 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 15, No. 4, October, 2008, pp. 48-55 ORIGINAL ARTICLE Functional outcome at 6 months in surgical treatment of spontaneous supratentorial intracerebral haemorrhage (SICH). Abdul Rahman Izaini Ghani, John Tharakan Kalappurakkal John, Zamzuri Idris, Mazira Mohamad Ghazali, Nur-Leem Murshid, Kamarul Imran Musa*. Department of Neurosciences, *Department of Community Medicine,
School of Medical Sciences, Universiti Sains Malaysia, Health Campus,
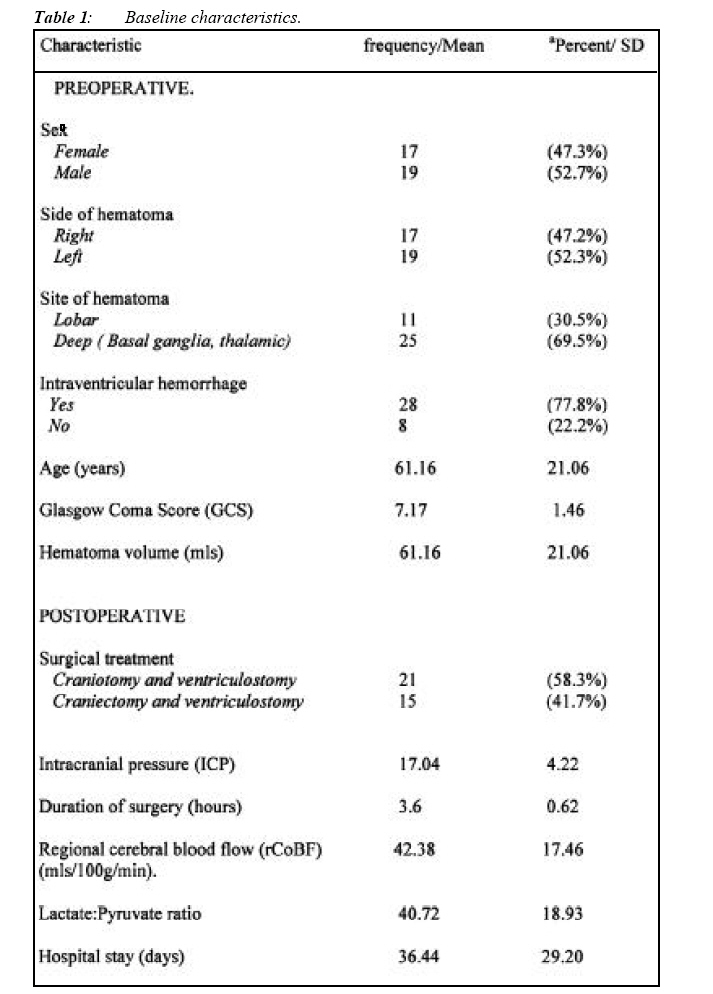
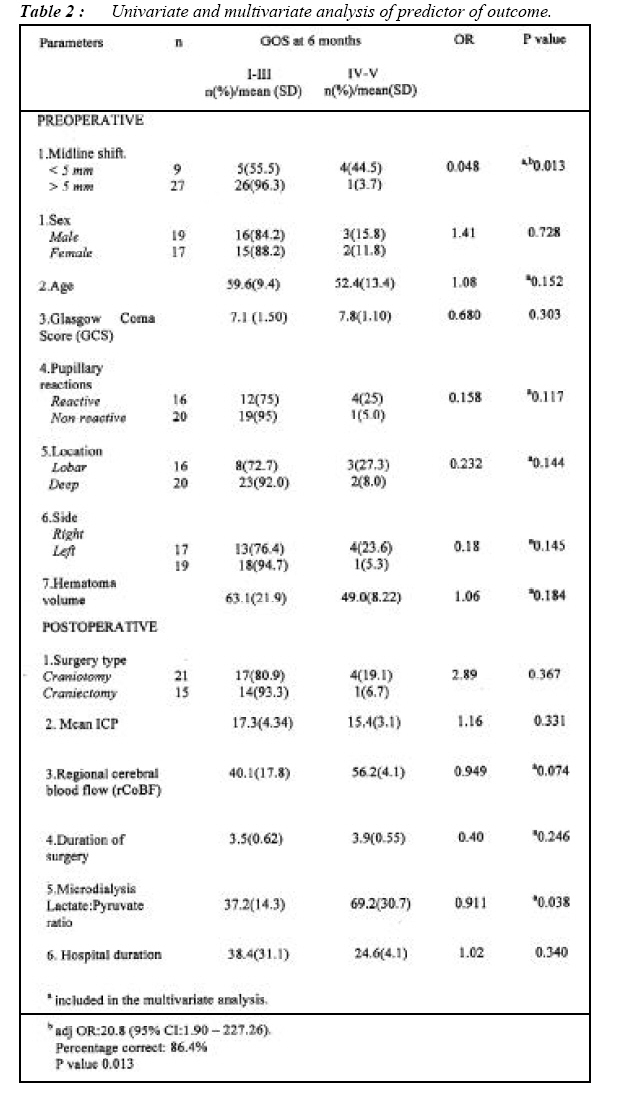
16150 Kubang Kerian, Kelantan, Malaysia Submitted-15-06-2008, Accepted-23-10-08 Code Number: mj08039 A prospective cohort study was done to evaluate the role of surgery in patients with spontaneous supratentorial intracerebral haemorrhage (SICH) and to identify predictors of outcome including the use of invasive regional cortical cerebral blood flow (rCoBF) and microdialysis. Surgery consisted of craniotomy or decompressive craniectomy. The ventriculostomy for intracranial pressure (ICP) monitoring and drainage and regional cortical cerebral blood flow (rCoBF) and microdialysis were performed in all subjects. Pre and post operative information on subjects were collected. The study end points was functional outcome at 6 months based on a dichotomised Glasgow Outcome Scale (GOS).The selected clinical, radiological, biochemical and treatment factors that may influence the functional outcome were analysed for its significance. A total of 36 patients were recruited with 27(75%) patients had Glasgow Coma Score (GCS) between 5 to 8 on admission and 9(25%) were admitted with GCS of 9. At 6 months, 86 % had a poor or unfavorable outcome (GOS I-III) and 14% had good or favorable outcome (GOS IV-V). The mortality rate at 6 months was 55%.Univariate analysis for the functional outcome identified 2 significant variables, the midline shift (p=0.013) and mean lactate:pyruvate ratio (p=0.038). Multivariate analysis identified midline shift as the single significant independent predictor of functional outcome (p=0.013).Despite aggressive regional cortical cerebral blood flow (rCoBF) and microdialysis study for detection of early ischemia, surgical treatment for spontaneous intracerebral hemorrhage only benefited a small number of patients in terms of favorable outcome (14%) and in the majority of patients (86%), the outcome was unfavorable. Patients with midline shift > 5mm has almost 21 times higher chances (adj) OR 20.8 of being associated with poor outcome (GOS I-III). Key words : intracerebral haemorrhage, regional cortical cerebral blood flow (rCoBF), surgery, Glasgow Outcome Scale. Introduction Intracerebral hemorrhage (ICH) is a common devastating neurological event that causes high morbidity and mortality with profound economic complication. Unlike the declining mortality with subarachnoid hemorrhage due to improvements in surgical and critical care techniques, the morbidity and mortality of ICH have remained relatively unchanged throughout the past several decades. It is associated with the highest mortality rate, with only 38% of affected patients surviving the first year (1).The role of medical and surgical treatment in ICH continues to be controversial. Studies of surgical hematoma evacuation in ICH using a variety of methods have yielded either negative or inconclusive results (2). Likewise, no medical treatment has been shown conclusively to benefit patients with ICH. This study is the first prospective cohort study in Malaysia assessing the role of surgery in the treatment of