 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
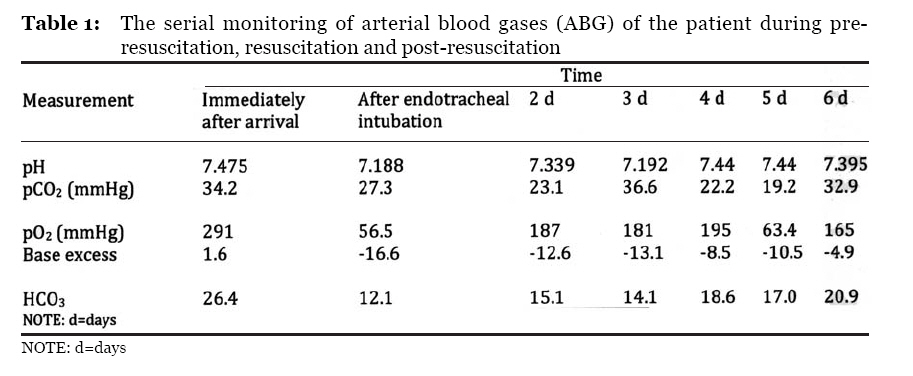
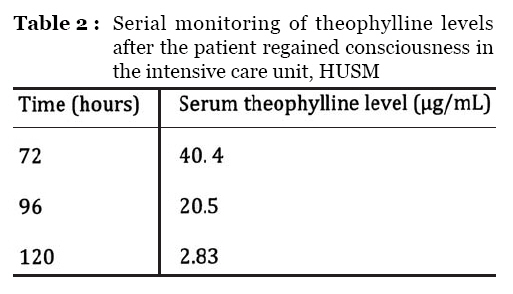
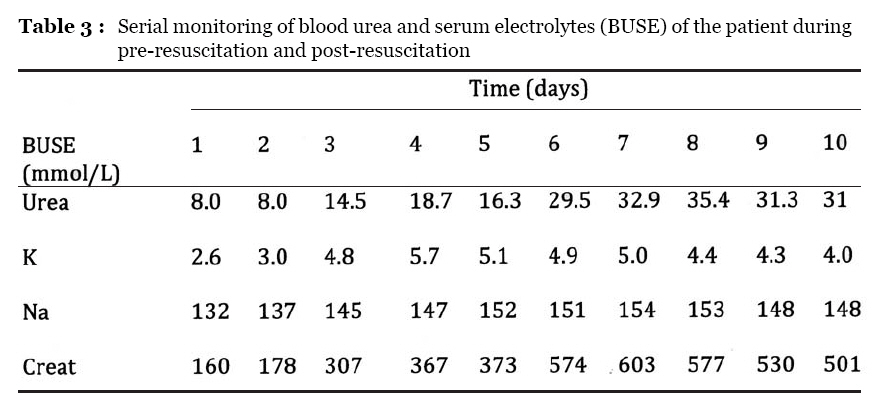
Malaysian Journal of Medical Sciences , Vol. 16, No. 2, April-Jun, 2009 pp. 4-9 CASE REPORT Theophylline toxicity: A case report of the survival of an undiagnosed patient who presented to the emergency department Nasir Mohamad, Nurkhairul Nizam Abd Halim, Rashidi Ahmad, Kamarul Aryffin Baharuddin Department of Emergency Medicine, School of Medical Sciences, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia Submitted: 10 Aug 2008 Code Number: mj09015 Abstract Theophylline toxicity is a life-threatening toxidrome that can present to an emergency department. To ascertain an immediate provisional diagnosis in toxicology at the emergency department is very challenging, especially when the patient presents with altered mental status, because the clinical features of several toxidromes overlap. We report a case of survival of undiagnosed theophylline toxicity that required intubation for two days in the intensive care unit. This was the first case to have been reported from our department. Accurate diagnosis of a toxidrome by gaining adequate history and conducting a thorough physical examination and early serum toxicology screening, coupled with good knowledge of toxicology, will lead to better patient outcomes. Keywords: Theophylline, toxicity, emergency medicine Introduction Theophylline is a commonly used drug in the treatment of acute or chronic lung diseases. Despite the considerable potential benefit of theophylline, its narrow therapeutic index and erratic absorption and elimination contribute to the potential for toxicity, which can have high morbidity and mortality (1,2). The toxidrome manifestation can present as an overlap with other drug toxicities, especially in unmonitored patients who have altered higher mental functions. We present a case of undiagnosed theophylline toxicity due to attempted suicide with sustained generalised tonic-clonic seizures with altered mental status and supraventricular tachycardia. As this was our first experience encountering such a case, we recommend a few measures that can be taken when managing a patient with an undiagnosed drug toxicity or toxidrome in the emergency department. Case report A 22-year-old man was brought to the Emergency Department (ED) of Universiti Sains Malaysia Hospital (HUSM) by family members 10 hours after the suspected ingestion 30 tablets of chlorpheniramine. He developed intermittent nausea and non-projectile vomiting (containing food particles) with abdominal pain 2 hours post-ingestion, and the symptoms persisted until he presented to the ED. On arrival, he appeared drowsy, but was not in respiratory distress. His pulse was persistently tachycardic to more than 120 beats/minute with a regular rhythm, and he was hypotensive, with a blood pressure of 90/64 mmHg. His axillary temperature was 37.0 ÚC with moist skin. His pupils were 3 mm bilaterally, equal, and reactive to light. Physical examinations of other systems were unremarkable. His electrocardiogram showed sinus tachycardia, and his capillary blood sugar was 6.7 mmol/L. In the ED, he complained of epigastric pain and urinary retention. Intravenous metoclopramide (10 mg) was prescribed to relieve vomiting along with intravenous ranitidine (50 mg), followed by activated charcoal. The patient was still hypotensive despite adequate fluid resuscitation. To restore normal blood pressure, the patient was started on an infusion of noradrenaline, which targets the peripheral alpha-1 receptor. After 2 hours in the ED, the patient underwent two generalised tonic-clonic seizures. Each episode lasted approximately 10 minutes and was aborted with intravenous diazepam. He was given intravenous phenytoin and was later electively intubated for airway protection and cerebral resuscitation. Initial blood gases showed metabolic alkalosis, and he was hypokalemic (see Table 1). The patient was admitted to the Intensive Care Unit (ICU) for monitoring and supportive care. While in the ICU, he developed a supraventricular tachycardia (SVT) and synchronised cardioversion (50 J) was delivered, which successfully reverted him back to sinus rhythm. The patient self-extubated on day two of his hospitalisation. His blood pressure was normotensive on inotropic support, but the pulse rate remained tachycardic. Further history elicited from