 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 15, No. 4, October, 2008, pp. 28-34 ORIGINAL ARTICLE Knowledge, attitude and practice of sawmill workers towards noise-induced hearing loss in Kota Bharu, Kelantan. Razman Mohd Rus, Aziah Daud*, Kamarul Imran Musa, and Lin Naing** Department of Community Health and Family Medicine,
Kulliyyah of Medicine, International Islamic University Malaysia, 25200 Kuantan, Pahang, Malaysia
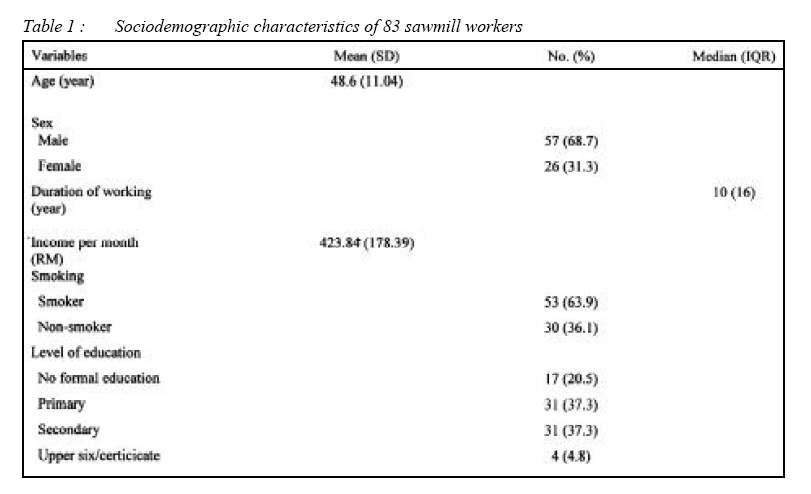
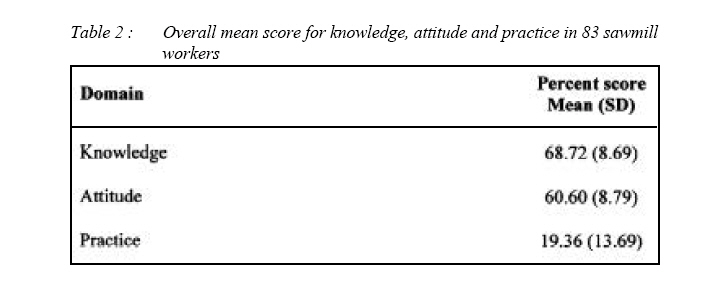
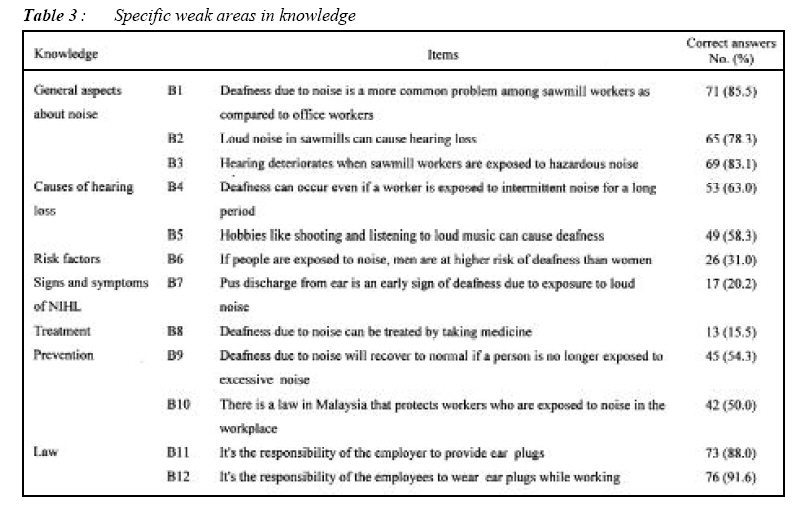
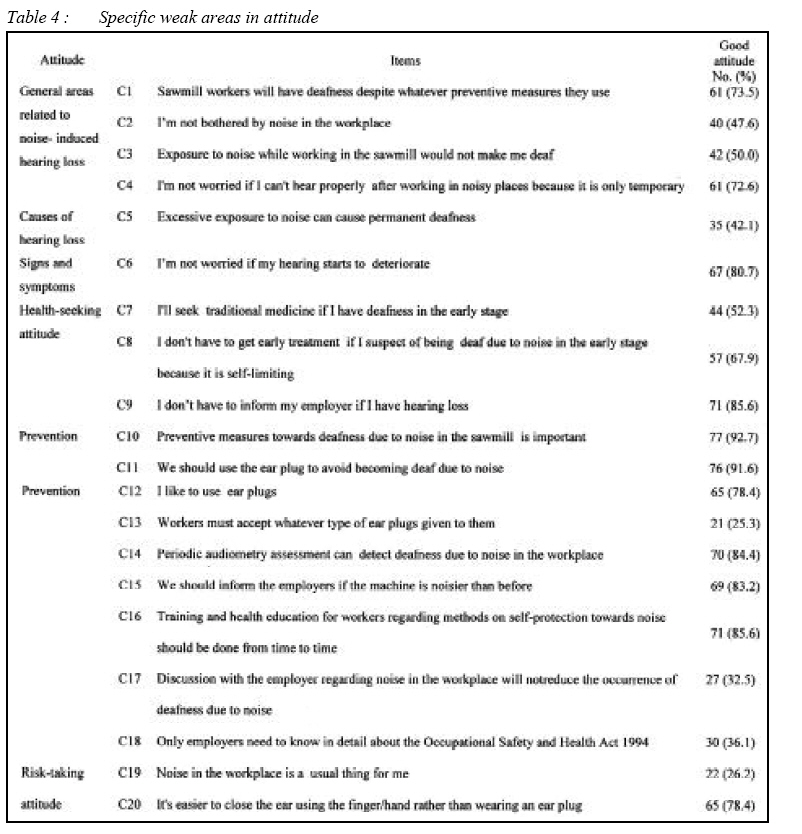
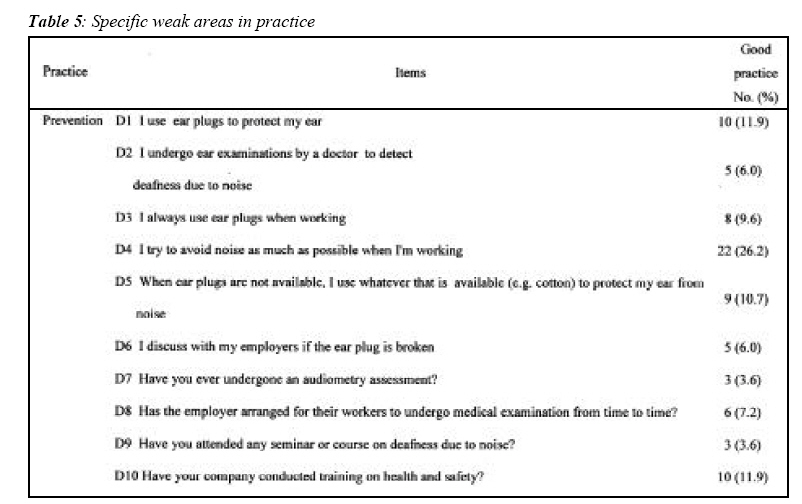
Submitted-15-06-2008, Accepted-23-10-08 Code Number: mj08036 The purpose of this study was to determine the sawmill workers’ knowledge, attitude and practice (KAP) in relation to noise-induced hearing loss (NIHL). A cross-sectional study was conducted involving 83 workers from 3 factories in Kota Bharu, Kelantan. Questionnaires were distributed to obtain the socio-demography, knowledge, attitude and practice level in relation to noise-induced hearing loss (NIHL). The weak areas identified in the knowledge section were treatment aspects (15.5%), signs and symptoms of NIHL (20.2%) and risk factors (31%). As for attitude; the prevention aspects were the lowest (25.3%), followed by risk taking attitude (26.2%), and causes of hearing loss (42.1%). Overall, the practice was not encouraging at all. It is important to have an education program to raise workers’ awareness and to improve their attitude and practices towards noise-induced hearing loss. Key words : sawmill workers, knowledge, attitude, practice, noise-induced hearing loss Introduction The average, otherwise healthy, person will have essentially normal hearing at least up to the age of 60 if his or her unprotected ears are not exposed to high noise levels, for example above 85dB (A) (1). Occupational noise is one of the most important risk factors for hearing loss in workers at most ages, ranging from 7% to 21% (averaging 16%) of the adult-onset hearing loss globally. High occupational noise exposure levels were reported in 17 studies conducted in 12 countries in South America, Africa and Asia. These high noise levels occurred in a wide range of workplaces, including manufacture of foods, fabrics, printed materials, metal products, drugs, watches and mining (2). In many countries, excessive noise is the biggest compensatable occupational hazard. The estimated costs of noise to developed countries range from 0.2% to 2% of the gross domestic product. There is a serious shortage of accurate epidemiological information on the prevalence, risk factors and costs of noise-induced hearing loss (NIHL) (3). In a study conducted among 442 noiseexposed and 83 non-noise exposed workers in the Klang Valley, although hearing protection devices were provided for 80.5% of the workers, only 5.1% wore them regularly (4). While there are multiple factors that contribute toward the occurrence of occupational NIHL, clearly lack of prevention is the main contributor. In Malaysia, under the Factories and Machinery Act 1967 (Noise Exposure Regulations 1989) (5). Part VII clearly states that the occupier shall institute a training program for, and ensure the participation of, all employees exposed to noise level at or above the action level of 85 db(A) 5. Unfortunately, till now, we do not have any information concerning the beliefs, perceptions, expectations and feelings of the workers toward the use of such protective equipment in the workplace as well as any other preventive methods like health education