 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 15, No. 4, October, 2008, pp. 56-67 ORIGINAL ARTICLE Delayed traumatic intracranial haemorrhage and progressive traumatic brain injury in a major referral centre based in a developing country Toh Charng Jeng , Mohd Saffari Mohd Haspani*, Johari Siregar Adnan**, Nyi Nyi Naing*** Department of Neurosciences, School of Medical Science, Universiti Sains Malaysia, Health Campus,
16150 Kubang Kerian, Kelantan, Malaysia & Unit Neurosurgery, Department of Surgery, Hospital,
Universiti Kebangsaan Malaysia, Jalan Yaacob Latif, Bandar Tun Razak, 56000 Cheras, Kuala Lumpur,
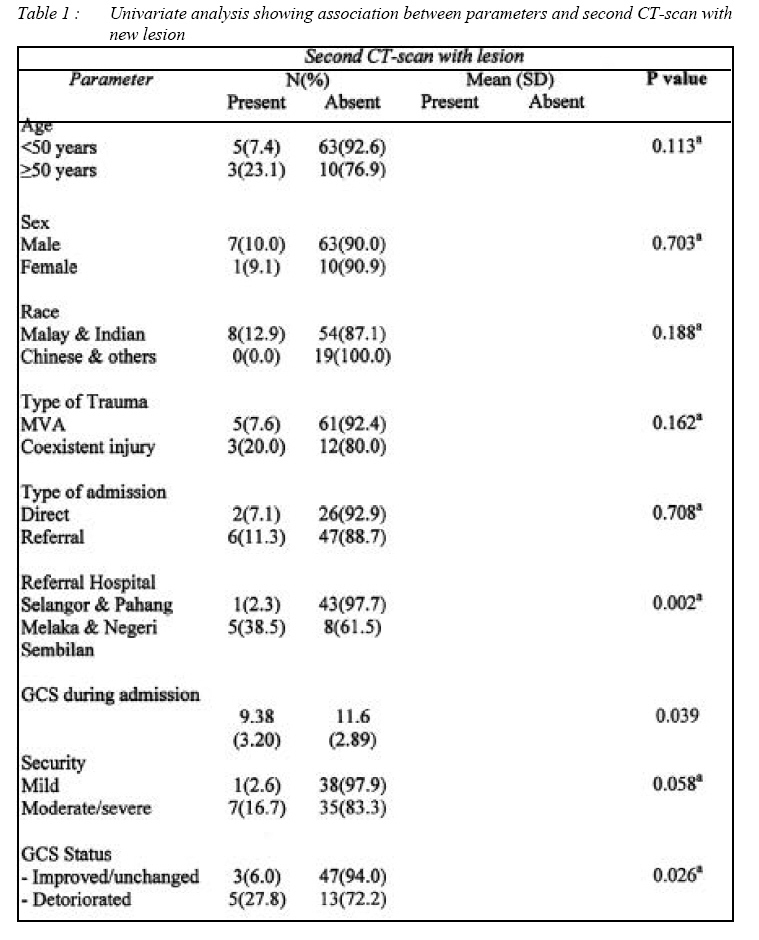
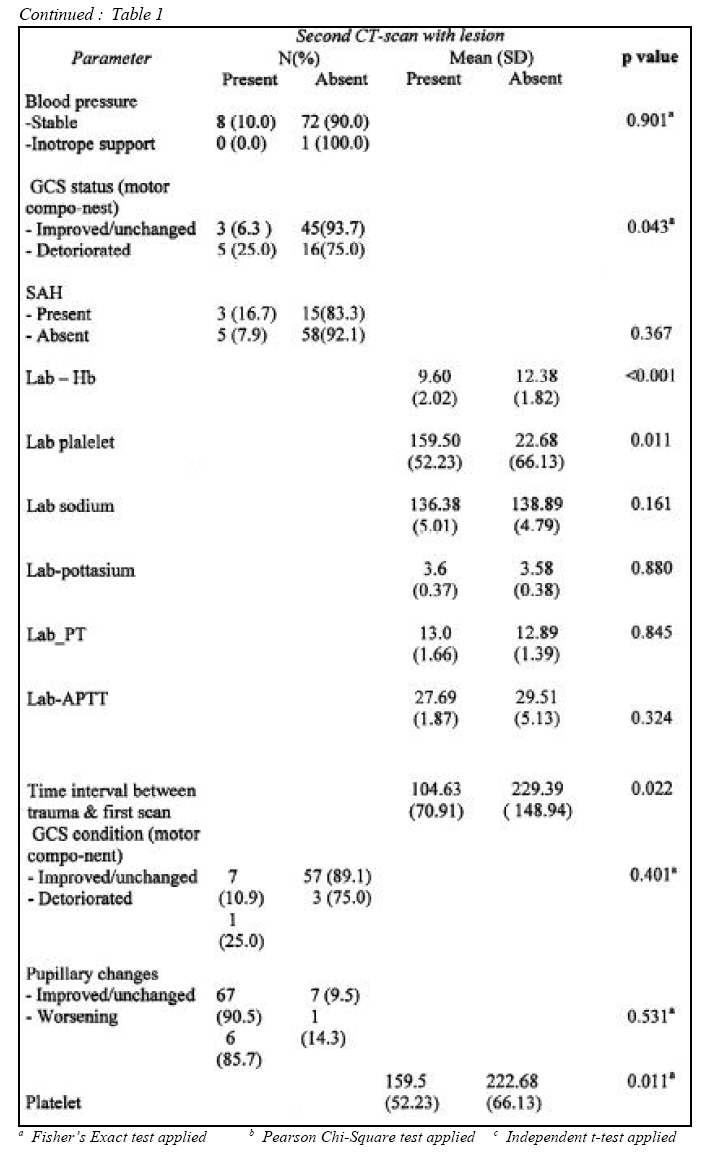
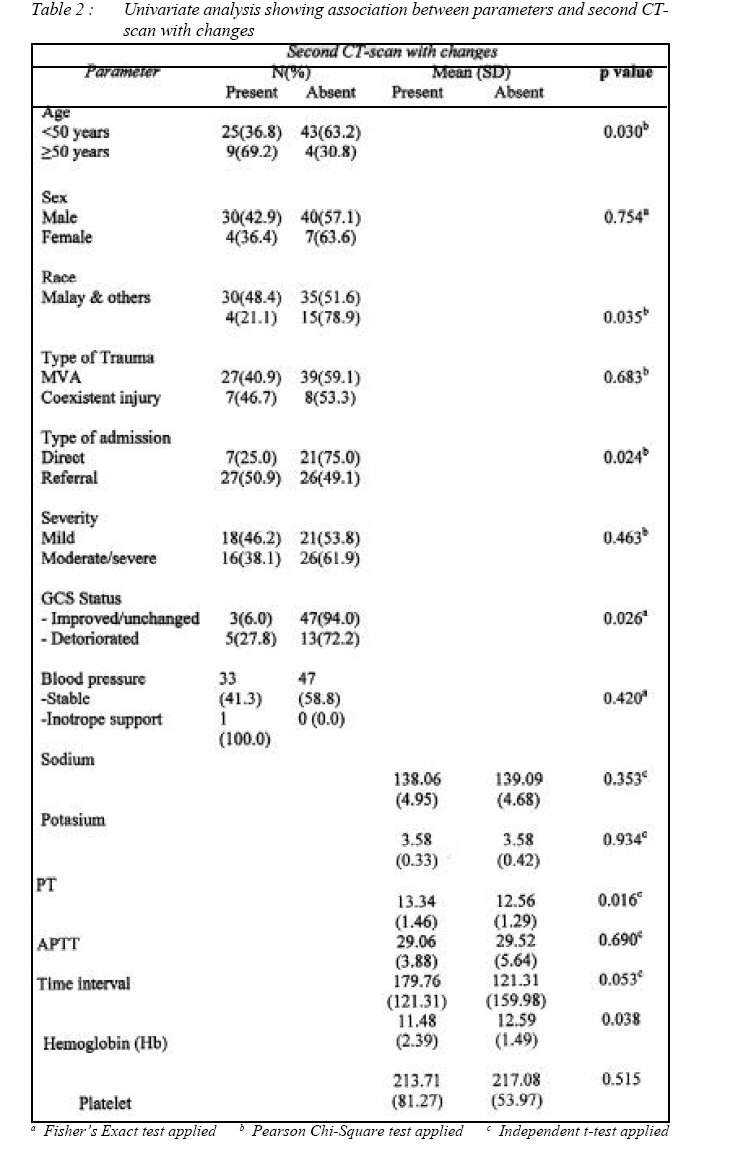
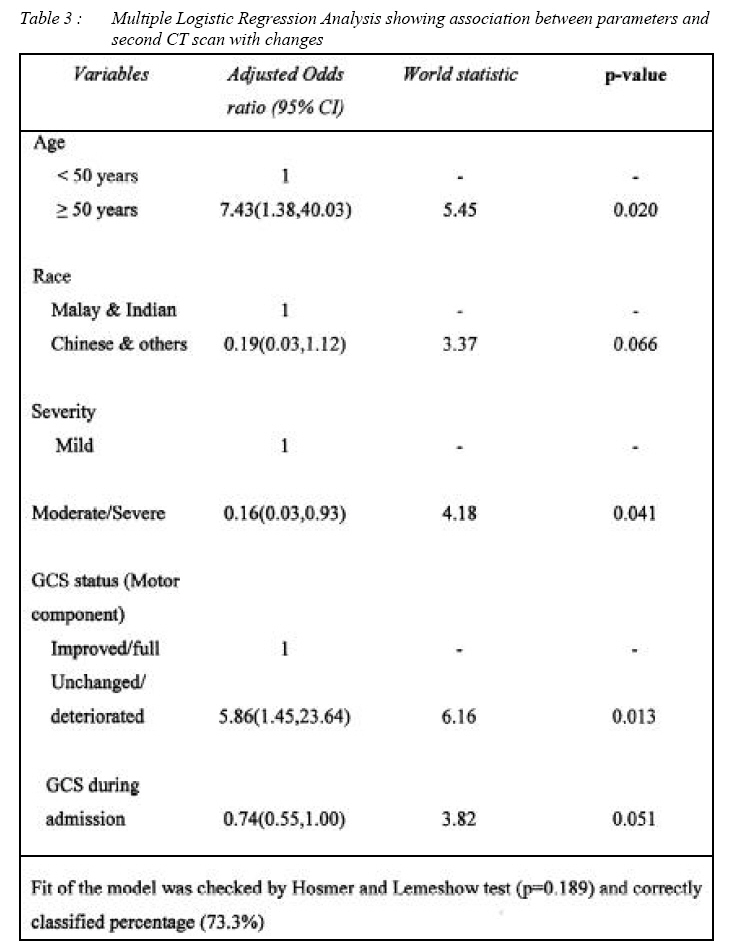
Malaysia. Submitted-15-06-2008, Accepted-23-10-08 Code Number: mj08040 A repeat Computer Tomographic (CT) brain after 24 -48 hours from the 1st scanning is usually practiced in most hospitals in South East Asia where intracranial pressure monitoring (ICP) is routinely not done. This interval for repeat CT would be shortened if there was a deterioration in Glasgow Coma Scale (GCS) most of the time the prognosis of any intervention may be too late especially in hospitals with high patient to doctor ratio causing high mortality and morbidity. The purpose of this study was to determine the important predictors for early detection of Delayed Traumatic Intracranial Haemorrhage (DTICH) and Progressive Traumatic Brain Injury (PTBI) before deterioration of GCS occurred as well as the most ideal timing of repeated CT brain for patients admitted in Malaysian hospitals. A total of 81 patients were included in this study over a period of six months. The CT scan brain were studied by comparing the first and second CT brain to diagnose the presence of DTICH/PTBI. The predictors tested were categorized into patient factors, CT brain findings and laboratory investigations.The mean age was 33.1 ± 15.7 years with a male preponderance of 6.36:1. Among them, (81.5%) of them were patients from road traffic accidents with Glasgow Coma Scale ranging from 4 – 15 (median of 12) upon admission. The mean time interval delay between trauma and first CT brain was 179.8 ± 121.3 minutes for the PTBI group. The DTICH group, (9.9%) of the patients were found to have new intracranial clots. Significant predictors detected were different referral hospitals (p=0.02), total GCS status (p=0.026), motor component of GCS (p=0.043), haemoglobin level (p<0.001), platelet count (p=0.011) and time interval between trauma and first CT brain (p=0.022). In the PTBI group, (42.0%) of the patients were found to have new changes (new clot occurrence, old clot expansion and edema) in the repeat CT brain. Univariate statistical analysis revealed that age (p=0.03), race (p=0.035), types of admission (p=0.024), GCS status (p=0.02), pupillary changes (p=0.014), no. of intracranial lesion (p=0.004), haemoglobin level (p=0.038), prothrombin time (p=0.016) as the best predictors of early detection of changes. Multiple Logistics regression analysis indicated that age, severity, GCS status (motor component) and GCS during admission were significantly associated with second CT scan with changes. This study showed that 9.9% of the total patients seen in the period of study had DTICH and 42% had PTBI. In the early period after traumatic head injury, the initial CT brain did not reveal the full extent of haemorrhagic injury and associated cerebral edema. Different referral hospitals of different trauma level, GCS status, motor component of the GCS, haemoglobin level, platelet count and time interval between trauma and the first CT brain were the significant predictors for DTICH. Whereas the key determinants of PTBI were age, race, types of admission, GCS status, pupillary changes, number of intracranial bleed, haemoglobin level, prothrombin time and of course time interval between trauma and first CT brain. Any patients who had traumatic head injury in hospitals with no protocol of repeat CT scan or intracranial pressure monitoring especially in developing countries are advised to have to repeat CT brain