spontaneous supratentorial intracerebral hemorrhage in combination with best medical therapy in a selected group of patients meeting the inclusion and exclusion criteria for the study. This study was also conducted to identify associated clinical, radiological, biochemical and treatment factors that could significantly determine functional outcome following surgical therapy for ICH. The objective of the study was to evaluate the role of surgery in the treatment of spontaneous supratentorial intracerebral hemorrhage and to identify and quantify important and significant clinical, radiological, biochemical and treatment factors that determined the functional outcome. Materials and Methods 36 patients who presented to the Hospital University Sains Malaysia were recruited into the study between February 2004 for a period of 1 year. Patients were eligible for inclusion if consent or assent was obtained from the relatives, evidence of spontaneous supratentorial intracerebral hemorrhage (ICH) was present on the initial CT brain, Glasgow Coma Score (GCS) 5-12 with obvious hemiplegia or disturbed consciousness, CT brain with hematoma volume >30 mls and/or evidence of mass effect based on midline shift at the level of third ventricle, features of herniation, and if they were young patients with a moderate to large lobar hemorrhage who were clinically deteriorating. The patients were excluded if clear evidence that the hemorrhage was due to an aneurysm and/or angiographically proven arteriovenous malformation (AVM), intracerebral hemorrhage secondary to trauma or tumor, cerebellar or brainstem hemorrhage, severe preexisting physical or mental disability that the patient was not independent through a 24 hour period prior to the ictus, and severe co-morbidity (e.g malignant disease, severe heart, lung or endocrine disease) which might interfere with the assessment of the outcome. The CT brain scan was performed using Siemens Somatoform 4 scanner. Axial slices of 3.75 mm for infratentorial cut and 7.5 mm for supratentorial cut were done parallel to the orbitomeatal line from the base of the skull up to the vertex. In each patient, the presenting symptoms and duration of ictus prior to admission were recorded. The neurological status on admission to the Department of Neurosciences registered as level of consciousness according to the Glasgow Coma Score (GCS) which incorporated measures of the best motor, verbal response and eye opening and the presence of normal or pathological pupillary light reaction. The classification of haematomas location was based on the location of the epicenter of the haematomas and was divided into whether the hematoma is lobar (frontal, temporal, parietal or occipital) or deep location (putaminal, basal ganglia, internal capsule or thalamic). The volume of the hematoma was calculated based on the recommendation by Kothari et al (3) by calculating the volume of the high absorption lesion. The associated intraventricular hemorrhage and degree of midline shift at the level of third ventricle were measured and recorded. All patients were operated within 72 hours of admission through an open craniotomy and hematoma evacuation by the author. Timing of surgery was divided into early surgery less than 24 hours or delayed surgery. In selected cases, in which a progression in brain swelling was expected to occur after the hematoma evacuation, a decompressive craniectomy and dural enlargement was performed. A thin microdialysis catheter (diameter of 0.62 mm) with a dialysis membrane at its tip was implanted into the brain tissue adjacent to the evacuated