program. Therefore, the present study was conducted with the aim of exploring their knowledge, attitude and practice related to noise exposure in the work place. Methodology This is a cross sectional studies conducted in June 2007 involving 83 sawmill workers from Kota Bharu, Kelantan. A list of sawmills located in Kota Bharu was obtained from Kelantan State Forestry Department. Universal sampling was applied to select the study subjects. Workers working in the production section at the time of data collection were included while those who had any history of psychotic disorder, such as schizophrenia based on personal declaration and information from the employer were excluded from the study. After the workers gave their written consents, a survey was conducted using a validated self-administered questionnaire. A specifically designed questionnaire was used to gather information on socio-demographic characteristics, knowledge, attitude and practice. To test the reliability and validity, the questionnaire was piloted out of the research area so as to avoid contamination of the study population. The construct validity of the instrument was examined by using the factor analysis (principal components with Varimax rotation) revealed 3 scales; knowledge, attitude and practice. The internal consistency was evaluated using Cronbach’s alpha coefficients for each scale. Cronbach’s alpha for knowledge, attitude and practice was 0.67, 0.92 and 0.75 respectively. Data collection was carried out after obtaining approval from the Research and Ethics Committee, Health Campus, USM. Development of questionnaire The Noise-Induced Hearing Loss questionnaire was developed in stages. The first stage involved reviewing the literature on knowledge, attitude and practice related to noise and also searching the guidelines on noise exposure in the workplace. In the second stage, a focus group discussion was held involving six workers and two supervisors which lasted for one and a half hours. The purpose of this discussion was to identify their beliefs, expectations and feelings related to noise exposure in the workplace. The session was recorded and videotaped. In the third stage, a workshop was conducted to determine the areas (scope) and select relevant items to be included in the questionnaire. The wordings and word phrases were discussed in detail and rephrased in the Malay language. These steps were vital in order to ensure a good content validity as well as to identify the subdomains to be covered in the KAP questionnaire. The demographic data comprised of age, sex, duration of working in the sawmill, smoking status, educational level and total family income. Section 2, 3 and 4 include the knowledge, attitude and practice of the workers respectively. General aspects about noise, problems in the workplace, causes of hearing loss, risk factors, signs and symptoms of noise-induced hearing loss, treatment, prevention and law were included in the knowledge section. The attitude section includes the general areas related to noise induced hearing loss, causes of hearing loss, signs and symptoms, health seeking attitude, prevention, law and risk-taking attitude. The practice section includes practising prevention and laws. Categorical responses (true, false and don’t know) were used for the knowledge section. As for the attitude items, the responses were recorded using the Likert scale 6, ranging from 1 (strongly disagree) to 4 (strongly agree) and as for practice, the responses were never, seldom, frequent and always. These responses were then converted into scoring. Total score was calculated