 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
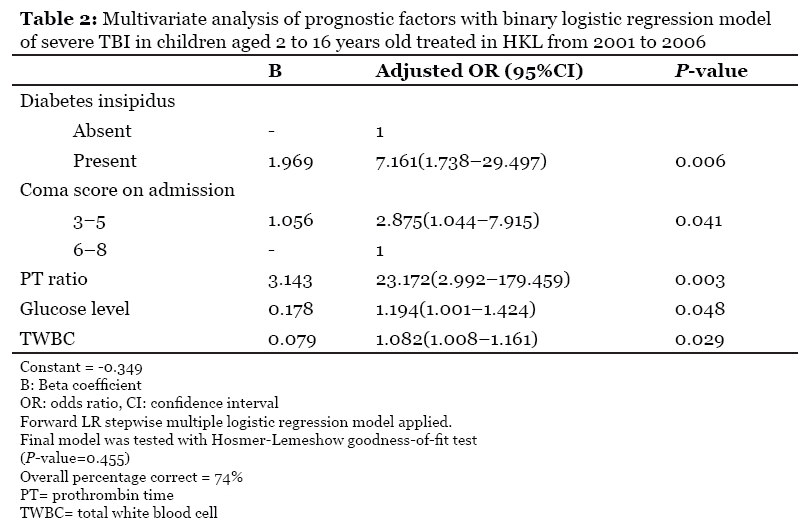
Malaysian Journal of Medical Sciences , Vol. 16, No. 4, Oct-Dec, 2009 pp. 25-33 ORIGINAL ARTICLE Prognostic Factors of Severe Traumatic Brain Injury Outcome in Children Aged 2-16 Years at a Major Neurosurgical Referral Centre Choon Hong Kan1,2, Mohd Saffari1,2, Teik Hooi Khoo1,3 1 Department of Neurosurgery, Hospital Kuala Lumpur, Jalan Pahang, 50586 Kuala Lumpur, Malaysia Submitted: 30 Jun 2009 Code Number: mj09030 Abstract Background: Traumatic Brain Injury (TBI) in children has been poorly studied, and the literature is limited. We evaluated 146 children with severe TBI (coma score less than 8) in an attempt to establish the prognostic factors of severe TBI in children. Keywords: severe traumatic brain injury (TBI), children, prognostic factors, Pediatric Cerebral Performance Categories Score, neurosciences Introduction Traumatic brain injury (TBI) is one of the leading causes of death and disability in the paediatric age group. In developed countries, paediatric trauma mortality still represents more than half of all childhood fatalities: 18 times more common than brain tumours (1). However, many aspects of paediatric neurotrauma still remain unclear as the literature focusing on the paediatric population per se is very limited. In fact, guidelines for management of paediatric TBI were mainly derived from adult guidelines (2). The fact that paediatric TBI patients are more prone to develop brain swelling support the idea that maturing brain reacts to insult in a different way (3). Several prognostic factors, such as age group, gender, pupillary reactivity, Glasgow Coma Score (GCS) on admission, serum glucose level, total white blood cell (TWBC) counts, platelet counts, coagulation derangement, computerised tomography (CT) scan features and grading, have been validated in various studies to predict outcome in adult neurotrauma. However, the impacts of these factors are poorly understood in paediatric TBI. The predictive value of GCS was reported to be low in one local paediatric TBI study (4). Not infrequently, those with GCS scores of 3 to 5 upon admission may still recover with independent function (5). The role of glucose level is somewhat controversial in the paediatric neurotrauma literature (6). Parish et al. reported that hyperglycaemia was not a poor prognostic factor in paediatric TBI, as is true in the adult population (7). However, Michaud et al. later demonstrated that hyperglycaemia was associated with poor neurological outcome in a larger series (8). Cochran et al. observed that paediatric severe TBI patients with admission serum glucose levels > 300 mg/ dL (16.65 mmol/L) were uniformly more prone to death (9). Chiaretti et al. found that delayed activated partial prothrombin Time (aPTT), low platelet count, elevated fibrin-fibrinogen degradation products (FDP) and low fibrinogen were associated with poor outcome in their paediatric TBI series, which consisted of 60 patients. Kuo et al. however, demonstrated that only FDP > 1000 μg/mL upon admission to the hospital in children with GCS scores of 7–12 was associated with a poor outcome (10). Most subjects in the series on prognostic factors were from developed countries with sophisticated systems of regional organization coupled with experienced trauma centres, which allowed for rapid evacuation, monitoring and treatment of these patients (11,12,13). Experienced staff and equipment such as ventilators and intracranial monitoring are still luxury items in Malaysia. The aim of this study is to identify factors associated with the outcome of paediatric severe TBI that can be identified early, during the first few hours after admission. We hope to use these findings to predict the outcome of severe TBI to guide treatment strategies in Malaysia. Materials and Methods We performed a cross-sectional analysis investigating children aged between 2 to 16 years presenting with severe TBI treated in Kuala Lumpur Hospital (HKL) from January 2001 until December 2006. Patients were managed according to a standard departmental protocol that includes artificial ventilation and sedation with midazolam/ morphine infusions. Patients were positioned in the supine position with the head elevated 30 degrees. The following parameters were kept within the desired ranges: temperature < 37.0 °C; partial pressure of carbon dioxide (paCO2) 35–45 mmHg; intracranial pressure (ICP) < 20 mmHg; cerebral perfusion pressure (CPP) within 60–70 mmHg. We also performed surgical evacuation and decompression for lesions with mass effects and decompressive craniectomy for refractory intracranial hypertension. Data regarding initial coma score, pupillary