 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 15, No. 2, April 2008, pp. 29-32 ORIGINAL ARTICLEOutcome of Laser-Assisted Uvulopalatoplasty (LAUP) in the Management of Snoring in Hospital Universiti Sains Malaysia (USM) Baharudin Abdullah, Nik Adilah Nik Othman & Dr Mohd Khairi Daud Department of ORL-HNS,
School of Medical Sciences, Universiti Sains Malaysia, Health Campus,
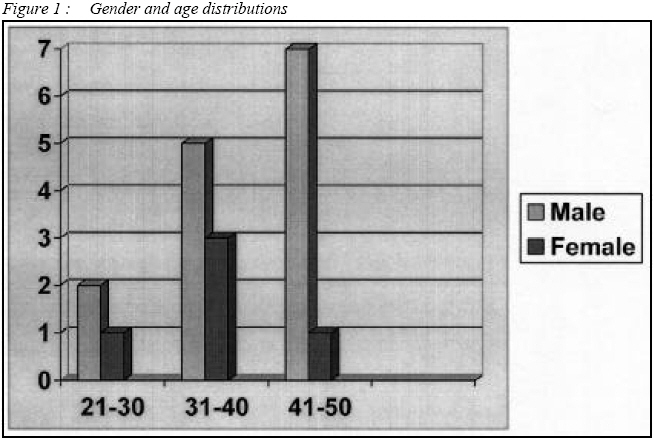
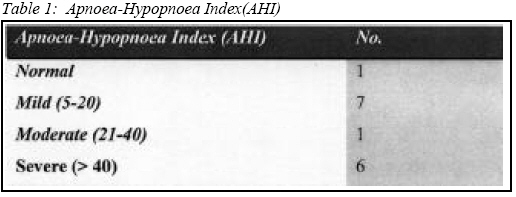
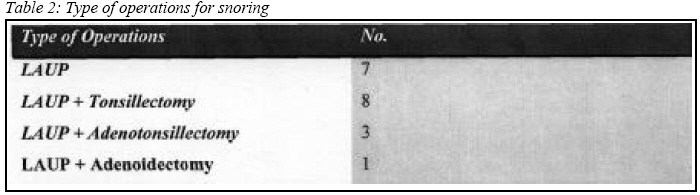
16150 Kubang Kerian, Kelantan, Malaysia Submitted-28-10-2007, Accepted-24-02-08 Code Number: mj08015 To determine the outcome of laser-assisted uvulopalatoplasty for the management of patients with snoring in Universiti Sains Malaysia Hospital (HUSM). A retrospective review of patients who underwent LAUP with or without tonsillectomy or adenoidectomy under general anaesthesia between December 2003 to December 2006. Data was obtained from admission and follow-up records in the otorhinolaryngology clinic of USM Hospital (HUSM). A total of nineteen patients underwent procedure for the treatment of snoring. Majority of these patients presented with symptoms of loud snoring and daytime somnolence. The main operations performed were LAUP with or without tonsillectomy or adenoidectomy. The justification for LAUP were overhanging and excessive uvula or soft palate, whereas for adenotonsillectomy were the hypertrophied adenoids and tonsils. On follow-up, most of the patients claimed improvement of snoring within the first 2 months post-operation. However, majority of them defaulted follow-up after that. One patient (AHI preoperatively was mild) was reviewed up to 8 months with no snoring. One patient (AHI was severe preoperatively and normal post operatively) remained in our follow-up was satisfied with the operation. Two patients continued to experience snoring post LAUP despite trial of non-surgical methods. The outcome of LAUP in our patients showed variable results. This showed that patient selection is very important to achieve good result in LAUP. Long-term follow-up is also essential to document the success for LAUP. Key words : Outcome, Laser assisted Uvulopalatoplasty, Snoring, Hospital Universiti Sains Malaysia. Introduction Snoring is an important social problem seen in both men and women. Snoring occurs as a result of soft tissue vibration caused by a partial upper airway collapse during sleep (1). The most common site of obstruction during snoring is the soft palate; however, other regions of the upper airway tract may cause snoring such as the nose, base of tongue, tonsils and epiglottis (2,3). Snoring can occur as primary snoring or as part of a syndrome of obstructive sleep apnea (OSA). There are a number of options for the treatment of primary snoring and OSA. The non-surgical treatment includes behavioural changes such as weight loss, cessation of consumption of possible beverages (alcohol, tobacco) and of sedative hypnotic medication before sleep, and especially for patients with moderate to severe OSA, they are treated with nasal continuous positive airway pressure (CPAP) (1, 4). This appliance is reasonably effective but it represents a control and not a cure. Many patients find it cumbersome and are unwilling to continue using it and seek surgical treatment instead (4). The surgical management of snoring focuses on the velopharynx (1). The aim is to enlarge the velopharyngeal isthmus by removing excess mucosa without damaging the musculature of the soft palate, resulting in reduced soft palate vibration and thus snoring (3). Several methods have been described. In early 1980, uvulopalatopharyngoplasty (UPPP) was introduced, followed by laser-assisted uvulopalatoplasty (LAUP) in 1986. Later cautery-assisted uvulopalatoplasty (CAUP) in 1995 and more recently, radiofrequency tissue volume reduction (RFTVR) has been added to this surgical regime (5). UPPP remains the most commonly performed surgical procedure for primary snoring and type I and II OSA (1, 2, 5). Type I or retropalatal collapse occurs at the level of soft palate, while Type II or mixed airway collapse occurs both behind palate and tongue base. Type III or retrolingual collapse occurs at the tongue base (5). Initially LAUP was used in the treatment of primary snoring but has recently gained some acceptance as an alternative to UPPP for the treatment of type I and II OSA, especially since UPPP has a relatively high complication rates of velopharyngeal insufficiency and occasionally nasopharyngeal stenosis (5). Materials and Methods We performed a retrospective review of patients who underwent LAUP with or without tonsillectomy or adenoidectomy under general anaesthesia between December 2003 to December 2006. Data was obtained from admission and follow-up records. The clinical presentations and examinations were looked into. The overnight polysomnography results were documented whenever available. The justifications for the surgery were also documented. All surgical procedures were performed by the ORL surgeons in the Department of Otorhinolaryngology at University Science Malaysia Hospital. The outcome of surgery was assessed after follow-up. Results Retrospective analysis revealed that of the 19 patients, 14 were males and 5 were females, giving a male :female ratio of about 3:1. The age of the patients ranged from 24 to 50 years old. The mean age was 38 years old. Figure 1 illustrates the patients’ distribution by age and sex. The follow-up period average was 2 years and 6 months. Body mass index (BMI) was the measurement of weight