at the appropriate quickest time . Key words : delayed, intracranial, haemorrhage, progressive brain injury, computer tomographic scan Introduction Trauma is the fifth leading cause of death in Malaysia in the year 2002 where traumatic brain injury (TBI) is one of the leading causes of death in young adult (1). Computed tomography scan (CT scan) imaging service is available in every state hospital currently with the improvement of the health care system in Malaysia in the 8th Malaysia Plan. Different trauma patients in different hospitals with different management protocols have their CT-brain done within first few hours of injury. In these settings, the first CT examination at admission apparently may fail to identify an intracranial lesion that evolves continuously, especially if the first CTscan is obtained within few hours after trauma (2, 3). Hence, it is advisable to have guidelines for early repeat CT scanning to detect progressive evolving haemorrhage before irreversible neurological deterioration occurs (4, 5). Unfortunately, CT-scan is being repeated routinely for almost every head-injured patient in our centre to avoid unforeseen complication without concrete indication. As a result, the workload and burden of the hospital has been increased with unnecessary radiation exposure to the patient. Moreover, most of the repeated CT-scan did not show significant changes compare to the previous one; therefore if the line of management remained the same, it might lead to a waste of resources. The timing of repeat CT brain is not clear and doing it after 24-48 hours may be too long (6). If the CT brain was repeated when Glasgow Coma Score (GCS) dropped suddenly or papillary changes occured, it might be too late for the patient and thus the prognosis would worsen. In this regard the objective of this study was to identify the predictors for CT detection of delayed traumatic intracranial haemorrhage and progressive traumatic brain injury (TBI) as well as the most ideal time for repeated CT scan brain to be done in Hospital Kuala Lumpur (HKL) with limited resources and manpower on suitable protocol might benefit busy government hospitals in the long run. Patients and Methods A cross sectional study was performed to determine the predictors of two pathologies namely Delayed Intracranial Haemorrhage (DTICH) and Progressive Traumatic Brain Injury (PTBI). The outcome variables was dichotomized as DTICH/ PTBI positive or negative. The diagnosis of DTICH was based on computed tomography (CT) as well as clinical criteria and was defined as the appearance of a new intracerebral hematoma hours to days after the inciting trauma. The diagnosis of PTBI was based on CT as well as clinical criteria and was defined as the appearance of a new intracerebral hematoma or the significant enlargement of a preexisting hematoma hours to days after the inciting trauma. The data was analysed using SPSS software version 12.0. All adult patients with all grades of TBI, admitted to Kuala Lumpur General Hospital within a period of 12 months from the first quarter of 2002 were studied and patients were categorized into 3 major groups according to Glasgow Coma Scale (GCS). Inclusion criteria were adult patient who were treated non-surgically after reviewing the first CTscan and those who had at least two CT-scan brains done regardless of the first CT-scan brain findings and exclusion criteria were children (<12 yrs) as well as patients who were treated surgically after reviewing first CT-scan. The CT-scan brain finding and GCS were classified into standard published criteria (7-14). Data collection were divided into three major groups which were CT-scan findings and changes, clinical features/history, and laboratory investigations. Statistical analysis Numerical variables were presented with mean and standard deviation. Categorical variables were presented with frequency and percentage. The outcomes were two variables which were second CT-scan with new lesions and second CT-scan with changes. Univariate analysis was performed by using Pearson Chi-Square test or Fisher’s Exact test for categorical variables based on expected frequencies of the