the patient after he regained consciousness revealed that he took 30 tablets of Neulin SR 250 mg. His theophylline level was assessed immediately, and was found to be 40.4 µg/mL at 72 hours post-ingestion (see Table 2). Repeated blood gases persistently showed mild metabolic acidosis, and he also had increased blood urea and creatinine. His creatinine phospokinase (CPK) level was >10,000 IU/L, but urine myoglobin was negative. Intravenous fluid was increased to 150 mL/kg/d, and an intravenous furosemide infusion was started. He was referred to a nephrologist due to the development of acute renal failure, and due to the toxic level of theophylline he was referred for hemoperfusion therapy to enhance theophylline elimination (see Table 3). However, he was treated conservatively. His theophylline level eventually decreased to 20.54 µg/mL and 2.834 µg/ml at hospital day 5 and day 6, respectively. His CPK level decreased to 7471 IU/L, and three repeated urine tests for myoglobin were negative. His blood pressure and heart rate later normalised, and he was transferred out to the High Dependency Unit (HDU) at hospital day 7. The patient was discharged well from the hospital after 2 weeks of hospitalisation without neurological deficit and with normalised renal function. Discussion We here describe a young patient who had allegedly intentionally ingested 30 tablets of ‘chlorpheniramine,’ but who at day 3 of hospitalisation admitted to having taken theophylline SR tablets, and was in acute theophylline toxicity. To ascertain an immediate provisional toxicological diagnosis in the emergency department is very challenging, especially when the patient presents with altered mental status. The clinical features of one toxidrome often overlap with other toxidromes. In this case, the patient initially presented at 10 hours post-ingestion with a history of abdominal pain, urinary retention, nausea, and vomiting, and with normal body temperature, equal pupil sizes, and altered mental status. At the emergency department, he developed hypotension and sinus tachycardia, and he subsequently developed generalised tonic-clonic seizures and supraventricular tachycardia (SVT). The presenting complaints were not a common presentation of anticholinergic toxicity (the incongruous findings were hypotension, moist skin with a normal body temperature, the pupil sizes and hypokalaemia). Such findings were more closely associated with toxicity related to theophylline, tricyclic antidepressants or phenothiazines. In general, the common presentations of chlorpheniramine (anticholinergic) toxicity are dementia with mumbling speech, tachycardia, dry flushed skin, dilated pupils, myoclonus, slightly elevated temperature, urinary retention, decreased bowel sounds, seizures, and cardiac arrhythmias (3). The best initial emergency department management of the patient depends on an accurate toxicological diagnosis. Had theophylline toxicity been suspected initially, intermittent gastric lavage with activated charcoal (46 grams every 46 hours) could be instituted aggressively. This would double the rate of elimination of theophylline. Alkaline diuresis could also be considered in this case, but is not generally recommended (4). The most common metabolic responses to theophylline toxicity in the literature are hypokalaemia, hyperglycaemia, lactic acidosis, hypomagnesaemia and hypophosphataemia (4,5,6). Thus, the presence of such abnormalities should raise suspicion of overt theophylline toxidromes. In this situation, toxic screening would be beneficial. If screening is done early in the emergency department, it can guide the specific management of the drug toxicity. Gastric emptying before administration of activated charcoal appears not to improve outcomes. There are several studies that failed to document any benefits from gastric emptying prior to the administration of activated charcoal . (7) Gastric lavage should not be considered unless a patient has ingested a potentially life-threatening amount of a poison. The procedure can be performed within 60 minutes of ingestion (8). Even then, a clinical benefit has not been confirmed in any controlled studies, according to the American Academy of Clinical Toxicology/European Association of Poisons Centres and Clinical Toxicologists Position Statement (9). Therefore, the best method available in the ED to reduce drug absorption from the gastrointestinal tract is the administration of activated charcoal, which