hematoma, the so called perihemorrhagic area. The catheter was perfused with a physiological solution, which passes through a semipermeable membrane at the tip, across which soluble small molecules in the extracellular space can diffuse into the catheter. Samples were collected continuously and were analysed immediately at the bedside for glucose, lactate and pyruvate.The microdialysis catheter was used to monitor the brain chemistry and pathophysiological changes in chemical process associated with ischemia defined by an abnormal lactate:pyruvate ratio of > 25 and was kept for the duration of 3 to 5 days. The Saber 2000 thermal diffusion flowmetry (TDF) sensor for the measurement of regional cortical blood flow (rCoBF) were positioned in contact with the gyral surface under the dura ipsilateral to the evacuated intracerebral hematoma and was kept for 3 days. Pathological tissue, large vascular channels and deep sulci were avoided. Data collection for regional cortical blood flow (rCoBF) was performed hourly. All patients in the study had a ventricular catheter inserted for intracranial pressure (ICP) monitoring and hourly recording of ICP was recorded. Postoperatively, all patients were admitted to the intensive care unit and were provided with best and appropriate medical therapy. The patients’ outcome were studied prospectively with a clinical follow-up at 1, 3, and 6 months at our out-patient clinic. For those patients who were unable to attend the interview because of severe disability, consultation with their family or caregiver was made over the telephone. The Glasgow Outcome Scale as described for head injuries was used. This scale classified patients into one of five mutually exclusive categories defined as 1) dead, 2) vegetative state (no social or relational interaction), 3) severely disabled (dependant on others for the activities of daily living but capable of social interaction), 4) moderately disabled (independent but objectively or subjectively disabled), 5) good recovery (capable of returning to the former level of function even with a minor deficit). This clinical outcome was divided into good or favorable outcome where patients made a good recovery or were disabled but independent (GOS IV and V) and poor or unfavorable outcomes (GOS I, II, III). Data analysis was completed using commercially available software SPSS, version 11 (SPSS, Inc) Chicago, IL. At univariate level, the chi square test and independent t-test was used to determine the functional outcome at 6 month based on Glasgow Outcome Scale in relation to different variables of the patients. At multivariate level, the multiple binary logistic regression analysis was used to determine variables associated with poor functional outcome. At univariate level, variables with p value < 0.25 and clinically important variables in the univariate analysis were included in the modeling using forward likelihood method. Results with p value < 0.05 were considered significant. Results The baseline characteristics of the patients preoperative and postoperatively is presented in Table 1. A total of 36 patients with the diagnosis of spontaneous supratentorial intracerebral hemorrhage were recruited in the study. Of this group, 19 patients were male (52.8%) and 17 (47.2%) were female. The age of the patients ranges from 39 to 76 years old with a mean age of 61.1 years old. The age distribution showed the majority of the patients were in the 5th to 7th decade. Overall age distribution showed that 50% of the patients aged above 60 years old. The patient’s GCS on admission ranged from 5 to 