 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
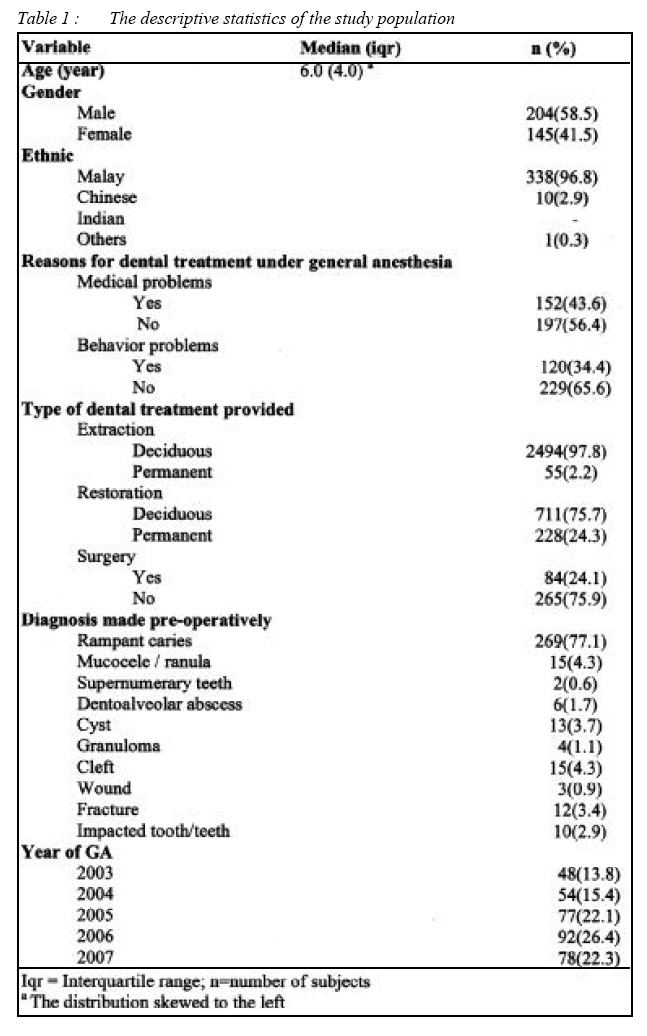
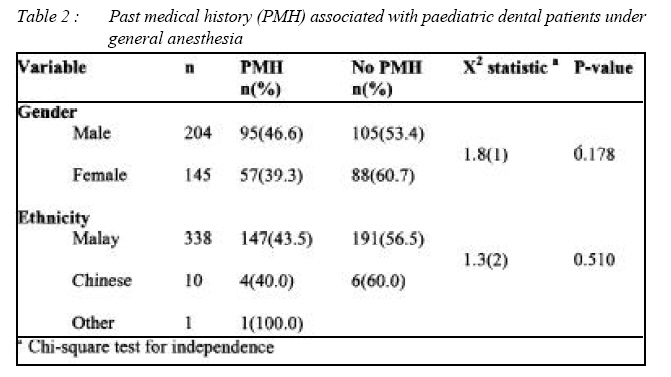
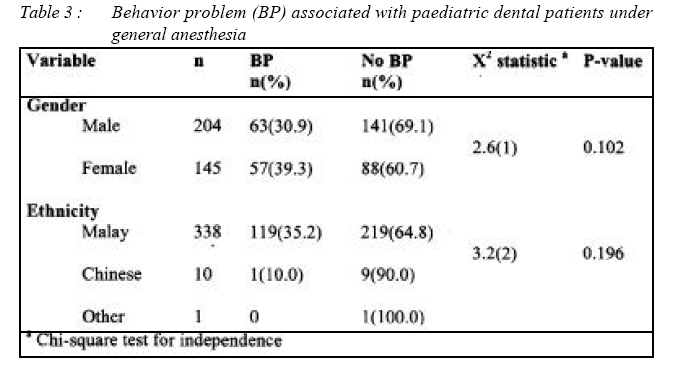
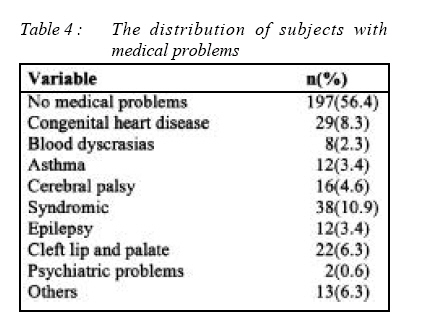
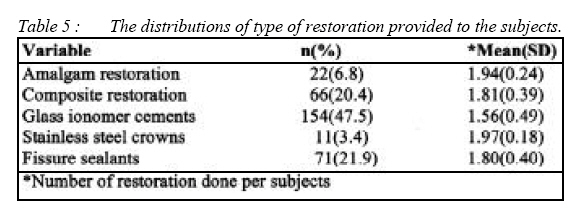
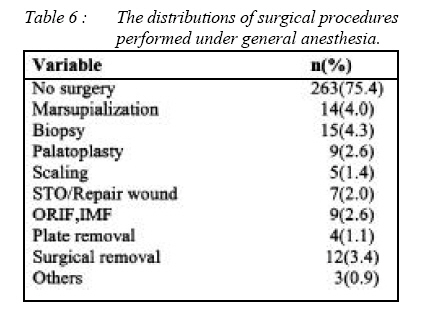
ORIGINAL ARTICLE Utilization of dental general anaesthesia for children Zarina Abdul Karim, *Normaizura Musa, *Siti Noor Fazliah Mohd Noor Dental Specialist Clinic, Hospital Kuala Terengganu, 20400 Terengganu. Submitted-1-1-2008, Accepted-1-8-08 Code Number: mj08024 A small number of children and adolescents need dental treatment under general anaesthesia (GA), either for medical reasons or due to lack of cooperation during dental treatment. The objective of the study is to identify the type of treatment that has been carried out under GA in Hospital Universiti Sains Malaysia (HUSM). A retrospective record review study from hospital records of dental patients (under 18 years old) receiving dental treatment under GA from 2003 until 2007 were retrieved from the database. Information such as the reason for GA, and the type of treatment provided was recorded in data sheet. The data were analyzed using SPSS 12.0.1 for Windows. It was checked and verified for errors. A total of 349 cases were treated of which 43.6% had medical problems. Patients were mostly diagnosed to have rampant caries (77.1%) and some of them have behavioural problems (34.4%). Treatment pattern in deciduous dentition revealed more extraction (97.8%) as compared to restoration (75.7%) whereas in permanent dentition more restoration was done (24.3%) as compared to extraction (2.2%). Majority of the restorations were done using Glass Ionomer Cements (47.5%). Biopsy (4.3%) contributed mainly to the surgery (24.1%) done during GA. General anesthesia is necessary when dental disease is interfering with health and general well-being of patient and it can facilitated dental treatment allowing dentists to benefit from improved treatment conditions and provide a higher quality of care. Key words : Dental general anaesthesia, Extraction of teeth, Restorative treatment, Surgery, Rampant caries Introduction Dental services in Malaysia have started since late sixties (1). All the way through these years, it has expanded to improve the dental health status of the population of Malaysia by providing promotive, preventive, curative and rehabilitative dental services. The paediatric dental treatment under general anesthesia (GA) was made available to patients in many main cities in the country, nevertheless study or data regarding the matter is scarce. Therefore, this study is conducted to look up into the area and the objective of the study was to identify the type of treatment that has been carried out under GA in HUSM. In treating children, the delivery of pain free dentistry is of prime importance for all dentists. Pain control is part of behavior management. If pain is not controlled, it will affect the standard of work dentist can achieve. Dental treatment facilitated by general anaesthesia allows dentists to benefit from improved treatment conditions and provide a higher quality of care. In additional , it also permit dentists to treat patients who otherwise could not be treated in a private practice setting, including highly anxious and/or phobic adults, pre-cooperative and uncooperative children, patients with developmental disorders, patients with muscle-control problems and patients with medical conditions that may be exacerbated by anxiety. Many patients elect to undergo general anaesthesia to reduce stress and increase comfort (2), and some patients needed general anaesthesia because of lack of cooperation as a result of age, maturity or physical or learning disability (3). An audit was carried out on children (≤17 years) with special needs who were treated under general anaesthesia in the Day Stay Centre at the Royal Hospitals NHS Trust, London, between 19851995. It showed that during these years, 586 child The provision of dental treatment under