 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
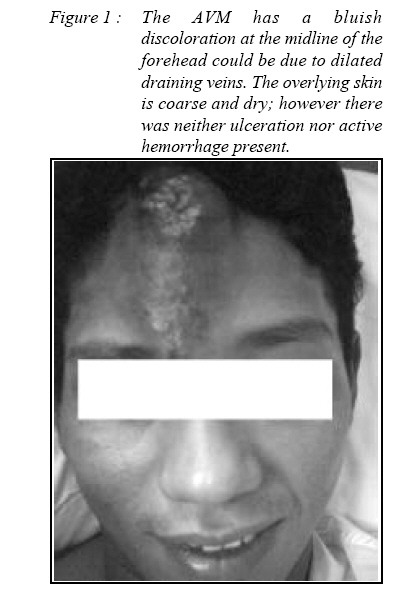
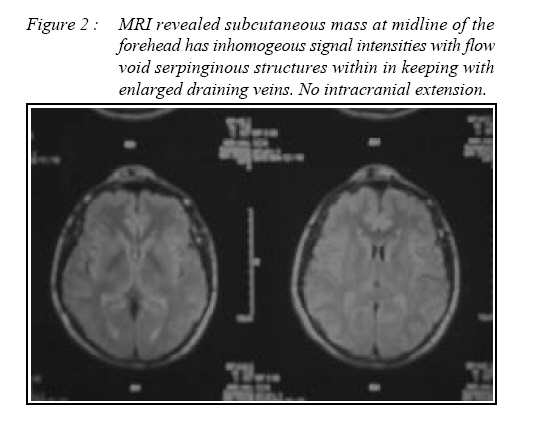
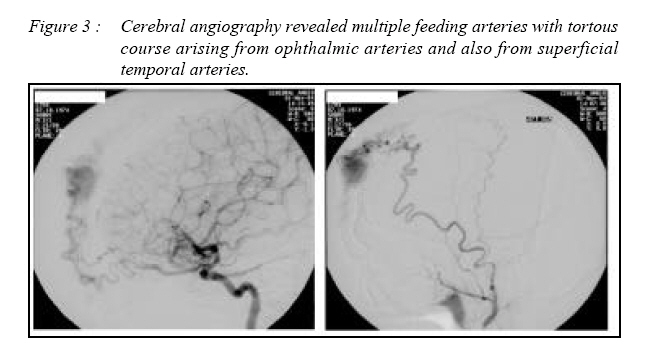
Malaysian Journal of Medical Sciences, Vol. 15, No. 3, July, 2008, pp. 55-57 Scalp arteriovenous malformation : a case report Wan Najwa Zaini Wan Mohamed, Noreen Norfaraheen Lee Abdullah, Ahmad Sobri Muda* Department of Radiology, School of Medical Sciences, Universiti Sains Malaysia, Health Campus 16150 Kubang Kerian, Kelantan, Malaysia Submitted-20-02-2005, Accepted-30-12-07 Code Number: mj08027 We report a rare case of Arteriovenous malformation (AVM) of the scalp in a 30 year-old Malay gentleman who presented with painless forehead swelling since birth. Magnetic Resonance Imaging (MRI) and cerebral angiogram performed and the findings are discussed. Key words : Scalp Arteriovenous Malformations, Subcutaneous Arteriovenous malformations, Radiological features Introduction Arteriovenous malformation (AVM) in the scalp is rare when compared with other subcutaneous or cervicofacial vascular anomalies such as the haemangioma or venous malformations. It is an abnormal fistula communication between feeding arteries and draining veins without intervening capillary bed. The draining veins can dilate and causes esthetic problem (1-3). It usually presents in late childhood, adolescent or early adulthood. It can also cause massive hemorrhages due to dryness of the overlying skin and injuries (1). In this report we describe the clinical and radiological features of a patient with a scalp arteriovenous malformation. Case Report The patient was a 30 year-old Malay gentleman who complained of a painless forehead swelling since birth, increasing in size for the past 3 – 4 years. Initially, it was a reddish small growth. The lesion bled once following trauma about a year prior to admission. The hemorrhage was secured at that time without resorted to any definitive treatment. Insidiously the forehead lesion grew in size and causing esthetic problem to him. There was no similar history in the family. On examination, there was a soft, bluish and non-tender lesion in the midline of the forehead. The overlying skin is coarse and dry; however there was neither ulceration nor active hemorrhage present (fig 1). Bruit was heard on auscultation of the lesion. The vital signs are stable and all other systems were normal. The blood investigations were unremarkable. Magnetic Resonance Imaging (MRI) of the brain revealed a predominently hyperintense subcutaneous mass in the midline of the forehead on both T1 and T2 weighted images which extends superiorly beyond forehead and inferiorly down to the root of nose. There are mulriple flow void serpinginous structures within the lesion which enhanced with contrast, in keeping with dilated vessels (fig 2). However, no MR angiography was done at that time. There was no intracranial extension. About 2 months after MRI, he underwent cerebral angiogram, which showed presence of abnormal early draining veins, in keeping with vascular malformations in the midline frontal region. Feeding arteries with tortous course appeared arising from the right ophthalmic artery with several other feeders from the left ophthalmic artery. There are also feeders also from right and left superficial temporal arteries (fig 3). No supply was noted from both anterior cerebral arteries. Enlarged early draining veins were seen draining into the scalp veins. There was no no intracranial venous drainage. He then underwent surgery for complete removal of his scalp AVM in the forehead. Discussion AVMs in scalp are relatively rare. They are 20 times more common in the brain involving or supplied by intracranial vasculature than in that from external carotid arteries (1). Cervicofacial involvement is most common in the cheeks, ears, nose, and less commonly forehead (2). Scalp AVMs are normally noticed in late childhood, adolescent or early adulthood, when substantial esthetic and social disturbance entailed, or due to various stimuli such as trauma, pregnancy or puberty (2). MRI is helpful to differentiate cervicofacial AVMs from other vascular lesions and aid in the correct diagnosis as well as to distinguish whether there is intracranial extension or involvement (3). MRI can also help to distinguish scalp AVMs which are high flow lesions from other low flow lesions such as venous or lymphatic malformations, and this will help with the treatment planning. However, catheter angiography is still the gold standard modality to understand the angioarchitecture of the lesion and to exclude any intracranial component (4). Management of scalp AVMs is difficult because of its high flow, complex vascular anatomy and cosmetic problems. There are various techniques and method of treatment for scalp AVMs. Among the treatment options include surgical excision, ligation of feeding vessels, transarterial and transvenous embolization, injection of sclerosant into the nidusand electrothrombosis (1, 5-7). Shenoy et al divided scalp AVMs into group 1 and II, to help decide the treatment of choice. Group 1 will represent primary scalp vascular malformations and Group II will represent secondary scalp venous dilatations. This patient belongs to group I representing primary scalp vascular malformations. Surgical excision is the most common and successful method of treating scalps AVMs (1). Endovascular approaches are an option as a definitive therapy or as an adjunct to surgical therapy to reduce blood loss during excision (5). The most common cause of treatment failure, even with combined embolization and surgery is incomplete resection. Recurrence has been reported as late as 18 years after complete surgical resection(4). References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08027f3.jpg] [mj08027f1.jpg] [mj08027f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}