 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 15, No. 1, Jan 2008, pp. 44-48 CASE REPORT A Rare Case of Paediatric Pontine Glioblastoma Presenting as a Cerebellopontine Angle Otogenic Abscess Kantha Rasalingam, Jafri Malin Abdullah, Zamzuri Idris, Hillol Kanti Pal, Nasser Wahab, Effat Omar* and Salmaa Win Mar** Department of Neurosciences, *Department of Pathology, **Department of Radiology,
School of Medical Sciences, Universiti Sains Malaysia, Health Campus,
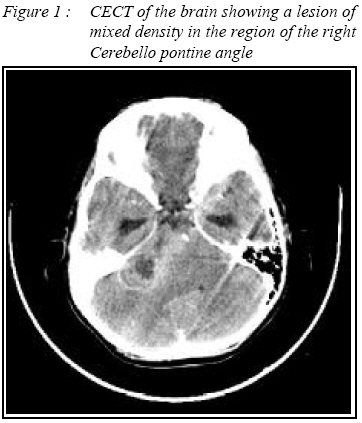
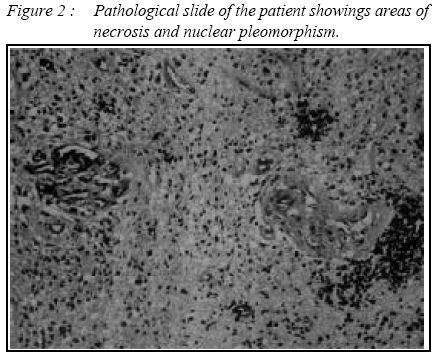
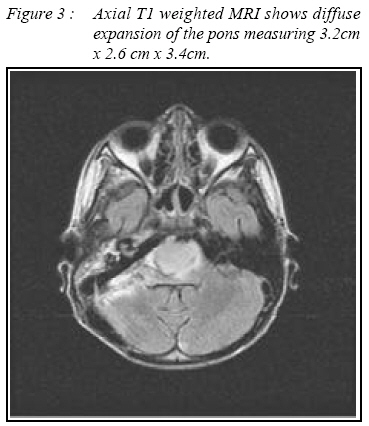
16150 Kubang Kerian, Kelantan, Malaysia Submitted-20-02-2005, Accepted-03-12-07 Code Number: mj08008 We describe rare case of a 9-year old boy who presented with a two- week history of right ear discharge and mild fever. Contrast enhanced CT scan of the brain showed a lesion in the right cerebellopontine angle with mild enhancement mimicking early abscess formation. Involvement of the mastoid air cells pointing towards a radiological diagnosis of mastoiditis reinforced the diagnosis of an abscess. A magnetic resonance imaging (MRI) was planned for the patient but his conscious level deteriorated and patient slipped into coma warranting immediate surgical intervention. Intraoperatively, about 90% of the tumour was removed and the appearance of the tumour resembled that of an acoustic schwannoma but histopathology confirmed the diagnosis of a glioblastoma multiforme (GBM). MRI done post operatively showed lesion in the pons confirming the diagnosis of an exophytic pontine glioblastoma multiforme. Key words : Maxillary molar abscess, cavernous sinus thrombosis, superior ophthalmic vein thrombosis. Introduction Paediatric high-grade gliomas include a heterogeneous group of tumors with different sites of origin and histologic aspects, and they affect children of different ages. These tumors can originate from any site in the central nervous system (CNS), particularly the supratentorial region and the brainstem. They rarely originate from the spinal cord or the cerebellum.(1) When arising from the brainstem, these high-grade gliomas are usually called diffuse brainstem gliomas. Histologically, most of these neoplasms contain only an astrocytic component and are called either anaplastic astrocytoma (AA; World Health Organization [WHO] grade III) or glioblastoma multiforme (GBM; WHO grade IV), depending on their grade. Tumors with mixed or nonastrocytic phenotypes are uncommon in pediatric patients. The number of children with high-grade gliomas is much smaller than the number of adults with these neoplasms. Whereas 40%–50% of all paediatric CNS tumours are gliomas, supratentorial high-grade astrocytomas constitute only 6%–12% of all primary paediatric brain tumors, and diffuse brainstem gliomas constitute only 3%–9%. (1, 2) Brainstem tumours are perhaps the most dreaded of cancers in children due to its poor prognosis, yet they remain an area of intense research. Brainstem gliomas account for about 10% of all brain and spinal childhood tumours.(1,3) Peak incidence for this tumour occurs around age 6 to 9 years. The term glioma encompasses various tumour types such as ganglioglioma, pilocytic astrocytoma, fibrillary astrocytoma, anaplastic astrocytoma and glioblastoma multiforme.(1) They have historically been some of the most difficult paediatric cancers to treat. Case Report We present a 9-year-old boy who was referred to our centre after complaining of double vision and ataxia of 2 weeks duration. He complained of severe headache 48 hours prior to admission which was retro-auricular in location associated with a yellowish discharge from the right ear, and fever . On examination in our centre, he was drowsy but arousable. Fundoscopy revealed bilateral papilloedema. Further examination showed a right 6th nerve palsy with horizontal nystagmus and mild cerebellar signs localized to the right. Otoscopic examination revealed pus in the right external external auditory canal. A CT scan of the brain ( Figure 1) was performed showed an ill defined isodense lesion in the right cerebellopontine angle measuring 2.4 x 2.3 x 3.8cm with moderate enhancement and acute obstructive hydrocephalus. Fluid collection was noted in the right mastoid air cells and middle ear cavity. The impression obtained at this stage with the clinical evidence of mastoiditis and ear discharge was that of a cerebral abscess. The total white cell count was not raised and there was no clinical evidence of bacteraemia. The patient was immediately planned for a MRI on the same day of admission, but while waiting for it his conscious level deteriorated and emergency surgery was undertaken. The aetiology for the deterioration was both due to his hydrocephalus and the compression of the brain stem by the lesion. A right retromastoid sub occipital craniectomy was performed immediately. A right parietal burr hole was made and ventriculostomy gave clear cerebrospinal fluid (CSF) under high pressure.Transdural aspiration from the suspected right cerebellar lesion revealed no pus. Durotomy was performed which did not relieve the tense right cerebellum. The removal of the lateral one third of the right cerebellar hemisphere had to be done due to herniation which did not response to medical andtreatment. It revealed a right cerebellopontine angle mass which was huge and enveloped by a layer of arachnoid mater. The tumour was reddish grey, noncapsulated, firm, solid with a central area of necrosis containing 3-4 ml of dirty greyish fluid. The right lower cranial nerves were protected along with the VIIth nerve and VIIIth nerve. Intraoperatively it seemed to be arising from the extracanicular portion of the vestibular nerve. The posterior lip of the porus acousticus was intact. There were no hemodynamic changes during surgery. Subtotal tumor removal was achieved with a small remnant of the tumor attached to the pons left in situ. Pathological Examination Fragments of tissue were composed of sheets of neoplastic glial cells with numerous small capillaries in between them.