 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
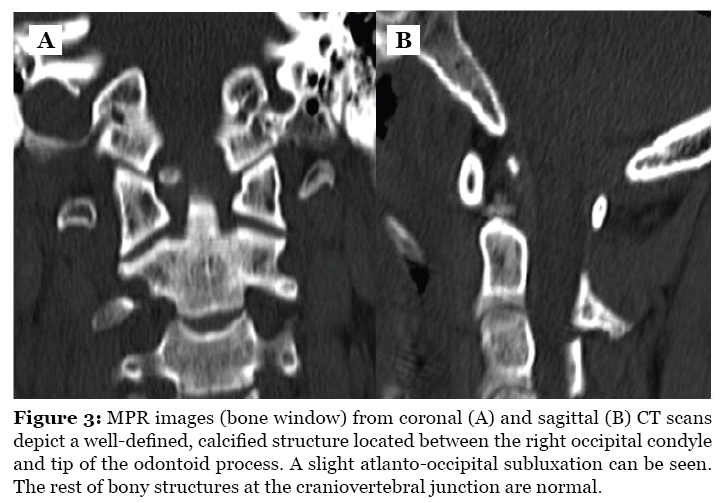
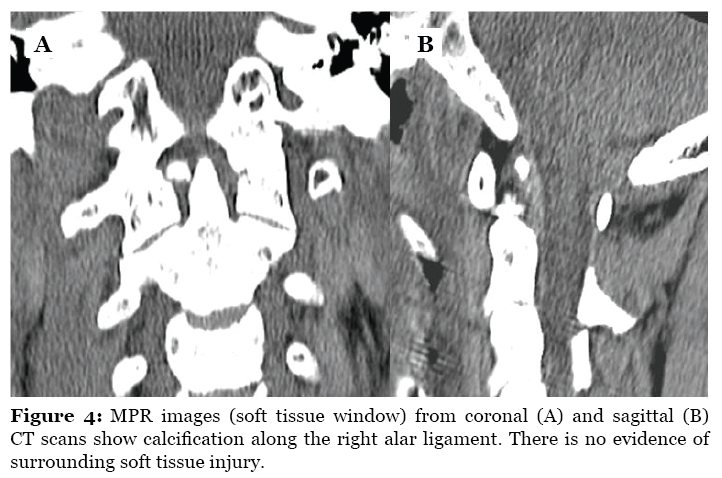
Malaysian Journal of Medical Sciences , Vol. 16, No. 4, Oct-Dec, 2009 pp. 69-72 CASE REPORT Calcification of the Alar Ligament Mimics Fracture of the Craniovertebral Junction (CVJ): An Incidental Finding From Computerised Tomography of the Cervical Spine Following Trauma Siti Kamariah Che Mohamed, Azian Abd. Aziz Department of Radiology, Kulliyyah of Medicine, International Islamic University Malaysia, 25710 Kuantan, Pahang, Malaysia Submitted: 2 Jul 2009 Code Number: mj09036 Abstract When performing a radiological assessment for a trauma case with associated head injury, a fragment of dense tissue detected near the craniovertebral junction would rapidly be assessed as a fractured bone fragment. However, if further imaging and evaluation of the cervical spine with computerised tomography (CT) did not demonstrate an obvious fracture, then the possibility of ligament calcification would be considered. We present a case involving a previously healthy 44-yearold man who was admitted following a severe head injury from a road traffic accident. CT scans of the head showed multiple intracranial haemorrhages, while scans of the cervical spine revealed a small, well-defined, ovoid calcification in the right alar ligament. This was initially thought to be a fracture fragment. Although such calcification is uncommon, accident and emergency physicians and radiologists may find this useful as a differential diagnosis in patients presenting with neck pain or traumatic head injury. Keywords: cervical spine, calcification, computerised tomography, injury, medical sciences Introduction Calcification in the region of the upper cervical spine is rare, although a few cases have been reported involving calcification of the alar or transverse ligament of the atlas. The calcification usually develops as a result of traumatic injury or inflammatory disease and is especially prominent in the elderly (1–3). In patients with a history of trauma, alar ligament calcification can mimic a fracture of the craniovertebral junction (CVJ). As an uncommon normal variant, it is important for accident and emergency physicians; and radiologists, to be able to distinguish such calcification from a fracture. We present a head injury case where the calcification was only incidentally detected and was initially thought to be a fracture fragment. Case Report A 44-year-old man who was involved in a road traffic accident (RTA) was admitted for deterioration in his level of consciousness. An urgent cranial computerised tomography (CT) scan showed a large right temporoparietal extradural haemorrhage (EDH), a left temporal hemorrhagic contusion and multiple skull vault fractures. Due to the severity of the head injuries, a CT scan of the cervical spine was also performed. A small, well-defined region of calcified tissue was detected between the odontoid tip and the right occipital condyle (Figure 1). The pre-vertebral soft tissue at the upper cervical spine was not thickened (measuring about 4.6 mm at the C2 level on the mid sagittal multiplanar reformat [MPR]). There was no indication of occipito-atlanto dissociation (the basion-dental interval measured 4.3 mm, which is within the accepted normal range) (Figure 2). The rest of the cervical spine seemed undisrupted. In view of the RTA and severity of the head injuries, a fracture at the CVJ was initially suspected. However the origin of the fractured fragment could not be determined. On comparison with sagittal and coronal MPR images (Figure 3 A & B), a well corticated structure (measuring about 6.5 x 3.8 x 4.0 mm) was identified between the right occipital condyle and odontoid tip. This indicated that the anomaly was a calcified structure rather than a fragment of bone. The adjacent occipital condyle, odontoid process and neural arch of the atlas showed smooth and well defined outlines. The soft tissue window (Figure 4 A & B) showed the calcification was within the right alar ligament. Unfortunately, due to the severity of the head injuries, and despite evacuation of the intracranial haemorrhages, the patient succumbed ten days later. Discussion The alar ligaments originate bilaterally from the odontoid process and run cephalad and laterally to reach the medial aspect of the occipital condyle. They are strong, rounded structures that play an important role in stabilising the head during rotary motion of the CVJ. These ligaments can be easily studied using high-resolution magnetic resonance imaging (MRI) that includes a proton attenuation weighted sequence. The orientation of the alar ligaments is highly variable and asymmetry is common in asymptomatic individuals (3,4). Calcification in the