in kg divided by the power of two of the height in metre (kg/m2). Eleven patients or 57.9 % have their BMI calculated and the mean BMI was 36.3 kg/m2 but the mean weight was 93.4 kg. Majority of these patients presented with symptoms of loud snoring and daytime somnolence. Fifteen out of nineteen (78.95 %) of them had undergone polysomnography before their operations and their results are illustrated in table 1 below. Postoperative polysomnography was performed in three cases and the results were not consistent in showing improvements. One polysomnography showed an improvement from severe to normal AHI. The second one gave result of severe AHI for both polysomnography but with an improved index number (67.2 to 41.2) and symptomatically patient claimed less snoring than before. The third one gave a worsening result, the postoperative AHI was moderate compared to normal result preoperatively, and the patient also claimed no change of the symptoms. The main operations performed were LAUP with or without tonsillectomy or adenoidectomy. Table 2 illustrates the type of operations performed. The justification for LAUP were overhanging and excessive uvula or soft palate, whereas for adenotonsillectomy were the hypertrophied adenoids and tonsils. On follow-up, most of the patients claimed improvement of snoring within the first 2 months post-operation. However, majority of them defaulted follow-up after that. One patient (AHI preoperatively was mild) was reviewed up to 8 months with no snoring. One patient (AHI was severe preoperatively and normal postoperatively) remained in our follow-up until 2 years and 6 months where he was discharged and satisfied with the operation. Two patients continued to experience snoring post LAUP, despite trial of non-surgical methods. Discussion Snoring is a social nuisance, and may be a precursor to more serious conditions like upper airway resistance syndrome (UARS) and obstructive sleep apnoea syndrome (OSAS). OSAS, if untreated has been implicated in the development of serious medical consequences which include cardiac arrythmias, systemic and pulmonary hypertension, myocardial infarction and an increase in the risk of motor vehicle accidents. Treatment options can either be medical, non-surgical or surgical procedures. Although it has been clearly documented that full-time use of nasal CPAP is necessary to control the sequelae of OSAS, compliance remain a major problem. Compliance is also an issue with medical treatments and even oral devices. Succesful surgical treatment remains the only treatment option that does not require daily compliance. Since Dr. Fujita’s introduction of Uvulopalatopharyngoplasty (UPPP) in 1980, it has been the surgical treatment for OSAS. Recently, laser-assisted uvulopalatoplasty (LAUP) has proliferated as a treatment for snoring and OSAS because it is relatively inexpensive, rapid and has lower and less severe complications (6). In our centre, LAUP with or without adenotonsillectomy has virtually replaced uvulopharyngopalatoplasty (UPPP) as the preferred treatment for primary snoring and OSAS. Postoperative complications of LAUP include pharyngeal pain and dryness, minor bleeding, oral candidiasis and temporary velopharyngeal insufficiency which we have not found in our series. Most epidemiologic data on snoring comes from subjective reports by both the snorer and partners. In Walker’s initial study of 105 snorers who underwent LAUP, 60 % of patients and bed partners reported complete or near complete elimination in the snoring, 29% noted a partial improvement and 10 % noted no improvement. Kamami’s most recent report showed almost similar results. These LAUP results are comparable to the UPPP subjective results (6). The subjective reports on the efficacy of LAUP are quite encouraging. However, subjective data alone is not adequate and objective testing is needed to accurately document the efficacy of LAUP. In Walker’s study on the objective assessment of snoring using a sonographic device, SNAP, he found that low frequency (velum-like) relative loudness from the oronasal respiration, correlated best with the subjective perception of the snoring (6). He suggested that further follow-up studies are needed to determine the long-term effectiveness of LAUP in mitigating snoring. Other objectives studies have suggested that up to 50 % of all patients obtain little or no long-term benefit from LAUP (6). The outcome of LAUP in our patients showed variable results. In the majority of patients, thirteen out of nineteen (68.4%) showed improvement in the immediate follow-up period. Unfortunately, two of the patients (10.5%) showed recurrence of symptoms. Five patients did not turn up for follow-up after the operation so we were unable to record any results. We believe these results are due to failure of the palate to stiffen after the laserization. The patients who had undergone combined LAUP and adenotonsillectomy (11 patients) did better than patients who underwent LAUP alone (7 patients). This variability is due to the fact that the LAUP was done in all categories of patient with various severity. This showed that patient selection is very important to achieve good result in LAUP. Conclusion The outcome of LAUP in our patients showed variable results. This showed that patient selection is very important to achieve good result in LAUP. Long-term follow-up is also essential to document the success for LAUP. References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08015f1.jpg] [mj08015t2.jpg] [mj08015t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}