is both rapid and very efficient. Orally-given activated charcoal may be the most effective treatment for a sustained-release theophylline overdose. The maximum benefit is obtained when it is administered soon after an overdose, although later administration might still be of value (10). It has been suggested that the mechanism of action of charcoal in theopylline toxicity is the adsorption of theophylline in the lumen of the gut through direct dialysis of theophylline across the gut mucosal capillaries. This interrupts enterohepatic circulation of the drug and promotes back-diffusion of theophylline from the blood to the intestine (11). Multiple doses of activated charcoal (MDAC) are recommended in patients who have ingested a life-threatening amount of theophylline (12). MDAC have been shown to significantly enhance the elimination of both parenterally administered and orally administered theophylline (12,13,14,15). The dosing should be 3040 g every 4 hours, but equal benefit has been demonstrated by giving smaller doses more frequently (16). In a case of potentially severe or life-threatening toxicity, extracorporeal elimination is recommended. The choices are charcoal hemoperfusion, continuous haemofiltration, or haemodialysis (17,18). In cases of slow-release theophylline overdose with rising theophylline levels and patient deterioration despite adequate gastrointestinal decontamination, gastric pharmacobezoar formation (the residue of sustained-release formulations) should be suspected. This can result in fatality (19). There have also been reported cases of successful treatment of theophylline toxicity by upper gastrointestinal endoscopic removal of all the tablets in the stomach 4 hours after ingestion (20). Intractable vomiting caused by theophylline toxicity can be controlled with a variety of antiemetics such as metoclopromide, prochloperazine and droperidol. Some authors recommend the use of ranitidine in conjunction with an antiemetic, as the reducing xanthine will induce a decrease in gastric acidity and a reduction in gastric acid volume. Ranitidine is preferable to cimetidine because ranitidine interferes less with hepatic clearance (21). However, there are reported cases that ranitidine can induce chronic theophylline toxicity in the elderly (22). Animal studies in rats concluded that cimetidine and ranitidine can induce interstitial nephritis, and thus these drugs should be used with caution. In the described patient, the renal profile on arrival was already deranged, and thus ranitidine was used with caution. Ranitidine has the potential to worsen renal function and delay its own clearance. Thus, its interference with hepatic metabolism can be prolonged (23). This is important to keep in mind when managing patients with theophylline toxicity. Seizure is a sign of neurotoxicity and is considered a poor prognostic sign. The serum concentration at which seizures are triggered is unknown. Intravenous diazepam may be used alone to control the seizures but it is not very effective in most cases. Phenytoin, phenobarbitone or carbamazepine can be used in combination, because these drugs increase theophylline metabolism, thus reducing the theophylline serum concentration (24). Short-acting antiepileptic use is advocated because they enhance the rate of elimination of theophylline through activation of CYP3A4 (25). They also decrease absorption of theophylline through activation of gut CYP3A4 proteins, which enhances first-pass metabolism for theophylline. Aside from their use as anticonvulsants, antiepileptics can also be useful in drug-induced supraventricular tachycardia. In this case, extracorporeal elimination of toxin would have been beneficial, but the theophylline toxicity was diagnosed too late. Due to the delay in diagnosis, the patient developed seizures and hypotensive episodes that required inotropic support, a sign of life-threatening intoxication. In conclusion, an accurate diagnosis of a toxidrome by gaining adequate history and conducting a thorough physical examination and early serum toxicology screening, coupled with good knowledge of toxicology, will lead to better patient outcomes. Acknowledgements The authors thank Dr Chew Ken Sheng for technical and editorial assistance. Author contributions Conception and design: NM References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj09015t2.jpg] [mj09015t3.jpg] [mj09015t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}