 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences , Vol. 16, No. 2, April-Jun, 2009 pp. 4-9 ORIGINAL ARTICLE Antimicrobial susceptibility of clinical isolates of Pseudomonas aeruginosa from a Malaysian Hospital Siva Gowri Pathmanathan1, Nor Azura Samat2, Ramelah Mohamed3 1Faculty of Medicine and Health Sciences, Universiti Sains Islam Malaysia, 55100 Kuala Lumpur, Malaysia; Submitted: 7 Nov 2008
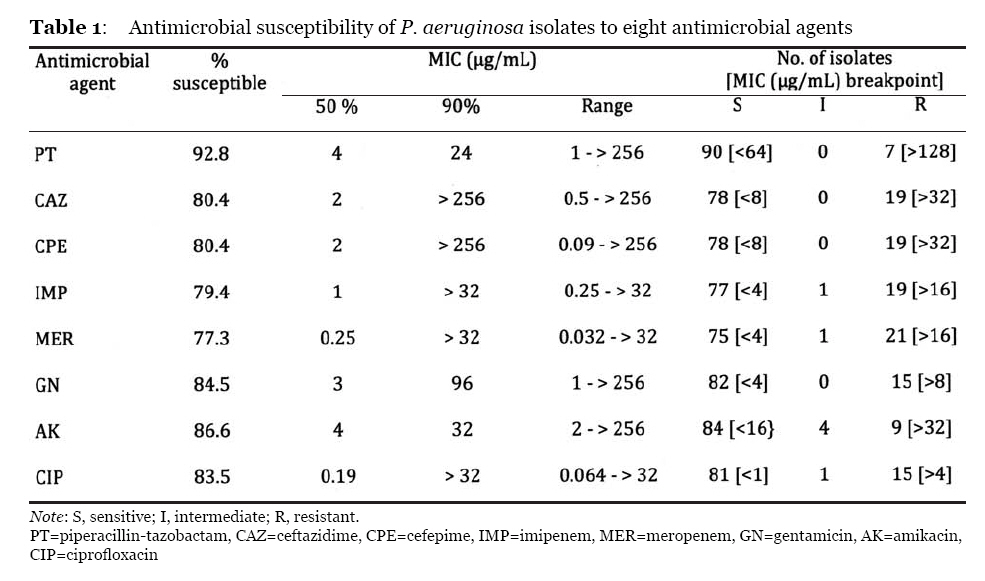
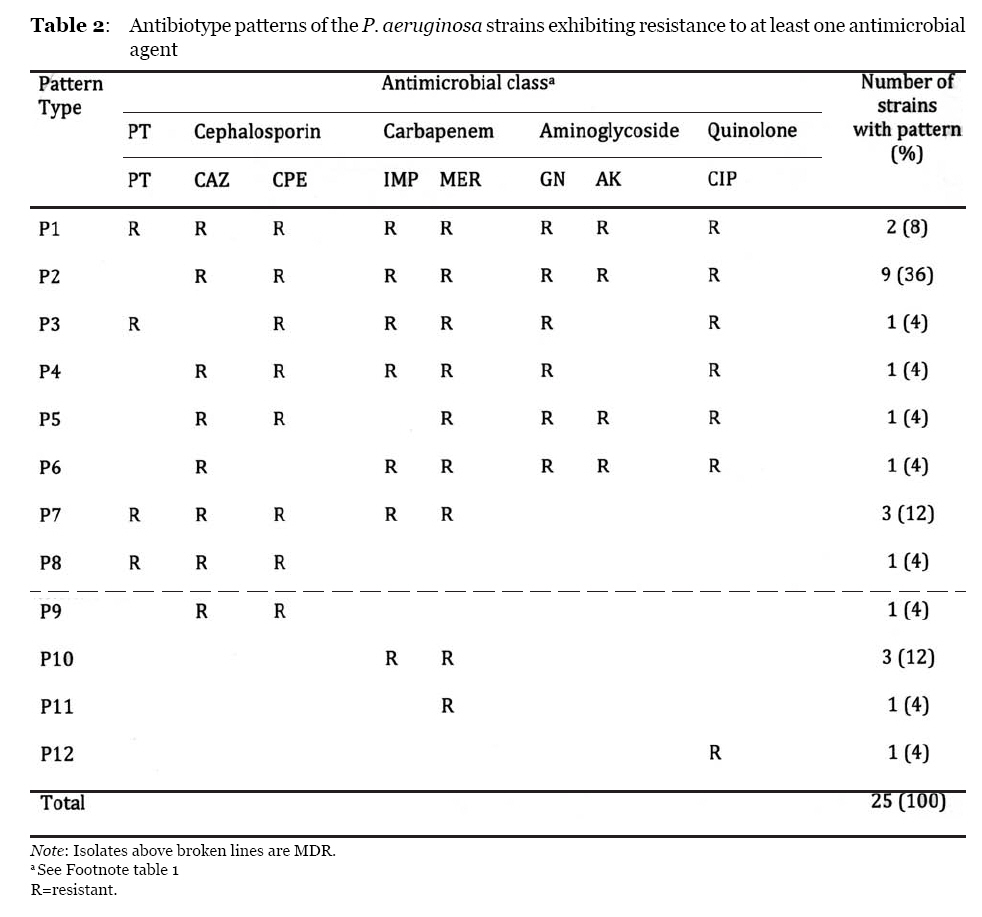
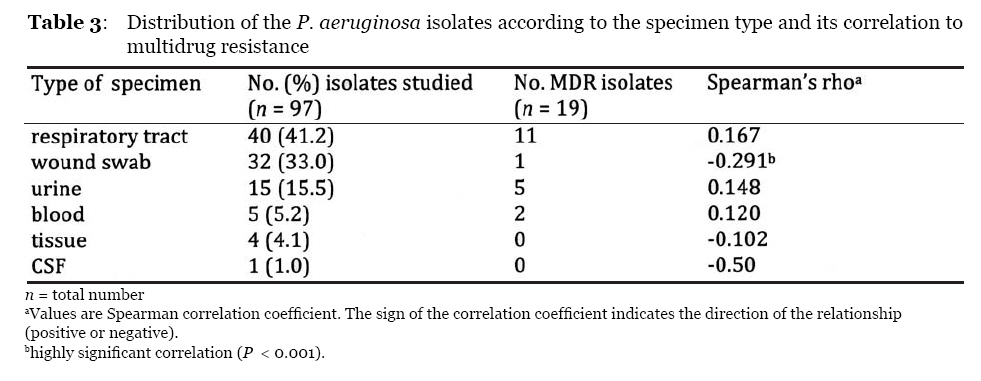
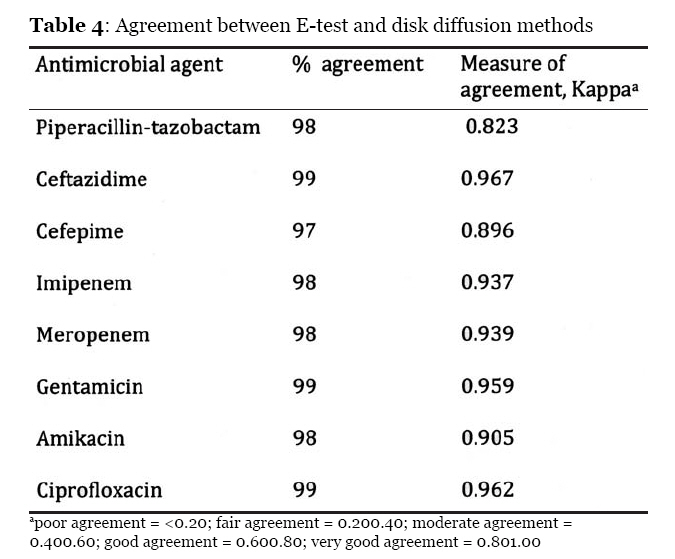
Code Number: mj09014 Abstract Ongoing surveillance of Pseudomonas aeruginosa resistance against antimicrobial agents is fundamental to monitor trends in susceptibility patterns and to appropriately guide clinicians in choosing empirical or directed therapy. The in vitro activity level of eight antimicrobial drugs was assessed against 97 clinical isolates of P. aeruginosa collected consecutively for three months in 2007 from a Malaysian hospital. Antimicrobial susceptibility was determined using the E-test method in addition to the hospital’s routine diagnostic testing by the disk diffusion method. Respiratory and wound swab isolates were the most frequently encountered isolates. The E-test and disk diffusion methods showed high concordance in determining the in vitro activity of the antimicrobial agents against the P. aeruginosa isolates. Piperacillin-tazobactam was the most active antimicrobial agent with 91.8% susceptibility, followed by the aminoglycosides (amikacin, 86.6% and gentamicin, 84.5%), the quinolone (ciprofloxacin, 83.5%) and the beta-lactams (cefepime, 80.4%, ceftazidime, 80.4%, imipenem, 79.4% and meropenem, 77.3%). Incidence of multidrug resistance was 19.6% (19 out of 97 isolates). Periodic antibiotic resistance surveillance is fundamental to monitor changes in susceptibility patterns in a hospital setting. Keywords: antibacterial agents, bacterial drug resistance, Pseudomonas aeruginosa Introduction Pseudomonas aeruginosa is an aerobic, motile, nutritionally versatile, gram-negative rod exhibiting intrinsic resistance to several antimicrobial agents (1,2). The rapid increase of drug resistance in clinical isolates of this opportunistic human pathogen is of worldwide concern (3,4,5,6,7). Ongoing surveillance of P. aeruginosa resistance against antimicrobial agents is fundamental to monitor trends in susceptibility patterns and to appropriately guide the clinician in choosing empirical or directed therapy, especially when new antimicrobial agents may not be readily available in the near future (8,9). However, there are few recent surveillance studies reporting antimicrobial resistance patterns of P. aeruginosa in Malaysia (10,11). Thus, in this study, we assessed the current in vitro activity level of eight antimicrobial drugs against clinical isolates of P. aeruginosa obtained from the Kuala Lumpur Hospital. The concordance between the E-test and disk diffusion methods in antimicrobial susceptibility testing was also evaluated. Materials and Methods Clinical isolates A total of 97 consecutive clinical isolates of P. aeruginosa were collected between October 2007 and December 2007 at the