reactivity, motor score, presence of hypotension (defined as less than the 5th percentile according to age-appropriate systolic blood pressure [AASBP]) and development of diabetes insipidus (DI) within 3 days were retrieved from hospital notes. Laboratory results for serum glucose, prothrombin time (PT) and aPTT ratio, international normalized ratio (INR), platelet counts and TWBC upon admission were recorded. CT scans were graded according to the Marshall classification, the presence of brain swelling, traumatic subarachnoid haemorrhage and intraventricular haemorrhage. Peak ICP and lowest CPP were recorded for those patients who had undergone ICP-CPP targeted therapy. Outcomes at 6 months were assessed with the Pediatric Cognitive and Performance Categories (PCPC) scale. Patients were categorised as having a “good outcome” or a “poor outcome”. Data entry and analysis were done using the Statistical Package for Social Sciences (SPSS) version 12.0. We used logistic regression to develop a model of risk factors for poor outcome from paediatric severe TBI. Independent variables were entered into the logistic model in a stepwise fashion with a significance cut-off of P < 0.25. We interpreted a P-value of less than 0.05 as significant at a 95% confidence interval (CI). Hosmer-Lemeshow goodness-of-fit testing established the best model— forward likelihood. The research protocol was approved by the ethical committee of Universiti Sains Malaysia in 2006. Results One hundred and sixty-seven children with severe TBI were admitted to HKL neurosurgical intensive care unit (ICU) between January 1 2001 and December 31, 2006, after exclusion criteria applied. Only 146 patients out of 167 were included in the study as the rest were lost upon follow up. The median age of patients was 13 years with a mean of 11.7 years and standard deviation of 4.2 years. The majority of the patients (133, 91.1%) were older than 4 years; 13 patients (8.9%) were less than 4 years; 123 patients (84.3%) were male and 23 (15.7%) were female. The majority of the patients (107, 73.3%) were of Malay origin. Eighty-nine cases (61%) had good outcomes according to the PCPC scale at 6 months. There were 35 cases of deaths (24%). Most of the cases were referrals from other centres (83.6%); 24 cases (16.4%) were direct admissions. The most common mechanism of injury was road traffic accidents (RTA), which accounted for 118 cases (80.8%); followed by fall from height, 14 cases (9.6%); 8 cases of unknown mechanism (5.5%); 2 cases from contact sports (1.4%) and another 2 cases from assault (1.4%). Univariate analysis of outcome showed statistically significant differences in AASBP (P = 0.006), coma score on admission (P = 0.038), motor response (P = 0.007), pupillary reactivity in those with equal and not dilated pupils (P = 0.001), presence of DI (P < 0.001), serum glucose level (P = 0.001), TWBC counts (P = 0.043), aPTT ratio (P = 0.03), PT ratio (P < 0.001), INR (P = 0.009), peak ICP value (P = 0.028), minimum CPP value (P = 0.001), Marshall CT grading (P = 0.025), presence of brain swelling (P = 0.009) and presence of IVH (P = 0.042). ICP monitoring and ICP-CPP directed therapy were only available in 39% of severe TBI in children aged 2–16 years old during the study period. These measures were not included in the logistic model. The multivariate logistic regression model with the forward LR (likelihood ratio) method concluded that coma score on admission (odds ratio [OR], 2.88; 95% confidence interval [CI], 1.04–7.92), presence of DI (OR, 7.16; 95% CI, 1.74– 29.50), PT ratio (OR, 23.17; 95% CI, 2.99–179.50), glucose level (OR, 1.19; 95% CI, 1.00–1.42) and TWBC counts (OR,1.08; 95% CI, 1.01–1.61) upon admission were predictors of outcome in paediatric severe TBI. The odds of having poor outcome are 7.2 times higher in those who develop DI within the first 3 days following TBI (OR, 7.16; 95% CI, 1.74– 29.50). The odds of having poor outcome if the admission coma score was 3 to 5 is almost 3 times (OR, 2.88; 95% CI,1.04–7.92) higher than those with admission coma score of 5 to 8. Every increase in PT ratio of 0.1 significantly increases the odds of a poor outcome by almost 2.3 times; the change can be as little as 2.99 and as high as 179.46 at the 95% confidence level. The odds of poor outcome is 1.2 times greater with every increase of 1 mmol/L in glucose level upon admission and the change can be as little as 1.01 and as high as 1.42 (95% CI). Every increase in TWBC by 1 x 103 mm3 increases the odds of a poor outcome by 1.1-fold; the change can be as little as 2.99 and as high as 179.46 (95% CI). Discussion Sixty-one percent of severe TBI children achieved good outcome at 6 months in our series. This was slightly better than the outcome