for each knowledge, attitude and practice domain. Then, each total raw score was transformed into ‘percent score’ by dividing the score with the possible maximum score, and multiplying by 100. Based on the discussion among the occupational health experts during the development of the questionnaire, a cut off level of 75% was considered to be satisFactories. Those who scored less than these cut off points, were considered to have inadequate knowledge, poor attitude and poor practice, and thus recommended for further health education intervention. The questionnaire consists of 42 items; 12 items for knowledge (7 subdomains), 20 items for attitude (6 subdomains) and 10 items for practice (1 subdomain). Statistical Analysis The data were analysed using SPSS version 12 software (7). Descriptive statistics on sociodemography was expressed as means and standard deviations (SD) or medians and interquantile ranges (IQR) for numerical variables; frequencies and percentage (%) were used for categorical variables. The KAP scores were compared by using mean (SD) and 95% confidence interval (CI). Mean (SD) for each item of the KAP was analysed and the proportions of respondents who correctly answered each item of the KAP were expressed as the correct percentages. Ethical approval The research proposal was approved by the Department of Community Medicine in October, 2005. The Research and Ethics Committee, School of Medical Sciences, Health Campus, Universiti Sains Malaysia, later approved this study on the 1st of August 2006. Results A total of 83 sawmill workers participated in this study. The study involved mostly Malay workers with mean age of 48.6 (SD 11.04) years. More than half (68.7%) of the workers were male and out of this, 63.9% were smokers (average of 4 cigarettes per day). Median duration of employment was 10 years (IQR 16.00) and earning an average of RM 423.84 (SD RM 178.39) per month (Table 1). Overall mean score for knowledge, attitude and practice is shown in Table 2. Specific areas that were found to be weak in knowledge (Table 3) were treatment aspects (15.5%), signs and symptoms of NIHL (20.2%), risk factors (31%), law regarding noise exposure in the workplace (50%), preventive aspects (54.3%) and causes of hearing loss whereby two items scored only 58.3% and 63%. Table 4 shows the weak areas identified in the attitude section. Specific areas that were found to be weak were on prevention (lowest was 25.3%), risk-taking attitude (26.2%), causes of hearing loss (42.1%), health seeking attitude (52.3%) and some components in the general areas related to noiseinduced hearing loss (47.6% and 50%). The weak areas identified in the practice section were shown in Table 5. The weakest practices were the audiometry assessment and seminar or courses attended. Surprisingly only 3.6% claimed that they had audiometry assessments done and attended seminars. Discussion In general, the overall mean knowledge and attitude scores were below satisfactory level (Table 2), and the mean practice score was remarkably low. Most of the items in this section were related to preventive measures with regard to NIHL. Therefore, in reality this reflects that their practice was actually poor. Three specific areas that were found to be weak in knowledge were on the treatment of noiseinduced hearing loss whereby only 15.5% of the workers managed to get correct answers. Here, the question examined the respondent’s knowledge on whether noise- induced hearing loss can be treated by only taking medicine. Majority of them thought it could be cured by just taking medicine but unfortunately