alar ligament is very rare. It usually develops with increasing prevalence after the age of 40 and tends to occur following minor trauma or as a consequence of inflammatory disease (1–3). In our case, the calcification was observed in the right alar ligament, which is similar to the findings of Sim and Park (1). They detected a nodular calcification in the periodontoid area on the initial axial CT scan performed on their patient following a severe head injury. They had also considered the possibility of a fracture involving the odontoid process (type I fracture), the occipital condyle (type III fracture) or the neural arch of the atlas at the CVJ. MPR, MRI and a 3D-CT scan of the cervical spine were performed for further evaluation of the anatomy of the calcified structure. Serial, open-mouth views and dynamic radiographs of the cervical spine demonstrated a stable cervical spine and a persistent, constant crosssection calcification. On the basis of this series of examinations, they concluded that the nodular calcification occurred in the right alar ligament and was unrelated to trauma or inflammation and, therefore, was an incidental finding (1). Kobayashi et al. (2) also reported calcification of the alar and transverse ligaments of the odontoid process in two patients presenting neck pain. Both patients had pharyngodynia and prior nuchal pain without previous history of trauma, and their symptoms had improved gradually with an anti-inflammatory drug therapy and neck immobilisation. CT scans revealed a nodular calcification in one patient and a poorly delineated calcified lesion surrounding the odontoid process in the other patient. Serial CT scans demonstrated that the calcifications shrank and disappeared with time. The authors assumed that the patients’ symptoms could be related to an inflammatory reaction induced by deposition of calcium since secondary arthritis was not observed, and the symptoms subsided as the lesions decreased in size (2). In our case, a cervical CT scan, performed to assess head injury, revealed a small, well-defined, ovoid of high-density tissue in the right periodontoid area along the course of the alar ligament. Initially, we also considered the possibility of it being a bone fragment, but comparison with the MPR images was helpful in ruling this out. The calcified fragment was well corticated and the surrounding bones of the CVJ were well defined. There was no convincing evidence to show that the tiny fragment originated from any of the bones of the CVJ. No cervical fracture was identified. Furthermore, there was no evidence of soft tissue injury or indications of inflammation or arthritic changes accompanying the calcification. In view of this, we concluded that there was a calcification in the right alar ligament that was unrelated to the current trauma (making it an incidental finding). Unfortunately, the patient’s conditions worsened and we were not able to perform other imaging such as MRI. From our extensive literature review, there are few case reports of focal or nodular calcification of the alar ligament; only those reported by Sim and Park (1) and Kobayashi et al. (2) were found. A condition called crowned dens syndrome, describing neck pain due to calcifications surrounding the odontoid process, has previously been reported in conjunction with calcium hydroxyapatite (HA) and calcium pyrophosphate dehydrate (CPPD) crystal deposition diseases. In CT scans, the calcifications in these instances are seen to surround the top and sides of the odontoid process in a crown or halo-like distribution and commonly affect the transverse ligament (5,6). In our case, the calcification was focal and nodular and lay along the anatomical location of the alar ligament. In conclusion, calcification of the alar ligament should be considered as a differential diagnosis in a traumatic craniovertebral injury, and this is especially true when the origin of a fracture is not clearly identified. Proper diagnosis is important because the treatment, which is beyond the scope of this paper, differs from fracture treatment and prevents unnecessary, prolonged, external immobilisation of the neck. Having said this, fracture of odontoid process (type I) and the occipital condyle (type III) should be carefully assessed and excluded if a bony fragment is detected, particularly in of the case of trauma. Author’s contributions Conception and design, analysis and interpretation of data: SKCM, AAA Data collection, drafting of the article, provision of study materials and patients: SKCM Critical revision, and final approval of the article: AAA References
© Copyright 2009 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj09036f2.jpg] [mj09036f1.jpg] [mj09036f3.jpg] [mj09036f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}