of adult severe TBI in Singapore, which was reported to be 51.2% (14). Immature brain has greater neuroplasticity as compared to adults, and this property will be lost due to myelination as patients grow (15,16). However, the percentage of good outcomes was reported to be as high as 90% in the literature (17). The higher rate is probably because other studies on TBI in paediatric patients included mild, moderate and severe cases of TBI. Our analyses did not find any association between age groups and outcome. This finding did not support the classic paediatric neurotrauma paper by Levin et al. (12). A recent study in the Indian population also failed to demonstrate age less than 4 as a factor affecting outcome (18). Poor outcome in those less than 4 years old of Levin’s series is probably due to the high occurrence of non-accidental injury (NAI) in that age group. NAI is often associated with poor outcome as reported in the literature (19). There were no cases of NAI during the period of study in children aged 2–16 years old after excluding those less than 2 years old. Furthermore, the four centres involved where Traumatic Coma Data Bank (TCDB) data were collected were actually treating a small percentage of all the paediatric TBI during the study period. Therefore the sample was not truly representative. We found no significant difference between outcome and gender in our study on severe TBI. Although Kraus et al. have reported 1.75 times greater risk for poor outcome in adult females, they actually included both moderate and severe TBI patients (20). Our findings support the more recent study on gender differences in outcome in an Asian population that included both adult and paediatric groups (21). The coma scale that we used (Modified Glasgow Coma Scale for those > 3 years old and Children’s Coma Scale for those < 3 years old) was reliable in predicting outcome in severe TBI in children. This modified scale is more appropriate in children as the total score for each component was equivalent to that obtained with the GCS, which made comparison with adult literature possible. The reliability of GCS in children with TBI has been questioned from time to time as it has great interobserver discrepancies (4,5) Motor score upon admission was associated with poor outcome in univariate analysis but not observed in the logistic model after various variables were fixed. There is no doubt that early hypotension contributes to secondary brain injury and subsequent poor outcome (22). Only eight cases (5.5%) had systolic blood pressure (SBP) less than AASBP upon admission in our series. This is probably due to the fact that most of our patients were referred from other hospitals (84.6%); those who were haemodynamically unstable would have been managed in other hospitals as they were not fit for transportation. Our univariate analysis did show that hypotension (defined as less than the 5th percentile of AASBP by the Brain Trauma Foundation in 2000) was associated with poor outcome; however this was not demonstrated in multivariate analysis. We suggest that the definition of hypotension in children in the context of TBI should be reconsidered. Vavilala et al. retrospectively reviewed the effect of various AASBP percentiles on outcome in children less than 14 years old and found that those with AASBP < 75th percentile (instead of 5th percentile) were more likely to exhibit poor outcome, even when SBP was more than 90 mmHg. The values of SBP in the National Task Force table have been derived from normal children and were according to their height. The cut-off point for hypotension in children with severe TBI should be set higher, probably at the 50th or 75th percentile of the SBP table by the National Task Force, or should be based on tables with values derived from critically ill or headinjured children. The recently published IMPACT study also called for reconsideration of SBP in the adult guidelines (23). They found that the outcome improved as SBP increased up to 135 mmHg. ICP monitoring was available in 39% of severe TBI in children aged 2–16 years old during the period of study in HKL. In fact, Morris et al. reported that 59% of total severe TBI (children and adults) received ICP-CPP directed therapy in the UK. There were significant variations in the management of intracranial hypertension (24). From univariate analysis, peak ICP and minimum CPP values were associated with poor outcome at 6 months. The mean ICP of the good outcome group was 26.4 mmHg (P-value = 0.028), which is higher than the classical threshold for treatment for intracranial hypertension (20–25 mmHg). Minimum CPP values appeared to be more significant than ICP with P-value of 0.001. Thus, in selected cases, a higher