9. Seven (19.4%) patients had GCS of 5, five (13.9%) patients presented with GCS of 6, eight (22.2%) patients with GCS of 7, seven (19.4%) with GCS of 8 and nine (25%) had GCS of 9. Overall, 27 (75%) of patients were admitted with GCS less than 8 and nine (25%) were admitted with GCS more than 8. In relation to pupillary reaction, 16 (44.4%) of patients had normal or reactive pupils and 20 (55.6%) of patients had an abnormal or non-reactive pupils. In all patients, the CT scan of the brain was performed. The CT scan finding showed that 19 (52.3%) cases of hematoma were located on the left side and 17 (47.2%) of hematoma were located on the right side. With respect to hematoma location, 25 (69.5%) hematomas were located in deep location (basal ganglia, putaminal or thalamic) and 11 (30.5%) cases were lobar. The volume, using the Kothari method, varied from 40 ml to 125 ml, with a median volume of 55 mls and mean volume of 61.2 mls (±21.06). Categorically, 21(58.2%) cases of hematoma had a volume more than 50 mls and and 15 (41.6%) cases had a volume of less than 50 mls. In 28 (77.8%) cases there were an associated intraventricular hemorrhage and in 8 cases (22.2%) no intraventricular hemorrhage was observed. Midline shift more than 5 mm measured by displacement of third ventricle were recorded in 27 (75%) cases. In 9 (25%) of cases, the midline shift were recorded between 0 to 5 mm. All patients in the study were treated surgically. Craniotomy was performed in 21 (58.3%) patients and decompressive craniectomy was performed in 15 (41.7%) patients. With respect to timing of surgery, 22 (61.1%) patients were operated within 24 hours from the ictus and 14 (38.9%) were operated between 24 and 72 hour from the ictus. The mean surgical duration was 3.6 hours. The ventriculostomy for intracranial pressure (ICP) monitoring were performed in all patients. In patients with persistent intracranial hypertension with an ICP value exceeding 20 mmHg, drainage of intraventricular blood or CSF was performed to ensure that the ICP is kept below 20 mmHg. The Microdialysis catheter was implanted in all patients for the analysis of lactate: pyruvate ratio. 23 (63.9%) patients had an abnormal lactate: pyruvate ratio, 4 (11.1%) had a normal ratio and in 9 (25%) cases, the lactate: pyruvate ratio was not analysed due to inadequate dialysate sample collection. In the poor outcome group, the mean lactate: pyruvate ratio was 32.7and 69.2 in the good outcome group. With respect to assessment of regional cerebral blood flow (rCoBF), the good outcome group recorded a mean rCoBF of 56.2 compared to the poor outcome group with a mean rCoBF of 40.1. Final outcome revealed that 31 (86.1%) patients had poor or unfavorable final outcome and 5 (13.9%) had good or favorable outcome at 6 months based on dichotomized GOS. At 6 months follow-up, 16 patients were still alive, indicating the survival rate of 45%. The mortality rate at 1, 3 and 6 months were 33%, 42% and 55% respectively. The univariate analysis of the relation between various variables and Glasgow Outcome Scale (GOS) at 6 months revealed 2 significant variables in determining the outcome. They are the midline shift and lactate: pyruvate ratio with the p value of 0.013 and 0.038 respectively. The results for significant and non-significant variables are shown in Table 2 respectively. The binary logistic regression analysis was performed to identify the significant variables in relation to functional outcome. Initially all the variables with p <0.250 and clinically important variables were included in the model. The variables