium also showed a few foci of necrosis with eosinophilic changes. Masson’s Trichrome Stain (MTS) MTS was used to highlight any fibrous changes to the heart tissue of the rats, which may occur due to healing and scarring of myocardium after an infarct or similar injury. The samples from MA group rats do not show any noticeable fibrous tissue changes compared to the control samples using MTS for observation under light microscopy. Immunohistochemistry In rat No.1 of the MA group, the foci of cellular infiltration were found to be stained similarly to its surrounding area (Figure 3), thus indicating the clusters of cells were actually regenerating myocytes. However, there may still be a few leucocytes or macrophages present within these foci of cellular infiltration, and further investigation with other anti-leucocyte or anti-macrophage antibodies can be used to elucidate their presence. In all the MA group rats, the myocardium samples were stained in almost uniform intensity, with several areas of differentiated staining intensity of DAB. Thus, the presences of cellular death within the samples were confirmed Table 1 summarizes the observed pathological changes in the samples of the MA group, in relation to the type of change observed and the extent of spread of each type of pathological change. Although the expected parameters of eosinophilic changes and contraction band necrosis were not observed in most of the samples, the presence of enlarged, internalised nuclei, and the absence of nuclei in certain myocytes showed a statistically significant relationship (P value of <0.05 using Kruskal-Wallis test) between the MA group rats and the control group rats. Discussion The acute dose of MA injected to the rats in this experiment were determined so that the rats would be able to show effects of acute MA intake and be able to survive for a day (13, 15). However, a complication to the design of this study arose when four of the MA group rats died within two hours after the MA injection, while a fifth rat died within four hours of injection. The deaths of the rats occurring within such a short time resulted in certain histopathological changes that were indicated in previous studies were found to be absent in the MA group rat samples. The difference in the length of time where each rat had survived after MA injection also could not be determined. The histopathological changes observed in the MA group rats’ samples include cellular infiltration in rat No.1; enlargement and internalisation of nuclei in all samples; loss of nuclei in certain parts of all samples; and eosinophilic changes in a few foci of necrosis in rat No.5. Previous studies in the acute dose intake of MA had indicated that eosinophilic changes can be noticeable in rats after 2.5 hours of acute MA administration, while cellular infiltration were noticeable after 18 hours of MA administration (15). The eosinophilic changes in rat No.5 and the cellular infiltration in rat no.1 were in agreement with the findings of the previous study (15). The cellular infiltration in rat No.1 was found in the sub-endocardium, particularly near the left ventricle free wall region. The sub-endocardial location of the cellular infiltration may be due to transmural gradient in blood flow, which resulted in the inner layer of the wall being more severely affected than its outer layer. In a typical transmural infarct the corresponding gradient in ischaemic injury initially produces rapid coagulative necrosis of the inner layer of the wall and lethal injury, subsequently propagates itself towards the epicardial surface to an extent dependent on both time and the characteristics of the vascular bed involved (17). The cells found in the foci of cellular infiltration in rat no.1 were identified as regenerating myocytes, with the presence of a few macrophages and leucocytes, but there were no fibrous tissue observed in these areas. There were no signs of inflammatory reaction in the tissue, even though death of cells was evident in scattered areas of the myocardium. The regenerating myocytes indicated that the affected tissue were trying to repair themselves by producing new myocytes to compensate for the dead cells. Macrophages and leucocytes were suspected to be present at these sites of regenerating myocytes, mainly because the macrophages function to remove dead cells through phagocytosis, thus eliminating the toxic substances from being released by dead cells in the damaged tissue area and preventing further tissue damage. Although the observation indicated certain cells in the foci of cellular infiltration were macrophages or leucocytes, further staining using anti-macrophage or anti-leucocyte antibodies is needed to have a positive confirmation of the presence of these cells. However, one major difference between the results of this study and previous studies is the absence of contraction band necrosis, a characteristic pattern of myocardial cell alteration that was present in experimentally induced acute regional myocardial infarcts of 2 hours or more duration (15, 17). Contraction band necrosis was reported to be frequently encountered in recent acute myocardial infarcts, and its presence facilitate the definitive diagnosis of sudden cardiac death (17). As such, the short duration of which the rats in the MA group survived in this study should be adequate to show contraction band necrosis. The absence of contraction band necrosis, however, indicates that the toxic effects of MA on other major organs apart from the heart may have caused the early deaths of the rats in MA group, before the changes to the myocardium had become noticeable. The disposition of MA and its metabolite amphetamine is highest in kidneys, followed by spleen, brain, liver, heart and serum (12). It was also observed that high MA concentrations in the brain occurred immediately after intravenous bolus dosing, suggesting that there is essentially no hindrance to passage of MA at the blood brain barrier, and MA distributes very rapidly to all tissues studied except the spleen (12). As such, there is a high probability that the deaths that occurred in the MA group rats in this study were due to the toxic effects of MA in other major organs, most probably the brain, and not due to toxic effects on the heart. However, the scope of the study limited the choice of exploring the effects of acute high dose administration of MA on the other major organs as well. Loss of staining with antibodies to myoglobin is the most sensitive and reliable diagnosis of early myocardial ischaemic damage (16). The results of the immunohistochemistry staining show that most of the samples have varying intensities of brown coloured staining by diaminobenzidine tetrahydrochloride (DAB). Thus, it can be concluded that the myocardium may have suffered some form of ischaemic damage to the tissue, which could have been due to the direct effect of MA in the blood or by other pathways of pathological damage that had yet to be explained. The deaths of rats within four hours of acute MA administration on a dose designed for the rats to survive for 24 hours indicate that there may be a need to re-evaluate the toxic and lethal dosages of MA for use in animals testing. However, the exact mechanism of MA toxicity that leads to sudden death is still unknown (3), thus further investigation into this issue should be done to provide a helpful guide for medical examiners when dealing with cases involving sudden deaths where MA abuse may be suspected. Further testing procedures such as examination of changes in other major organs and detection of serum levels of MA may be necessary to help detect deaths due to acute intake of MA. The use of electron microscopy in conjunction with light microscopy is also recommended, as they would allow clearer differentiation of the necrotic changes in myocardium or other major organs. It is undeniable, however, that an acute dose intake of MA will lead to serious damage of the heart or other major organs that may possibly lead to death, and as such, drug abusers and the society in general should be aware of the dangers of abusing this drug or other harmful drugs. Acknowledgements The authors wish to thank the Department of Chemistry, Malaysia for supplying the MAHCl used in the experiment, as well as the staff of the Pathology Laboratory of Hospital Universiti Sains Malaysia, and Biomedicine Laboratory, School of Health Sciences, USM. This research was conducted under IRPA grant no. 06-02-05-00021-EAR References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08004t1.jpg] [mj08004f3.jpg] [mj08004f2.jpg] [mj08004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}