the condition is irreversible. Having this incorrect information may lead them to ignore the seriousness caused by hazardous noise on their hearing capabilities and continuous exposure to loud noise. This was followed by signs and symptoms of NIHL. Nearly 80% of the workers thought that pus discharge is one of the signs of noise-induced hearing loss. In reality, pus discharge would mean infection of the ear. Signs to suggest noise-induced hearing loss include: difficulty in understanding spoken words in a noisy environment, need to be near or look at the person speaking to help understand words, familiar sounds are muffled, complaints that people do not speak clearly and ringing noise in the ears (8). Only 31% of the sawmill workers knew that men and women had the same risk if both were exposed to loud noise. Factors that influence whether hearing loss can occur in exposed individuals are: age, genetics and race; which belongs to the nonmodifiable risk factors. The modifiable risk factors include cigarette smoking, lack of exercise, presence of diabetes mellitus, and use of drugs such as aminoglycosides (9). In addition, the characteristics of the sound such as; sound intensity, duration and individual susceptibility to noise-induced hearing loss (10) also play major roles. Hearing loss is not taken seriously by many workers because it is not a dramatic life threatening illness or injury as it occurs gradually, not visible and has uncertain time course. People who develop NIHL are usually unaware their hearing are affected until the loss are quite significant 11 Three weakest areas in attitude were on prevention (lowest was 25.3%), risk-taking attitude (26.2%) and causes of hearing loss (42.1%). This could be attributed to lack of advice and guidance on the risk from loud noise and knowledge on the function of the ear. Perhaps developing positive attitudes and behaviors toward hearing loss prevention program is more effective the earlier it begins (12). The weakest practices were the audiometry assessment and seminar or courses attended. Surprisingly only 3.6% claimed that they had an audiometry assessment done and attended seminars. Although Malaysia has the Occupational and Safety Health Act 1994 and the Noise Regulation 1989 under the Factories Machinery Act 1967, this is seldom enforced. WHO reported that developing countries often lack both effective legislation against noise and program to prevent noise-induced hearing loss 3. Despite 26.2 % of the workers claimed that they tried to avoid being exposed to noise as much as possible when thay are working only 11.9% of them used ear plugs. Although it is a reported practice, it is higher than those reported in the study by Maisarah and Said whereby only 4.1 % of exposed Factories workers used hearing protection devices. Reasons for not wearing include discomfort, and most importantly, the danger of not using it is not apparent (4). Over reliance on hearing protectors alone to reduce noise exposure among sawmill workers might not be an appropriate strategy due to the fact that hearing protection devices (HPD) is often ignored in tropical countries because of the hot and humid climate conditions, which make the use of this device impractical (13). We therefore conclude that an educational program to educate the workforce in order to improve their knowledge, attitude and practice towards noise in the workplace is very much needed. References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08036t4.jpg] [mj08036t3.jpg] [mj08036t2.jpg] [mj08036t5.jpg] [mj08036t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}