with p <0.250 were midline shift (p=0.013), mean lactate: pyruvate ratio (p=0.038), age (p=0.152), papillary reactions (p= 0.117), hematoma location (p=0.144), hematoma volume (p=0.184), GCS (p=0.303), regional cerebral blood flow (rCoBF) (p=0.074), duration of surgery (p=0.246) and side of hematoma (p=0.167). The binary logistic regression analysis showed that the only significant predictor of functional outcome in this study was the midline shift (OR=20.8; 95% CI = 1.90-227.26; p=0.013). It showed that patients with midline shift >5mm has almost 21 times higher chances of being associated with poor or unfavorable outcome. Discussion This prospective study on survival analysis and functional outcome in patients who were treated surgically for spontaneous intracerebral hemorrhage showed an overall mortality at 1, 3 and 6 months to be 33%, 42% and 55% respectively. The patients status at 6 months showed that 20 (55.6%) patients had GOS I, 1 (2.8%) patient had GOS II, 10 (27.7%) patients had GOS III and 5 (13.9%) had GOS of IV. None of the patients in this study had GOS of V. In term of functional outcome at 6 months based on dichotomized Glasgow Outcome Scale (GOS), 5 out of 36 patients (13.9%) had a favorable outcome and in the remaining, 31 out of 36 patients (81.9%) had an unfavorable outcome. At 6 months, 16 patients were still alive indicating a survival rate of 45%.It is worthwhile to mention that the groups of patients in this study were mainly ‘ill patients’ with poor neurological status on admission, had GCS score on admission ranges from 5 to 9. The finding of this study parallels with many previous studies including randomized and non-randomized studies assessing the role of surgery in intracerebral hemorrhage with a reported mortality and morbidity at 6 months between 50 and 95% (4 - 7). Similar result was also found in the STICH study by Mendelow and colleagues (4). This study was the largest prospective randomized trial whose goal was to compare early surgery with initial conservative treatment. This study also found the uniformly poor outcome in patients presenting with intracerebral hemorrhage in coma. In those with initial Glasgow Coma Score of eight or below, nearly all were classified as having unfavorable outcomes. Early surgery raised the relative risk of poor outcome for these patients by 8%. In comatose patients, surgery is probably harmful and it is estimated that 40 operations would be required to achieve one more favorable outcome in this group of patients. With regard to radiological variables based on CT imaging, we observed a significant association between midline shift in relation to functional outcome and survival time. The midline shift was found to be an important outcome predictor in both univariate and multivariate analysis. In the multivariate analysis by logistic regression analysis, this study found that midline shift as the only significant predictor of functional outcome (p=0.013). Any patient with a midline shift >5mm had almost 21 times higher chances of being associated with poor or unfavorable outcome (p=0.013; OR 20.8; 95% CI 1.90 – 227.26). This finding was consistent with other studies that also identified significant association between the midline shift with functional outcome (8, 10). Many other studies also found that the hematoma volume to be predictive of outcome and survival (10 - 13). In our study, the hematoma volume was not a significant predictor of outcome. However, it appeared that the poor outcome group had a higher hematoma volume (63.1) compared to the good outcome group (49.0). The correlation