general anaesthesia falls into three main groups that is out-patient ‘short case’ dental chair anaesthesia, out-patient ‘day stay’ intubation anaesthesia and inpatient ‘hospital stay’ intubation anaesthesia (5). There were various types of patients admitted for dental treatment under general anaesthesia including healthy patients with behaviour problems and patients with special needs such as those having handicapping conditions like congenital heart disease and bleeding tendencies (6). Behavior problems and inability to cooperate were the main reasons for treatment under general anaesthesia (7) and also patients that are too young to cooperate that have early childhood caries (8). Patients with medically handicapped conditions may benefit from general anaesthesia (9) including those with intellectual disability such as autistic disorder (10), cerebral palsy and mentally retarded patients (11). Studies have shown that the quality of restoration carried out under general anaesthesia were far more better than under local analgesia since there were better moisture control and planned restoration placements(12, 13). There are also children who had undergone repeated general anaesthesia and the common characteristics of these children is that they have 100% caries involvement of maxillary central incisors at time of initial treatment, majority of central incisors were non restorable, still using nursing bottle at the time of general anaesthesia, child responsible for brushing own teeth, poor cooperation in the medical and dental setting, difficult personality as described by parent, dysfunctional social situation and lack of follow-up dental care (14). This study directs at providing baseline information regarding the types of treatment for paediatric dental patients carried out under general anaesthesia. It has its own restrictions and is bound to attract criticism and require further improvements. It is hoped that the data from this survey will be useful for other researchers. The information attained in this study would be decisive especially in planning of future general anaesthesia service in paediatric dentistry. Furthermore, it also will facilitate dentists in determining the most appropriate treatment plan for paediatric patients, especially for those with special requirements. This will enable the clinicians to expand the quality of dental service in Malaysia for the betterment in the future. Materials and methods The general anaesthesia service was provided as ‘in-patient’ hospital stay intubation anaesthesia at HUSM where the patient had to be warded prior to the treatment under general anaesthesia. All patients were firstly seen by the staff nurses at the outpatient clinic and upon examination if the child was uncooperative or have medical problems the patients were referred to the dental officer (DO) oncall. The DO will later refer the patient for consultation with the paediatric dentist. All patients referred for treatment under general anaesthesia will receive a full consultation, proper history and examination by the paediatric dentist, and where necessary, patients that have medical problems will have a pre-anaesthetic assessment and check-up at respective paediatric clinic such as cardiology or nephrology. Parents were informed of the detailed procedure and proposed treatment plan including the fasting and discharge procedures. The parents were given admission form with telephone number to contact if they want any additional information or need to cancel the general anaesthesia if the child became sick at the designed date. Then the child’s name is placed on the waiting list. The parents and child will have to wait about two months before their turn for the general anaesthesia depending on the number of existing patients in the waiting list. During the hospital stay in the ward, the information regarding fasting and discharge will be repeated again by the anaesthetic and written consent is obtained in the ward prior to the conduct of general anaesthesia. On the day of the general anaesthesia, the