(Figure 2) The tumor was cellular with some pleomorphism and some cells undergoing mitosis were noted. Endothelial proliferation and areas of necrosis were noted. The tumor cells stained positive for glial fibilary acid protein (GFAP). The tumor also expressed vementin. In conclusion, the histological diagnosis was that of a glioblastoma multiforme. Post operative progress Post operatively the patient was kept on ventilatory support for 24 hours. Once conscious, he was able to move all his limbs. He had a mild right sided 7th lower motor neuron palsy and a right sixth nerve palsy with associated nystagmus and mild right sided cerebellar signs. In view of the histopathology of glioblastoma multiforme, a brain MRI was ordered and the findings are consistent with that of a diffuse pontine glioma. (Figure 3). The patient was managed in the ward with a hospital acquired infection. Two months after surgery the patient was taken home by the parents against doctor’s advice and died on the same day. Discussion This case is presented as there was a discrepancy in the clinico-radiological diagnosis with that of the operative and histopatholigical diagnosis. We are presenting this case because of its subacute presentation (with a history of less than 2 weeks) mimicking that of an otogenic cerebellar abscess with obstructive hydrocephalus. The radiological investigation available on admission ( plain and CECT scan brain) suggested a rapidly advancing lesion in the right side in the posterior fossa. The peripheral vein enhancement suggested an inflammatory pathology. At surgery however, a solid mass with a nectrotic central area encased by arachnoid layer in close proximity and anterior to the VII th and VIII th nerves suggested an acoustic neuroma. The site of origin of this tumour could be the cerebellum, root entry zone or the brainstem. Post operative MRI however confirmed the diagnosis to be that of a diffuse brainstem glioma. The histopathological diagnosis of this patient was that of a glioblastoma multiforme. With this diagnosis, it was necessary to determine the site of origin of the tumor which could be localized to 3 main regions mainly the pons, the cerebellum or the nerve root entry zone. MRI done post operatively however established the site of origin to be pons. As the tumor originated from the pons and majority of the tumour appeared to be residing outside of the pons the diagnosis of this tumor is a exophytic pontine glioma. In 1985 Epstein et al reported classification schemes based on CT appearance of brainstem tumors.(5) These classification schemes described surgically treatable subgroups of gliomas. A simple way to classify these tumours is into two categories: typical brain stem gliomas and atypical brain stem gliomas. They are now recognized as a heterogeneous group of tumors and have been broadly classified by Epstein in four categories: diffuse, focal, exophytic and cervicomedullary Exophytic brainstem gliomas arise from the subependymal glial tissues and expand outside the pons. However, the area of extension is mainly into the fourth ventricle unlike our patient where the area of extension was mainly the cerebellopontine angle. The clinical presentation of our patient was rather subacute with minimal cranial nerve involvement unlike that presentation of an exophytic glioma. The pathology of exophytic brainstem tumours are mainly that of a low grade glioma however as established our histopathological diagnosis was that of a glioblastoma multiforme. Unlike the majority of brainstem gliomas which are malignant tumors, most exophytic brainstem gliomas are low grade and this alters the management for the patient. Surgery is only potentially beneficial for patients with focal, exophytic and cervicomedullary tumors and not diffuse brainstem tumors. The goal of surgery should be to reduce the tumour size and not aim for complete resection as an attempt to do so might prove catastrophic. The diagnosis of a malignant glioma provided a poor prognosis as GBM carries a median survival rate of less than 12 months. The other possible origin for this tumour could be the nerve root entry zone or the cerebellum. With the exception of Neurofibromatosis type II, paediatric extraparenchymal cerebellopontine angle (CPA) tumors is very rare.(4) Most gliomas encountered in the cerebellopontine angle involve the CPA angle as exophytic extension of primary brainstem and/or cerebellar tumors. A CPA glioma is exteremly rare and so rare there have only been 7 cases reported. The rarity of this location and with the MRI findings however, we have ruled this out as a possible site or origin. In conclusion, brainstem gliomas are a common but difficult tumour to treat. From this patient’s clinical presentation, radiological and pathological findings, we can conclude that they need not follow the normal pattern as described by previous literature. Nevertheless, all brainstem gliomas need to be classified carefully as their management will depend on its location. With the advancement of gene therapy, it is hoped that futher development in the management of brainstem gliomas is achieved. References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08008f3.jpg] [mj08008f2.jpg] [mj08008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}