cells. Independent t-test was applied for analyzing numerical variables. P-value was set at 0.05. Backward stepwise Multiple Ingistic Regression analysis was used to determine factors associated with the outcomes likelihood ratio test was used to determine the significance of the model. Fit of the model was checked by Hosmer-Lemeshow test and the classification table. The results were presented with crude and adjusted odds ratio, 95% Confidence Interval, Wald statistic and corresponding p-value. Statistical Package for Social Science (SPSS) version 12.0 was used for data entry and analysis. Results Eighty-one patients fulfilled inclusion criteria where male was preponderant (6.36:1) in this study. Out of 81 patients, 70(86.4%) were males. Ethnic groups comprised of 43 (53.1%) Malays, 11 (13.6%) Chinese, 19 (23.5%) Indians. Eight (9.9%) patients were categorized in ‘others’ which included those patients from Sabah, Sarawak, Indonesia and Vietnam. Age ranged from 14 to 72 years old with a mean of 33 years (SD of 15.8 years). In this study, the types of trauma were broadly classified into 3 categories namely motor vehicle accident (MVA), fall from height and assault. MVA cases comprised of 81.5% of the total, whereas 14.8% and 3.7% were fall from height and assault cases respectively. Majority of patients studied were referred cases from different level trauma centers. The states of referrals in accordance to the most level of sophisticated and trained personel to the lowest were Selangor, Pahang, Negeri Sembilan and Melaka. There were 28 (29.6%) patients admitted directly to HKL and the remaining 53 (70.4%) cases were referrals. Selangor referred majority of patients 42 (68.9%). The rest of the referrals were 6 (9.8%) patients from Pahang, Melaka 6 (9.8%) and 7 (11.5%) from Negeri Sembilan. Among all the patients in this study, 44.4% of them were classified as having mild head injury; followed by 35.8% in moderate head injury and the remaining (19.8%) sever head injury. Among those patients with second CT brain, 45.5% had improved GCS status prior to the imaging. 24.2% of them deteriorated and this was 6% higher than those with full GCS status (18.2%). The remaining 12.1% had unchanged GCS status. A total of 41.8% of the patients were detected to have only one intracranial bleed as compared to 35.8% of them who sustained multiple intracranial bleeds. Diffuse Axonal Injury (DAI) group attributed to 16.1%. It was clearly demonstrated that majority (more than 50%) of the patients had their CT brain done earlier than 250 minutes. Among all the types of intracranial haemorrhage, intracranial bleed (ICB) had highest chance (64%) to evolve; followed by extradural hematomas (EDH) (32%) then subdural hematomas (SDH) (4%) whereas subarachnoid haemorrhage (SAH) and diffuse axonal injury (DAI) would not evolve . ICB was shown to cause most frequent occurrence of PLE (79%). This figure was followed by SDH (16%). Univariate Analysis for outcome as second CT with new lesions By comparing the two different-age groups, three (23.1%) patients aged 50 and above were observed to have new clots in second CT scan lesions comparing to 7.4% in patients < 50 years old. Five (63%) of 8 patients with new lesions in CT scan were from those below 50 years old . They were not significant statistically, age of patients and delayed intracranial hemorrhages were not related (p=0.113) (Table 1a, b). By comparing the two gender groups, 90% of male patients were observed to have no new clots in second CT scan lesions. This was quite comparable to 90.9% of female patients with no new clots seen. Among all the patients with CT scan changes, 88% were from males. Gender was not associated with new bleed in second CT brain (Fisher’s Exact Test: p=0. By comparing the races, Malay and Indian patients together comprised 54 (87.1%) of 62 patients; and 19 Chinese and other races (100.0%) were observed to have no new clots in second CT scan. A hundred percent of those with new clots found were from Malay and Indian group. These differences were not significant statistically and no association between the races of patients with delayed intracranial hemorrhages (Fisher’s Exact Test: p=0.188) (Table 1a, b). By comparing the types of trauma, only 5 out of 66 (7.6%) patients who suffered from MVA were found to have new clots in second CT scan lesions as opposed to 20.0% in other types of trauma group. MVA contributed to 63% of those with new clots found in second CT brain. They were not significant statistically and no association between the types of trauma with delayed intracranial hemorrhages (p=0.162) (Table 1a, b). Types of admission (whether direct or referral) did not significantly influence the outcome of finding new lesions in second CT scan. The difference observed between 7.1% from direct and 11.3% from indirect admissions in having new clots in second CT scan were not statistically significant (Fisher’s Exact Test: 0.162). Similarly, 64% of indirect admissions were not associated with new clots. Thus, second CT brain with new clot was not associated with types of admission (Table 1a, b). A total of 38.5% of referrals which were from Melaka & Negeri Sembilan had new clot in second repeated CT scan as compared to 0.03% of referrals which were from Selangor & Pahang Hospital. Referrals from Melaka & Negeri Sembilan Hospital were observed to have higher percentage (38.5%) than the expected value of 10.5%. Some more, out of the cases with new clots found, 83% of them were those from Melaka & NS. Null Hypothesis is not true as second CT brain with new clot was shown to be associated with referral hospital with p = 0.02 (Table 1a, b). Comparison between the lower and higher ranges of GCS status was made. The lower range of the GCS level with the mean of 9.38 was associated with the finding of new clots in second CT brain as opposed to those with the mean of 11.66 which was associated with no new clots. However, GCS during admission was not associated with new clot with p = 0.039 (Table 1a, b). Even though 88% of the moderate and severe head injury group had new clots seen in second CT scan, only 16.7% versus 2.6% in moderate/severe and mild injury respectively were associated with new clots of which was marginally significant statistically with p=0.58. By analyzing these data to compare between the combined group (full/improved/unchanged GCS level) with deteriorated GCS patients, 6% and 27.8% were shown to have new clots in second repeated CT scan respectively. It means that there was 16% higher value observed in group with deteriorating GCS level than the expected frequencies of 11.8%. Majority of those with new clots were those with clinical signs of deterioration (worsening GCS level) ~63% out of 8 patients. Thus, a conclusion could be drawn that there was an association between the new clots found in the repeated CT scan with GCS level clinically as the Fisher’s Exact Test shows p= 0.026 (Table 1a, b). These two groups of patients were compared for the purpose of analyzing the specific motor component of GCS assessment. 23.8% of those with unchanged/ deteriorating GCS level had new clots found in second CT scan, instead of 6.3% of the full/improved GCS group. Almost 2/3(63%) of those with new clots found were come from the unchanged/deteriorating group. The motor component of GCS assessment was an important predictor for anticipating the findings of intracranial new clots with significant statistical p value of 0.043 (Table 1a, b). Whether there was presence of SAH or not would not affect the outcome of findings of new clots in second CT scan with the p=0.367. Null Hypothesis is true in saying that the findings of 16.7% and 7.9% in those with or without SAH respectively were only happening by chance (Fisher’s Exact Test: p = 0.367) and there is no association between SAH and second CT brain with new clot. Distribution in ranking of lab-HB on admission had significant effect to occurrence of new clots observed in second CT scan. At glance, there was obvious difference in terms of the ranges of lab-Hb in relation to CT scan new clots findings from the graph demonstrated. 