Kuala Lumpur Hospital, Malaysia a government tertiary referral hospital with 81 wards and 2,502 beds. Of the 97 specimens, 21 were obtained from general paediatric wards, 20 from general medicine wards, 14 from neurology wards, 11 from intensive care units, 9 from orthopaedic wards, 7 from general surgery wards, 5 from respiratory medicine, 4 from urology wards, 2 from uronephrology and 1 each from dermatology, ENT (ear, nose and throat), burn and nephrology wards. The isolates were identified by standard laboratory methods (1). Antibiotic susceptibility test Minimal inhibitory concentrations (MICs) of piperacillin-tazobactam, ceftazidime, cefepime, imipenem, meropenem, gentamicin, amikacin and ciprofloxacin were determined by E-test (AB Biodisk, Solna, Sweden) in addition to the hospital’s routine antimicrobial susceptibility testing by the disk diffusion method. Results of E-test and disk diffusion methods were interpreted in accordance to the Clinical and Laboratory Standards Institute (CLSI) (12). Control strains included P. aeruginosa ATCC 27853 and Escherichia coli ATCC 25922. Multidrug-resistant (MDR) isolates were defined as isolates demonstrating resistance to antimicrobials from at least two of the five antipseudomonal classes of antimicrobial drugs tested in this study: piperacillin-tazobactam, cephalosporins, carbapenems, aminoglycosides and fluoroquinolones. Statistical Analysis Statistical analysis was done using SPSS software, version 15. Statistical analysis by Spearman’s rank correlation was carried out to assess the correlation in susceptibility between two drugs. Cross-tab analysis was performed to obtain a Kappa value to measure the concordance between E-test and disk diffusion methods. The percent concordance of the two methods was calculated as follows: [(a + d)/(a + b + c + d)]*100, where a is the number of isolates sensitive by both tests, b is the number of isolates sensitive by E-test and resistant by disk diffusion, c is the number of isolates resistant by E-test and sensitive by disk diffusion, and d is the number of isolates resistant by both tests (13). The Spearman’s rank correlation was also performed to evaluate the association between occurrence of drug resistance and i) ward of patient origin and ii) specimen of isolates. In all cases, a P value of < 0.05 was considered indicative of significance. Results The results of the antimicrobial susceptibility testing are shown in Table 1. Piperacillin-tazobactam was the most active antimicrobial agent in vitro with 91.8% susceptibility, followed by the aminoglycosides (amikacin and gentamicin), quinolone (ciprofloxacin), the cephalosporins (ceftazidime and cefepime) and the carbapenems (meropenem and imipenem). Twenty-five isolates were resistant to at least one of the five antipseudomonal classes of antimicrobial agents and revealed a total of 12 antimicrobial resistance patterns (Table 2). The most prevalent pattern, P2, displaying resistance to all antimicrobial drugs except piperacillin-tazobactam was observed in 9 (36%) of the 25 isolates. The MIC of piperacillin-tazobactam on these isolates was between 3 and 16 ìg/mL. Pattern P7 was the second most common with resistance to