patient was transferred from their respective ward to the operating reception area and was examined again by the anaesthetist and the surgeon performing the procedures. Some patient may need premedication. One parent will accompany the child to the operating room and once the child is sedated, the parent is sent to the waiting area at the recovery room. Nasal intubation is routine and the child was fully monitored throughout the procedure. The child is made conscious once the dental procedures were completed and later sent to the recovery room for post-operative monitoring before being transferred back to their respective ward. If the child’s condition is satisfied clinically, they are allowed to be discharged 6 hours post-operatively on the same day. The patients were reviewed within 1 week at the specialist dental clinic for assessment of their dental conditions. For healthy patients, they are discharged from the clinic after 1 month review and later placed in the waiting list for the undergraduate students. Patients with medical problems will be reviewed three monthly at the paediatric dentist specialist clinic. This was a retrospective record review study where the source of data was drawn from hospital records of paediatric dental patients (under 18 years old) who were treated under GA from 2003 until 2007. The study was approved by the Internal Review Board of Human and Ethics Committee, HUSM prior to conduct of the study. The data was collected within a period of 10 months. To achieve the precision of 5% for the expected prevalence of 40% (4) there is a need of sample size of 369 subjects. Based on the records from the database, there were 349 subjects and all the records were retrieved. The variables registered for this descriptive study were age, gender, ethnicity, type of dental treatment carried out under general anesthesia in HUSM such as restorative treatment, extraction of teeth and surgical cases. All data was entered and analyzed with Chi-square test using SPSS Version 12 for Windows (SPSS Inc., Chicago, IL, USA). The results is considered significant at P<0.05. Results Three hundred and forty-nine paediatric dental records were retrieved. The age distribution of the patients are skewed to the left, thus the median (6.0 year-olds) and inter quartile range (4.0) were used to describe the age. More male patients (58.5%) had been treated under GA as compared to female patients (41.5%). Many deciduous teeth were extracted (97.8%) as compared to permanent teeth (2.2%). There was a tendency for the increase number of cases treated under general anaesthesia. The details of the descriptive statistics of the study population are shown in Table 1, respectively. There were 43.6% patients with medical problems that were treated under general anaesthesia and 34.4% patients with behavioural problems were administered for general anaesthesia. There was no significance difference detected between the medical problems in relation to race and gender, and also between the behaviour problems in relation to race and gender (p>0.05). The results are shown in Table 2 and Table 3, respectively. Patients with syndromic features (10.9%) followed by congenital heart disease (8.3%) and cleft lip and palate (6.3%) had mainly contributed to the group of patients with medical problems as shown in Table 4. Glass ionomer cements (47.5%) were commonly used to restore the teeth (Table 5) and surgical biopsy (4.3%) was often performed since child patients were unable to tolerate pain during the procedure (Table 6). Discussion The dental general anaesthesia service was made available after the successful setting up of School of Dental Sciences in 1999 in the North-East of Malaysia. Before the inaugural opening of the dental school which acts as teaching hospital to future dentists, many patients were treated in the government hospital at Kota Bharu by the attending oral surgeons. In this study, no consideration were taken regarding the level of dental disease, using the deft or DMFT index as compared to other study (15) where