66 patients with no new lesion seen are those with the mean lab-Hb of 12.38gm% and 8 patients who had new changes were those with the lower value of mean lab-Hb (9.6gm%). There was no association between the lab-Hb and new lesions in the repeated CT scan (p<0.001) (Table 1a, b). The distribution of the platelet count on admission also contributed to the changes observed in 2nd CT scan. Lower ranking of lab-platelet with the mean value of 159.5 X 109/L had significant influence in causing new clots seen in 2nd CT scan as opposed to higher value of lab-platelet (mean - 222.6 X 109/L). It was statistically significant with the p-value of 0.011(Table 1a, b). Comparison between the lower and higher ranges of lab-sodium level was made. The lower range of the lab-sodium with the mean of 136.4mmol/L was associated with the finding of new clots in second CT brain as opposed to those with the mean of 138.9mmol/L which was associated with no new clots. However, these findings were not significant statistically (p=0.161) (Table 1a, b). Comparison between the lower and higher ranges of lab-potassium was made. The ranges of distribution were fairly equal in both groups. As noted above, these findings were not significant statistically (p=0.88) (Table 1a, b). Comparison between the lower and higher ranges of lab-PT level was made. The larger distribution of the lab-PT level with the lower mean of 12.9s was associated with the finding of new clots in second CT brain as opposed to those with the mean of 13.0s, which was associated with no new clots. However, these findings were not significant statistically (p=0.845) (Table 1a, b). It was found that the shorter the time interval between trauma and first CT scan (mean: 104.6min), the higher tendency for the second CT scan to have new lesion. If the ranking of the time interval was higher (mean: 229.4min) there was a higher chance of 2nd CT scan not to have a new lesion (p=0.002) (Table 1a, b). Blood pressure at presentation seemed not to be an important clinical parameter (Table 1a, b). Univariate Analysis for outcome as second CT with changes Nine out of 13 patients (69.2%) with ages 50 and above had second CT scan changes, and this figure was higher than the expected frequency of 42.0%. Age factor for being used as one of the predictor of CT scan changes was not happening by chance, (c2=4.723, df=1, P=0.030). Further evidence was shown when 26% and 9% of those with 50 years old and above had positive and negative changes in 2nd CT scan respectively (Table 2). By comparing the two different gender group, 42.9% of male patients were observed to have new clots in second CT scan lesions as opposed to 36.4% of female patients. 88% of those with new lesions in CT scan were from males and almost similar incidence (85%) had happened in male patients without second CT brain changes. They were not significant statistically and no co-relation between the gender of patients with progressive intracranial hemorrhages (p=0.754) (Table 2). Influence of races to have changes seen in the second CT scan was studied with the results as shown above. It was found that 30 out of 62 (48.4%) of both Malay and Indian had more chances of obtaining 2nd scan changes comparing to the group comprising of Chinese and others (21.1%). It was significant statistically with the p=0.035. Malays, who were the main race of the samples collected (62 out of 81 patients), were contributing 56% to those with changes in second CT scan; Indian 32% and Chinese 12% only (Table 2). A total 40.9% of patients, who suffered from MVA, were observed to have second CT scan changes as opposed to 46.7% in patients who either fell from height or being assaulted. 79% of those with changes in second CT scan were from the MVA group; 18% fall from height and 3% assault. There were not significant statistically and no association between the types of patients with progressive intracranial hemorrhages (c2=0.166, df=1, P=0.683) (Table 2). Fifty three (65.4%) out of all the samples studied (81) were the referrals from other hospitals. Among these, 27 (59.0%) of them had 2nd scan changes. This could be compared with only 25.0% of them who were admitted directly. It was 58% higher frequency in referred cases to have second scan changes comparing to the direct admission group (21%). Types of admissions did influence the outcome of whether there was second scan changes or not as the p=0.024 (Table 2). By comparing the different states of referrals, 61.5% of patients from Melaka/Negeri Sembilan were observed to have second CT scan changes as opposed to 43.2% in patients who came from Selangor/Pahang. 