between the hematoma volume and outcome was not detected in our study probably due to small number of patients in our study. In some studies of supratentorial ICH (9, 14, 15), measurements of hematomas suggested that a critical volume of 4050 mls separates patients of the bad from those of the good prognostic groups. In our study, the intracerebral hematoma was surgically evacuated either by craniotomy or craniectomy. This study found no significant difference in functional outcome (p=0.367) when this type of surgery were compared. Other investigators (16, 17) have also evaluated the role of decompressive craniectomy in the treatment of spontaneous intracerebral hemorrhage. Maira et al (17) on the other hand, found a statistically significant difference on functional outcome in patients who had decompressive craniectomy compared to patients who only had a craniotomy for hematoma evacuation. The differences in outcome between this study and our study which showed the majority of patients (81.9%) had a poor final outcome is attributed to differences in other prognostic factors that determines outcome in intracerebral hemorrhage such as hematoma volume, location of hematoma and evidence of mass effect or herniation. One of the contrasting patient’s characteristic compared to our study is the hematoma volume, whereby 84% of their patients had a hematoma volume of < 50 mls. In our study, only 42% of our patients had a hematoma volume < 50 mls. This is the first study that attempted to identify the correlation between regional cerebral blood flow monitoring in patients with ICH in relation to functional outcome. This study demonstrated that the patients with good functional outcome recorded a higher rCoBF (56.2 ml/100g/min) compared to the poor outcome group (40.1 ml/100g/min). Our study of rCoBF in patients with intracerebral hemorrhage was consistent with the study by Lee (18) and Sioutos (19) where 4 out of 8 patients (50%) with mean rCoBF value of >50 ml/100g/min had a good functional outcome compared to only 1 out of 24 patients (4%) with mean rCoBF <50 ml/100g/min had a good functional outcome. However, this is not statistically significant (p=0.074).The possible explanation for this is probably due to relatively small sample size and other more established factors that determine the outcome such as midline shift, initial GCS and hematoma volume. With respect to the microdialysis study represented by an analysis of mean lactate:pyruvate ratio, this study showed that the good outcome group appeared to have a higher mean lactate:pyruvate ratio (69.2) compared to the poor outcome group (37.2). However both groups demonstrated a higher mean lactate:pyruvate ratio (i.e value more than 25 suggest evidence if ischemia). However, this study did not suggest that higher mean lactate:pyruvate ratio is associated with good outcome. We suggest a better design study with bigger sample size to hopefully show the effect of lactate:pyruvate ratio that uses the cut off ratio of 25 in order to differentiate between good and poor outcome group. Finally, the identification of prognostic factors that determine the patient’s outcome would assist the attending physician to decide on the best therapy for the patient and providing them with an evidencebased knowledge regarding this disease. Acknowledgements Dr. Abdul Rahman Izaini Ghani’s publication is part of the partial fullfillment for the Master of Surgery (Neurosurgery) USM Programme. References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08039t1.jpg] [mj08039t2.jpg] |
| |||||||||

{kind=link}
{kind=link}