the authors had recorded these index before the treatment begun. This index may help in determining the most appropriate dental treatment for the patient. For example, in paediatric patient with medical problems who had undergone general anesthesia, the index will help dentist to justify between extraction and restoration since high deft or DMFT index might suggested high caries risk (16). Thus, we cannot appreciate the pattern of dental treatment provided for the patient based on the level of dental disease. There was no assessment done regarding the level of socioeconomic status of the patient and their parents. With that information, probably it would be possible to gather Knowledge, Attitude and Practice (KAP) of the parent towards the treatment plan for their child. In additional, appropriate strategy can be designed in order to help parents to get the picture of the rationale for the treatment. Out of 349 sample size, there were 58.5% males and 41.5% females. This data did not reflect the actual gender percentage in Kelantan, which reveal that female population was more dominant than men (17). In comparison with other study, it was noted that there was no significant difference in the proportions of girls and boys utilizing the service (18). The data showed that the median age of the paediatric dental patients who had undergone dental treatment under general anesthesia was 6 years old, with the distribution skewed to the left. This finding is in accordance as reported by Alcaino and coworker (18) where in their study more than twothirds of the children are less than 6 years of age. In their study, there reported that it is possible that this 4 to 6 year-old group represents children with heavily restored dentitions requiring maintenance. A study done by Camilleri and co-worker discovered that the average age of patient was 7 years old (19). This study showed that majority of the patients was Malays as the majority of the populations in Kelantan were Malays (17). In other centres, most patients were Caucasians; nevertheless there was an increase in the number of Asian children being treated (20) although Asians were minority group. Many of the children treated had some form of medical problems. This finding was in concordance as reported previously (20) and on contrary, some researchers reported that behavior problems and inability to cooperate were the main reasons for treatment under general anesthesia (8). Other study showed significantly higher number of dental procedures for healthy patients than for special needs patients due to the anxiety and fear to dental procedures among the healthy patients even though they did not have behaviour problem (6). Using general anesthesia, necessary precautions were able to be taken for patients with complicated medical conditions, thus avoiding extra stress for the patients and their family of admission to an unfamiliar environment overnight. Hence, these groups of patients were better treated in the hospital environment (4). There were many patients with congenital heart problems treated under general anaesthesia as compared to patients with respiratory problems such as asthma and bleeding diathesis in this study (ASA III and IV). This finding is in accordance as reported by Camilleri et al. (19) where about 31.4% of their subjects have congenital heart disease as compared to asthma (27.6%) where most of these patients received comprehensive dental treatment under general anaesthesia. Amongst the cases of patients with medical problems, syndromic child and cleft lip and palate patients were the most treated under general anesthesia. Cleft of the lip and palate was the most frequent congenital malformations of the head and neck region. This finding is not surprising since it has been shown that Kelantan has a higher prevalence of cleft cases as compared to other states in Malaysia (1). In this study, many patients were treated under general anesthesia because of their behavior problem. Nevertheless, other studies showed that some patients were treated under