limit of ICP may be acceptable as long as an adequate CPP can be maintained, as has been suggested in the adult guidelines for managing severe TBI by the Brain Trauma Foundation (BTF). There might also be age differences in the specificity of ICP and CPP in association with outcome as pointed out by Chambers et al. (25). Studies on the predictive value of ICP and CPP in terms of outcome can only be done in centres where all the severe TBI patients (coma score <8) are subjected to ICP-CPP directed therapy. Our study also demonstrated that children with severe TBI who developed DI within 3 days post-trauma have a mortality rate of 71%. Boughey et al. reported a higher mortality rate of 86% in their study on 2014 patients of TBI from all age groups (26). There were 4 patients who developed DI within 3 days post-TBI who eventually exhibited good outcomes. This group might represent those with pure skull base injury or injury to the posterior pituitary instead of flow problems due to elevation in intracranial pressure or restriction of flow to the hypothalamic-pituitary axis due to cerebral oedema (27). Our study confirms the deleterious effect of glucose on injured paediatric brain. The IMPACT study also demonstrated similar linear associations with outcome in the adult TBI population (28). Studies have shown that hyperglycaemia exacerbates the impact of ischemia and hypoxia in the injured brain, worsening secondary brain damage. The mechanisms involved include hyperosmolarity, lactic acid production, alterations in neuronal pH and increased excitatory amino acids. Researchers have shown substantial reduction in mortality in critically ill patients (non-diabetic) treated with early intensive insulin therapy (29). Further study on the effect of aggressive glucose normalization in the management of children with severe TBI should be carried out. The importance of coagulopathy in paediatric TBI is increasingly being recognised (11,18,30,31). In view of the high incidence of coagulopathy in paediatric severe TBI, routine laboratory screening of coagulopathy was considered cost effective and has become standard practice in some centres as a component of the initial work-up of paediatric age group TBI (31). Chiaretti et al. suggested that d-dimer, FDP and fibrinogen be included as an initial screening test in paediatric TBI (30). At our centre, baseline coagulation tests were done on those with children with severe TBI. This included PT ratio, INR, aPTT ratio and platelet count. d-dimer, FDP and fibrinogen levels were not routinely available in our centre. Among the coagulation markers in our study, only PT ratio was associated with poor outcome with a high degree of accuracy in the multivariate study. aPTT ratio was associated with poor outcome in univariate analysis but not in the logistic model. PT ratio instead of aPTT ratio is crucial in determining outcome. This is explained by the fact that the coagulation cascade is initiated by the release of thromboplastin from the damaged brain tissue, which primarily activates the extrinsic clotting cascade and not the intrinsic pathway (32). In fact, brain tissues have the highest level of thromboplastin as compared to any other tissue in the body (33). The IMPACT study in adult TBI demonstrated prognostic effects of PT and platelet count, only among other coagulating factors (28). They also emphasised the importance of correcting coagulopathic syndromes and called for further vigorous study on outcome with treatment of these abnormal values. The pathophysiology of hypercoagulation state in TBI is multifactorial and rather complex. Blood loss due to systemic or cranial injury may induce bleeding diasthesis by depleting platelet and clotting factors whereas the injured brain may itself induce a hypercoagulation state by releasing the pro-coagulant tissue factor thromboplastin. The fact that platelet counts were not associated with outcome in paediatric TBI is explained by the fact that platelet counts are usually higher in this age group. Leukocytosis was found to be an independent predictor of outcome in children as reported in the adult literature. This is the first series evaluating the impact of TWBC counts in predicting outcome in children with severe TBI. The adult series also observed a significant correlation between coma score on admission and higher TWBC counts in severe TBI (34). However, the IMPACT study did not include TWBC counts in their analysis of prognostic value of laboratory parameters in adult TBI (28).The fact that TBI in children was associated with decreased cell-mediated immunity further complicates the issue (35). Neutrophil count would probably be a better predictor of outcome in TBI than TWBC counts. Cerebral swelling (corresponding to Marshall Grade III) was present in 48.6% of the patients during the study period. This figure is similar to that in the paediatric literature, with a range of 26%–44% (36,37). Although the significance of cerebral swelling in paediatric TBI has been controversial, our study demonstrates cerebral swelling was associated with poor outcome in only 44% of patients (32 out of 72 patients). The fact that cerebral swelling was not associated with poor outcome in multivariate analyses supports the notion that the mechanism of cerebral swelling is probably different and less malignant than the mechanism in adults, which has consistently been associated with poor outcome in the literature (38). Marshall classification did not significantly affect outcome in multivariate analyses. This could be due to the high occurrence of cerebral swelling corresponding to Marshall Grade III in paediatric TBI. The analysis of Marshall classification in our study is limited by the definition of mass and diffuse lesions, especially in those cases with a combination of both. Some surgeons would operate upon diffuse injuries with small components of mass lesions in the critical region. According to the Marshall classification, the grading of mass lesions is performed according to the serial CT scan performed within 12 hours after the surgery. This was not done routinely in all our post-operative patients, mainly because of limited resources. A recent study suggests that combinations of individual CT predictors rather than Marshall classification were more reliable for prognostic purpose in adult TBI (39). The IMPACT study demonstrated that CT scan characteristics were important predictors of outcome in adult TBI; those characteristics include class III and IV diffuse injury, brain swelling and the presence of traumatic subarachnoid haemorrhage (tSAH) (40). The presence of tSAH and IVH were found not to predict the outcome of paediatric TBI. Conclusion Our series represents one of the largest series of severe TBI in children in our region and represents the urban Malaysian population. We have concluded from multivariate analyses that low coma score at admission, development of hyperglycaemia, leukocytosis and prolonged PT ratio serve as useful indicators in predicting outcome in children with severe TBI, aged 2–16 years old (Table 2). The roles of AASBP, Marshall grading, presence of cerebral swelling and IVH were not established in the logistic regression model, although these have shown significance in univariate analysis (Table 1 part A and part B). Age and gender do not affect outcome in severe TBI in children. ICP and CPP could not be included in our analyses as only selected cases received ICP-CPP targeted therapy during the period of this study. The use of coma scale in children must be according to developmental age and comparable with the adult GCS. The measurement of coma score should be standardised to avoid confusion in analysis of the neurotrauma literature. By using modified GCS for those older than 3 years old and CCS for those younger than 3 years old, we have demonstrated that coma score can predict outcome in children with TBI. The definition of hypotension in children with TBI based on AASBP should be reconsidered. Values derived from those critically ill or TBI patients should be made available. Coagulation derangement (prolonged PT ratio) predicts outcome better than other laboratory parameters such as glucose and TWBC (odds ratio of 2.3 compared to 1.2 and 1.1), thus full coagulation profiles that include d-dimer, FDP and fibrinogen level should be available during initial work-up in severe TBI patients. This study demonstrates preliminary evidence of a relationship between the various factors predicting outcome in children with severe TBI. A prospective trial confirming our findings is needed in the future before we can make definitive recommendations regarding patient management. Our results have the potential to impact future patient management protocols in severe TBI in children, as well as to aid in the design of neuroprotective trials. If prospective trials confirm our findings on hyperglycaemia and coagulopathy, then aggressive and early control of glucose level with insulin and normalization of PT ratio with fresh frozen plasma would become standard practice in children with severe TBI. Author’s contributions Collection and assembly of data, provision of study materials or patients: CHK, MS All authors have contributed equally to the conception and design, critical revision of the article. References
© Copyright 2009 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj09030t1a.jpg] [mj09030t2.jpg] [mj09030t1b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}