70% of those with changes in second CT scan were attributed by those referrals from Selangor/ Pahang. They were not significant statistically and no associated between the different states of referrals with progressive intracranial hemorrhages (c2=1.356, df=1, P=0.244) (Table 2). Comparison between the lower and higher ranges of GCS status during admission was made. The lower range of the GCS level with the mean of 11.21 was associated with the finding of second CT brain changes as opposed to those with the mean of 11.60 which was associated with no changes. However, these findings were not significant statistically ( P=0.671) (Table 2). By comparing the different severity of intracranial injury, 47.2%, 31.0% and 50.0% of patients with mild, moderate and severe intracranial injury respectively were observed to have changes in second CT scan lesions. 50% of those with changes in second CT scan are from those with mild intracranial injury. There were not significant statistically and no association between the different levels of severity of intracranial injury with progressive intracranial hemorrhages (c2=2.255, df=2, P=0.463) (Table 2). Number of the both groups of patients studied was fairly equal (34 vs 40). For those with second CT scan changes, the ranking of the lab- Hb were at the lower site with the mean value of 11.48gm%. In contrast, no second CT scan changes were seen in those with higher ranking of lab-Hb with the mean of 12.59gm%. Thus, lower value of lab-Hb on admission was associated with higher incidence of second CT scan changes (P=0.038) (Table 2). Comparison between the lower and higher ranges of lab-platelet was made. The more dispersed the lab-platelet value with the lower mean value of 213.7 X 10/L was associated with the finding of changes in second CT brain as opposed to those with the mean of 217.7 X 10/L which was associated with no changes. However, these findings were not significant statistically (MannP P=0.515) (Table 2). Comparison between the lower and higher ranges of lab-sodium level was made. The lower range of the lab-sodium level with the mean of 138.1mmol/L was associated with the finding of changes in 2nd CT brain as opposed to those with the mean of 139.1mmol/L which was associated with no changes. However, these findings were not significant statistically (P=0.353) (Table 2). Comparison between the lower and higher ranges of lab-potassium was made. The lower range of the lan-potassium with the mean of 3.6mmol/L was associated with the finding of changes in second CT brain as opposed to those with the mean of 5.6mmol/L which was associated with no changes. However, the median of both the groups was fairly equal. The results were not significant statistically (P=0.934) (Table 2). More prolonged the bleeding profile (longer PT level), the higher tendency for the second CT scan with new clots found. 33 patients who had longer PT level (mean=13.34gm%) were found to have new clots in second CT scan. 42 patients with mean lab-Hb of 12.56gm/% were not associated with new clots in second CT scan. It was statistically significant with p=0.016 (Table 2). Comparison between the lower and higher ranges of lab APTT was made. However, the data from both of them was fairly similar in terms of the ranking and median level. Any difference observed was occurred only by chance with the p=0.690. These findings were not significant statistically (Table 2). The shorter the time interval between trauma and repeat CT scan (mean=179.8mins), the higher tendency for such patients to have new clots in second CT scan whereas with the longer time interval (mean=244.1mins), the lesser occurrence to have new clots found in second CT scan. With the p=0.053, it can be concluded that the shorter the time interval between trauma and second CT scan, the higher the tendency for patients to have new clots in second CT scan (Table 2) . In this study, 604.00 