general anesthesia because of their dental fear or because they were too young to cooperate but otherwise healthy (4) and the main background of variables that may cause dental fear include social factors, personality factors and previous negative experience (21). Majority of cases treated were rampant caries followed by cleft, cyst and fracture and is in accordance with other study (21, 22) and may correlate with the current status of caries experience in this country (1). Young patients with rampant caries were the most common reason for treatment under general anesthesia and in some cases the presence of rampant caries was combined with a high level of anxiety resulting in severe management problems (23). The management of patients with rampant caries that have to be treated under general anesthesia where treatment have not been provided before, it is often has to comprehensive and too late to avoid radical action that may involve extractions of all the badly carious teeth (24) and restoration using stainless steel crowns for remaining teeth. The used of stainless steel crowns should be envisaged for restoration on primary molars and tooth that need extensive restoration. These children with rampant caries are highly caries-susceptible and may have recurrent disease; possibly necessitating repeat general anaesthetic, thus careful follow-up including individualized prevention is essential with evaluation of the restorative treatment (23). Restoration of primary teeth with stainless steel crown showed the highest success rate as compared with other type of restorative material (25) and their use in primary teeth are indeed very useful. In this study, majority of deciduous teeth were extracted as compared to the permanent dentition where extraction was not dominant and findings were in agreement as reported previously (21). Previous published data have suggested that medically compromised children (ASA II, III and IV) receiving dental treatment under general anesthesia have had more extractions and less restorations than the ASA I and II children undergoing similar procedures. The ASA II, III and IV children were classified into nine main groups according to their medical diagnosis: cardiac, neurology, craniofacial, dermatology, immunology and viral infections, bleeding, renal/hepatic, respiratory and other (primary multiple system disorders, metabolic and endocrine disorders). Nevertheless, some researchers found that unsurprisingly (since treatment planning for comprehensive care under general anesthesia has to be radical if recourse to further general anaesthetics is to be avoided), there was an overall predominance of extractions over restorations in both groups (19). There was more restoration done for permanent teeth as compared to the deciduous teeth, and Glass Ionomer Cements were the most commonly used restorative materials. This finding is in agreement as reported by a hospital in Saudi Arabia where many teeth were restored using Glass Ionomer Cements (26) but is contradictory to a study reported by Vinkier and co-worker (23) where they used mainly amalgam restorations to restore the primary teeth. Glass Ionomer Cements was mainly choose due to its advantages as a tooth colored material, adhere directly to the both enamel and dentin through an ion exchange mechanism and biologically active, as it is capable of releasing fluoride, calcium and phosphate ions (27). Fissure sealant as a preventive measure was also incorporated for the dental treatment. Surgery conducted under general anesthesia is beneficial to child patients without doubt since they were afraid of needle and cannot stand long surgical procedures under local analgesia. In many cases, general anesthesia allows the dentist to complete treatment rather than delay care because a patient’s anxieties and fears about treatment make him or her uncooperative. By reducing patient apprehension and movement, dentists can offer significantly improved dental care. Current approaches to general anesthesia can provide total relaxation, minimize recall