piperacillin-tazobactam, the cephalosporins and the carbapenems. Pattern P9 exhibited resistance to the carbapenems in 3 isolates. Two isolates were resistant to all antimicrobial agents tested. Resistance to both carbapenems was observed in 20 of the 25 isolates. The overall incidence of multidrug resistance was 19.6% (19 out of 97 isolates). Table 3 shows the distribution of the 97 P. aeruginosa isolates according to the specimen type and its correlation to multidrug resistance. The E-test and disk diffusion methods showed high percentage of concordance (>96%) and an excellent Kappa measure of agreement (0.8 to 1) (Table 4). Discussion Periodic antimicrobial resistance monitoring in P. aeruginosa is fundamental to updating the current activity level of commonly used antipseudomonal drugs. In the present study, the carbapenems were the least active agents evaluated with only 77.3% and 79.4% of isolates being susceptible to meropenem and imipenem, respectively. Imipenem has been reported to be very active against P. aeruginosa in a number of recent studies, (3,10,14) while others have reported otherwise (6,15). A study done in another tertiary care hospital in Malaysia (10) involving isolates collected in 2005 reported a low incidence of imipenem resistance (9.90%) compared to the present (20.6%). Another Malaysia/Singapore study in 1999 that did not include our hospital found imipenem to be the most active â-lactam (14.7% resistance), but cefepime and piperacillin-tazobactam had higher resistance rates than the present study (11). Varying drug resistance levels in different hospitals in the same country have been reported in the past and is attributed to the differential usage of antibiotics in the respective hospitals. An Indian study (4) noted that the low incidence of imipenem resistance (7.2%) at their hospital compared to a higher resistance rate detected in another setting in the same country (16) was due to the fact that imipenem is still used as a reserve drug in the former. In general, when compared to previous Malaysian studies (10,11), our study showed higher resistance rates to all drugs tested except cefepime, meropenem and piperacillin-tazobactam. However, the difference in MDR rates between the present and other studies could not be compared due to varying definitions of multidrug resistance. A number of studies found piperacillin-tazobactam to be either the most active antimicrobial agent against P. aeruginosa or the second most active after amikacin (3, 4,7,10,17). However, a recent report has questioned the appropriateness of the current CLSI resistance breakpoint of piperacillin-tazobactam since the study discovered an increased mortality rate associated with empiric piperacillin-tazobactam therapy given to patients with P. aeruginosa bacteraemia; the isolates had reduced piperacillin-tazobactam susceptibility (18). Although amikacin was the second most potent drug in vitro, the resistance rate was higher compared to other studies (5,6,7,10). In the other studies, the resistance rate of amikacin was far lower than its aminoglycoside counterpart, gentamicin. In the present study, however, there was a significant correlation between the two aminoglycosides (rho > 0.9, P < 0.01), although the MIC90 value of amikacin (32) was lower than that of gentamicin (96). A significant correlation between class members was also observed among the cephalosporins and carbapenems (rho > 0.9, P < 0.01) with equal MIC90 values (i.e., > 250 and > 32, respectively). The high percentage of concordance and an excellent Kappa measure of agreement showed that both methods have high agreement in determining the in vitro activity of the antimicrobial agents on P. aeruginosa isolates, which corroborates similar studies (19,20) that reported an excellent and acceptable correlation, respectively, between the disk diffusion and E-test methods. Therefore, although the E-test is rapid, easy to perform and has an added ability to determine MIC value, the disk diffusion method is equally reliable and more cost-effective for routine hospital use. There was no significant correlation between drug resistance and the wards from which isolates originated (data not shown). The distribution rank of the isolates according to the types of specimens (respiratory > wound swab > urine > blood) was similar to that described by a worldwide SENTRY antimicrobial surveillance study (8), even though the total number of isolates included in the present study is incomparably small. Respiratory isolates (41.2%), including tracheal and nasopharyngeal aspirates as well as sputum, were the most frequently encountered. P. aeruginosa isolates from respiratory tract also showed the highest rate of multidrug resistance, as observed in a similar study of inpatient isolates done in a Saudi Arabian hospital (21). Wound swab isolates (33.0%) were the second most frequently encountered. However, the incidence of resistance was statistically less likely to be observed in these isolates (P < 0.001). Of the 32 pus isolates, 31 were fully susceptible to all the antimicrobial agents tested, suggesting that wound swab isolates are less likely to be multidrug resistant. Nevertheless, the correlation between specimen type and multidrug resistance would have been more noteworthy if supported by data on patients’ clinical conditions, which is a limitation of our study. In conclusion, the higher resistance rate, when compared to previous studies, calls for prudent use of antibiotics in order to limit further increases in resistance. Antimicrobial surveillance should be done periodically to monitor the current susceptibility patterns in local hospitals. A standard definition of P. aeruginosa multidrug resistance will allow better comparisons between studies. Acknowledgements We are grateful to the head of the Microbiology Unit of Hospital Kuala Lumpur, Dr Muhammad Nazri Aziz for his support and providing the isolates for this study. We thank medical laboratory technologist Ms. Mazlina Abd Ghani for her technical assistance. We also thank Ms. Emmy Hainida Khairul Ikram for assistance with the SPSS software. This study was supported by a research grant from Universiti Sains Islam Malaysia, no. PPPP(X)2006. Author contributions
References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj09014t1.jpg] [mj09014t3.jpg] [mj09014t2.jpg] [mj09014t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}