minutes ( ª 10 hours) would be the upper limit of the interval between trauma and repeat CT-scan to have higher chance of new changes in the repeat CT-scan. It was not that 10 hours ± 2 hours (standard deviation = 121.3135 minutes) would have been the proven appropriate time to repeat CT-scan. Patients with presence of indication to repeat CT brain had 2.98 times higher chance in getting a positive changes in second CT brain comparing to those without indication. Blood pressure did not seem to be a contributing parameter towards the second CT changes (Table 2). Multiple Logistic Regression analysis revealed that five parameters were selected by modeling procedure to determine whether there were association with second CT-scan with changes. They were age, race, severity, GCS status (motor component) and GCS during admission (Table 3). Those who were age more than or equal to 50 years old were almost 7.5 times more likely to have second CT scan with changes compared to those who were less than 50 years (OR=7.43, 95% CI 1.38, 40.03, p=0.020). Chinese and other races were not different from Malay and Indian in association with second CT scan with changes (OR=0.19, 95% CI 0.03, 1.12, p=0.066). For those patient with moderate severe clinical conditions were less likely to have second CT scan with changes compared to those with mild severity (OR=0.16, 95% CI 0.03,0.93, p=0.041). Patients with unchanged or deteriorated GCS status (motor component) were nearly six times more likely to have second CT scan with changes than those with improved or full GCS status (OR=5.86, 95% CI 1.45, 23.64, p=0.013). One unit higher GCS score during admission was 0.74 times less likely to be having second CT scan with changes 0.74, 95% CI 0.55, 1.00, p=0.051. This findings was marginally significant. Multiple logistic regression revealed that parameter were not associated with second CT scan with new lesion. Discussion GCS status, GCS status (motor component), haemoglobin level, platelet count, referral hospital and time interval between trauma and first CT brain were the significant predictors of delayed intracranial haemorraghe (DTICH). Conscious level upon admission was not significant in this study because the new clot was yet to form. However, deterioration of the GCS level was coinciding with the mass effects resulted by the new clot. Therefore, it was not surprise to have this factor to be the significant predictor. Motor component of the GCS was investigated solely as it could be assessed precisely even in patients with bilateral periorbital hematoma and intubated patients. Patients with sedation, which suppressed the motor response, were excluded in this study. However, parameters of coagulopathy were not quite consistent in finding the platelet count with the mean of 159.5 x 109/L of causing DTICH but not the PT/APTT value. Somehow these parameters had been quite controversial so far to be the significant predictors in all the previous studies (15, 16). Low hemoglobin level with the mean of 9.6gm% was proved to be more easily associated with new clot because in such a situation, there would be an instantaneous loss of blood volume with or without the occurrence of disseminated consumptive coagulopathy (associated with low platelet count). Throughout the process of correction of the anemia/ hypovolemia episode, the sudden surge of the blood pressure will favor for bleeding tendency and lead to the formation of new clot (16). During the period of this study 2380 patients with TBI were seen of whom 245 were severe TBI and 1812 were moderate TBI. 323 patients with mild TBI were also referred to HKL in this period. All patients with mild, moderate and severe TBI referred received CT scan of the brain. The mild TBI had CT scan due to presence of skull fractures on their skull x-ray. 2054 patients who were treated surgically and those not receiving at least two CT scan were not included in this study. This meant that a majority of the patients received less than two CT scans. Due to the fact that HKL accepted only referral cases nearly 40% the mild TBI included in the study received CT scan more than twice and were admitted for observation