 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
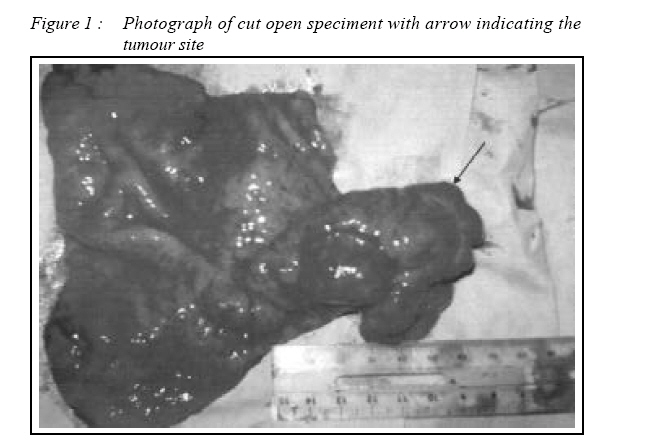
CASE REPORT Stomach gastrointestinal stromal tumours (GIST) intussuscepted into duodenum : A case report Febra Anak Siam & Sze Li Siow Department of General Surgery, Serawak General Hospital, Jalan Tun Amad Zaidi Adruce, 93580 Kuching, Serawak, Malaysia Submitted-20-02-2005, Accepted-30-6-08 Code Number: mj08041 Gastrointestinal stromal tumours are tumours of gastrointestinal tract and mesentery. The commonest site of it occurrence is stomach. Patients with GISTs are usually asymptomatic but they can present as abdominal pain, bleeding and rarely gastric outlet obstruction. In this particular case, patient presents with symptoms of anaemia, partial gastric outlet obstruction and intermittent epigastric pain. Laparotomy was performed and a diagnosis of gastroduodenal intussusception secondary to gastrointestinal stromal tumour was made. Key words : Gastrointestinal stromal tumours (GIST) Introduction Gastrointestinal stromal tumour (GIST) are distinct subgroup of tumours that derived from the gastrointestinal mesenchyma which could neither be classified as neurogenic – non smooth musclederived tumours. These tumours include leiomyomas, leiomyoblastomas and leiomyosarcomas. GIST was first applied to these group of tumours in 1983 by Mazur and Clark (1). These tumours can occur at any sites along the gastrointestinal tract and stomach is the commonest site followed by small bowel. The median age of its occurrence is 50-60 years old with a slight male predominance (2). The incidence rate of these tumours is around 16 per million populations and in UK the rate of new cases is about 900 cases per year (5). Case Report This patient is a of 29 years old Iban gentleman who presented with intermittent upper abdominal pain associated with nausea and vomiting. He also claimed to have symptom of anaemia such as lethargy, generalized body weakness, giddiness and exertional dyspnoea for 5 months. He had poor appetite in which he is able to tolerate fluid and small amount of solid diet and he is losing weight. In the past, he had history of passing malaenic stool without haematochezia. Multiple oesophagogastroduodenoscopy (OGDS) were done in past and he was told to have stomach ulcer associated with Helicobacter pylori infection. He was admitted to the Male Surgical Ward for workup for his illness. On examination, he is a small built young man and is clinically pale. Abdominal examination did not reveal any mass or organomegaly. There was no lymphadenopathy. Digital rectal examination revealed malaenic stool. An urgent OGDS was performed and revealed a huge tumour in the stomach obstructing the pylorus and the duodenum was not able to be entered. Biopsy was taken reported as benign gastric ulcer. Laparotomy was performed and intraoperatively there was a huge polypoidal mass arising from the antrum measuring 6 x 6 cm. The mass had a wide pedicle and was bosselated with area of necrosis. The whole mass had intussuscepted into the duodenum down till D2/ D3 junction. There were few lymph nodes identified along the right gastro-epiploic vessel. The duodenum was stretched and dilated. Intraoperative diagnosis of GIST was made with Bilroth’s I Partial Gastrectomy was performed. Histopathology report confirmed the diagnosis. Surgical margins were clear. Patient recovered well from the operation. Figure 1Discussion The presentation for GIST is usually non specific symptom and it all depends on the size and location of the tumours. Small GISTs which is 2 cm or less usually often detected as an incidental findings during investigation for other unrelated disease because the are usually asymptomatic. The presentation of stomach GIST causing duodenal obstruction is not common. There were not many cases of GIST reported presenting with gastroduodenal intussusception. Crowler et al had reported a case of gastroduodenal intussusception in 59 years old lady who presented with a year history of indigestion and a 3 weeks history of intermittent severe epigastric pain, early satiety, bilious vomiting with undigested food. His patient had an OGDS done and noted gastric outlet obstruction. A Computered Tomography Scan (CTScan) was done with the diagnosis of intussusception which was confirmed later by laparotomy (3). in this patient we had a young gentleman who presented with symptoms of anaemia and intermittent epigastric pain. The chronic anaemia is likely due to an on going chronic blood loss from the non healing gastric ulcer. He also had history of intermittent abdominal pain as a result of intussusception. In view of the longstanding disease process which was not treated, there was significant duodenal dilatation as a result of chronic intussusception. It was not a complete obstruction as he was still able to tolerate fluid preoperatively. There was no single investigation diagnostic of GIST diagnosis. CTScan is not sensitive in diagnosing GIST but reliable in determining the size and presence of any secondaries. Barium contrast studies and OGDS help to localize the tumour but OGDS is more superior because it offered therapeutic therapy as well as detecting smaller GIST (5). Commonly the diagnosis of GIST was made based on the findings of a well defined extraluminal mass, frequently polylobulated with a pseudocapsule as seen in this patient. The confirmatory diagnosis of GIST can only be achieved via histological and immunohistochemical methods. Histologically, GIST composed of either spindle-shape cell (70%) or epitheloid cell (20%) or mixed sphindle and epitheloid (10%).In contrast to smooth muscle myoma or sarcoma, GISTs are typically immunoreactive for KIT (CD117). This is very important as 95% of GISTs are positive for KIT. The positivity for CD 34, the haemotopoietic progenitor cell antigen is reported in 70-80% of GIST (2). Surgical therapy remains the mainstay of treatment for GIST. Complete en bloc resection (R0 resection) is being the intention during the surgical procedure. Five years survival rate after a complete resection of GIST was reported as 48 - 70% depend on the risk of aggressiveness of the tumour. Many classification were made to reassess the risk of aggressiveness of GIST include by Bucher et al and Fletcher et al (6, 7). Boni et al had reported in his series that despite new chemotherapeutic regime, to date only radical surgery offer the chance of longterm survival (8). In our case, the tumour was completely resected with clear margin and intra operatively the presence of nodes noted. The presence of tumour more then 5 cm and nodes were the features of high risk tumour as highlighted in our patient. This is according to assessment by Fletcher classification to assess the risk of aggressiveness in GIST(6). Based on this viewpoint, this patient had received an adequate treatment. He was not referred for adjuvant chemoradiotherapy as his tumour was not sensitive to these modalities. The study on the usage of new drug called imatinib mesylate is however still early and no clear guideline on the usage of this drug (4). This patient is currently under closed surgical follow-up. References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08041f1.jpg] |
| |||||||||

{kind=link}