of the procedure and allow for successful treatment of even the most phobic dental patient (2). General anaesthesia for a healthy, fearful child is extremely safe and, in the long run, is the best outcome for the profession and patient (28). Even if dental care under general anaesthesia is a very effective treatment modality, it is often the last resort because of the expense and risk-benefit considerations (29) and also some parents may find it hard to accept (8). One of the most important issues affecting the choice of pharmacological behaviour management is the cost and reimbursement for general anaesthesia (30). Reimbursement for services includes dental procedures, anaesthesia costs and facilities fees, depending on whether the procedure is done in an outpatient care facility or hospital (30). All patients in this study have to be warded for the dental treatment under general anaesthesia to take place. This would definitely increase the cost of providing the general anaesthesia service including maintenance of the general anaesthesia equipment as well as the hospital ward during the hospital stay. Another issue that is generally recognized by the dental community is that the majority of the insurance industry does not cover the cost of general anaesthesia for dental procedures in children (28). There were an increasing number of patients in this study being admitted to hospital for dental treatment to be provided under general anaesthesia and this finding is in accordance as those reported previously (18). It is apparent that the majority of children are of preschool age and have high treatment demands. Although some of these children may readily accept treatment initially, compliance usually decreases as treatment demands in the dental chair increase. Hence, the provision of extensive treatment under general anaesthesia in some children may be justified and such services should be provided safely, effectively and efficiently in the appropriate environment (18). In conclusion, general anesthesia facilitated dental treatment and increases the access to dental care especially for medically compromised patients. It also allows dentists to benefit from improved treatment conditions and provide a higher quality of care. There is a need to include deft or DMFT index in future study. This allows us to know the level of dental disease and will be able to plan better treatment for the paediatric dental patient. There is a need to consider the socioeconomic status of the patient and their parents. The information will provide us the background knowledge of the parents and how they react towards the treatment plan for their child since some researchers have showed that parents have reported more smiling, improved school performance, and increased social interaction after dental extraction under general anesthesia (31). In additional, we as well could design the apt strategy in order to help parent to get the picture of the rationale for the treatment. In future study, the American Society of Anesthesiologist (ASA) Classification should be included to provide the anesthetic risk in the study. This classification, will give the indication for different type of anesthesia in paediatric dental treatment according to the patient’s medical status. In future study, the time taken to do treatment under general anesthesia should be evaluated so that the cost effectiveness of the procedure can be related to the number of the procedure done in the session. The reasons most of the patients received treatment under general anesthesia must also be evaluated as that have been reported previously (32) since this will enable the proper planning for the patients. Acknowledgements Appreciation is extended to the staffs at the Record Unit HUSM and staffs of School of Dental Sciences for their support during the period of this study. References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08024t3.jpg] [mj08024t5.jpg] [mj08024t4.jpg] [mj08024t2.jpg] [mj08024t1.jpg] [mj08024t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}