even though the volume of the clots were small. As for the CT scans, all 1st CT scans were abnormal for all categories of TBI. Not surprising that time interval between trauma and first CT brain was one the most important predicting factors as the sooner after injury the first scan is performed, the greater likelihood there is subsequent hemorrhagic progression on later CT scans (17, 18). Referral hospitals will contribute to the difference in terms of the time interval between trauma and first CT brain. Patients admitted to state hospitals of Melaka/NS took lesser time for them to obtain CT brain facilities. Pupillary changes was not an important predictor as it could be explained by the fact that it was a late clinical sign/ manifestation whereby changes in other clinical evaluating modalities such as GCS assessment are more sinister in predicting the new clot formation in second CT scan. Age, race, types of admission, GCS condition, pupillary changes, no of lesions, haemoglobin level, prothrombin time and the time interval between trauma and first CT brain are found to be significant predictors of progressive brain injury (PBI). In older patients who were at higher risks of having hypertension, diabetes mellitus and amyloidosis were predisposed to vascular rigidity and fragility, leading to haemorrhagic stroke subsequently (19, 20). In cases with cerebral atrophy, there were more potential spaces for the clot to evolve. The severity of head injury was not influencing the outcome of PBI. However, the deterioration of the GCS is significantly affecting the possibility of PBI (p = 0.02). It is surprising that the motor component was not sensitive to detect PBI as what was being proposed in the previous discussion. Pupillary change was a sensitive clinical assessment on the mass effect caused by the brain edema and the evolving clot. Both the age and number of intracranial bleed (solitary or multiple) were inter-related. It was shown that patients with age of more than 50 years old were more prone for multiple intracranial bleed (21). Similarly haemoglobin level and the time interval between trauma and first CT brain had the same significance as explained before. However, prothrombin time was found to be an important predictor rather than platelet count. In massive trauma, the major mechanism is believed to be autoinfusion of tissue thromboplastins which is the triggering factor in activating extrinsic coagulation pathway (prolonged prothrombin time) (22). Thus, it was not surprising that it was an important predictor for PBI. In our setting, ICP monitor facilities were limited. Often, patients who suffered from traumatic head injury with MLS were intervened early (decompressive craniectomy/ lesionectomy) as putting patients under cerebral protection without ICP monitoring is not justified! Therefore, the insignificance of MLS as a predictor is selfexplained. SAH plays an important role in progressive intraparenchymal damage (23). However, it was not a significant predictor in this study. Variation of the resolution power of the CT scan machine from various states might contribute to the difficulties in picking up SAH lesions occasionally. Conclusion This study showed that 9.9% of the total patients had DTICH and 42% had PTBI of all TBI patients studied during the period mentioned. A poor GCS prognosticate a poor outcome and the action to wait for the GCS to deteriorate was not justified. Consequently, other predictors should replace GCS and pupillary changes in whenever occasion if possible for early detection of DTICH and PTBI such as Hb level, coagulation profile, elder age group patient and of course the time interval between the trauma and first CT brain should be used as a guideline for patients in hospitals where no fixed protocol is present CT scans, or those who do not receive ICP monitoring. Acknowledgements Dr. Toh Charng Jeng’s publication is part of the partial fullfillment for the Master of Surgery (Neurosurgery) USM Programme. References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08040t2.jpg] [mj08040t3.jpg] [mj08040t1b.jpg] [mj08040t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}