 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 17, No. 2, 2010, pp. 4-9 Original Article Observation of Ureteric Diameter in Negative Intravenous Urogram in Hospital Universiti Kebangsaan Malaysia Siong Lung WONG1, Hamzaini ABDUL HAMID2 1Department of Radiology, Faculty of Medicine and Health Sciences, Universiti
Malaysia Sarawak, Lot 77, Seksyen 22, KTLD; Jalan Tun Ahmad Zaidi Adruce, Correspondence: Dr Wong Siong Lung, MD (UKM), MMed (Radiology) (UKM), Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak, Lot 77, Seksyen 22, KTLD, Jalan Tun Ahmad Zaidi Adruce 93150 Kuching, Sarawak, Malaysia, Tel: +6082-292 267 Fax: +6082-422 564, E-mail: slwong@fmhs.unimas.my Submitted: 18 Aug 2009 Code Number: mj10014 Abstract Background: This study observed the widest ureteric diameter in negative intravenous
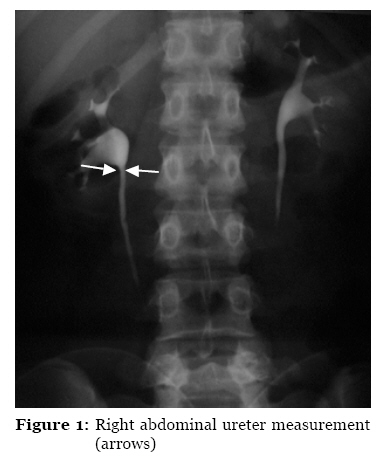
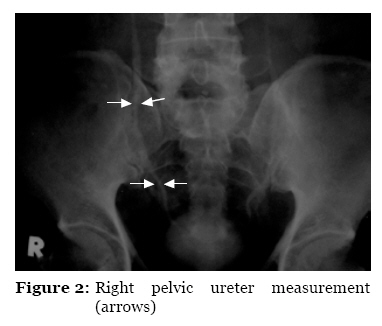
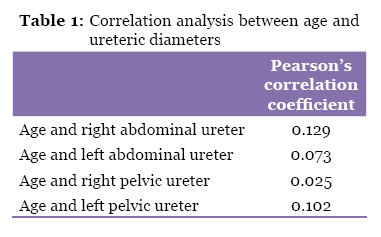
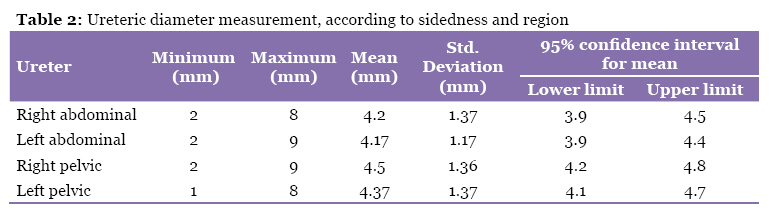
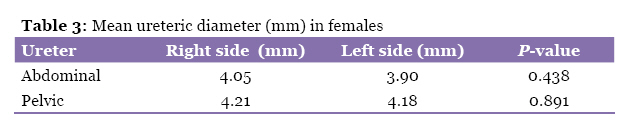
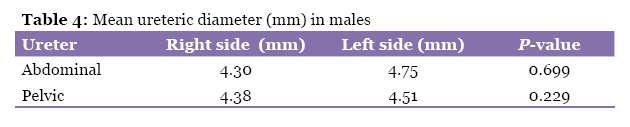
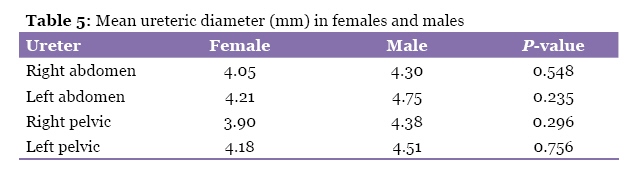
urogram (IVU) examinations using low osmolar contrast media. Keywords: low osmolar contrast media, negative intravenous urogram, ureteric diameter, medical sciences Introduction Assessment of ureteric diameter is important in the diagnosis of urinary diseases. Intravenous urogram (IVU) remains as one of the few modalities that can reliably study the entire course of the ureters. Ureteric dilatation is an important secondary sign that can identify a diagnosis of stone disease even when a stone has recently passed. Chronic vesicoureteric reflux and congenital anomalies of the urinary tract (e.g., posterior urethral valves, megaureter, and prune-belly syndrome) may also result in dilatation of the ureter. Similarly, infectious processes (e.g., Escherichia coli, Pseudomonas, and Citrobacter) can impair ureteric peristalsis, causing ureteric dilatation (1). Inflammatory processes adjacent to the ureter may also impair ureteric peristalsis and result in ureteric dilatation (2). Compression of the ureter by a pelvic or an abdominal mass can cause unilateral or bilateral dilatation of the ureter. Current information about ureteral diameter adopted by most radiological textbooks is mostly from papers published in the 1970’s and has quoted a maximal ureteric diameter of 7mm, solely based on research in non-pregnant female populations (3,4). A recent review of literature on the techniques and interpretation of IVU also briefly mention that a diameter of less than 8mm is generally considered to be normal (5). But the reference from which this observation is made is also from a study performed more than 30 eyars ago in which low osmolar contrast media (LOCM) were not commonly used due to the high cost (even in the 1990s, there was only approximately a 50% of penetrance of LOCM into the market) (6). In view of current IVUs which are all carried out using LOCM, a refined observation of ureteric diameter is deemed appropriate as in theory, non-ionic LOCM exerts only a third of osmotic pressure of conventional ionic contrast media. The result therefore should be that of reduced distension of the ureters, compared to high osmolar contrast media. A study of ureteric diameter in infants and young children (up to 16 years of age) has identified linear relationships between advancing age, the height of the lumbar vertebra and ureteric diameter (8). Reviews of literature showed that there has not been a study that looks into the relationship between ureteric diameter and age in an adult population. It is a commonly recognized fact that pregnancy is associated with upper urinary tract dilatation due to both physiologic processes and compression of the urinary system by the gravid uterus. The right collecting system was larger in 86% of the affected subjects while the left side was affected in 10% of the subjects (7). It usually occurs during midterm of pregnancy, which is thought to be due to the dextrorotation of the uterus (urologic process during pregnancy). Some authors also assume that such dilatation is not transient but persists long after the post-partum period (3,7). This study is therefore aimed at providing information about the mean ureteric diameter in negative IVUs to determine if there is a correlation between age and ureteric diameter in an adult population and to ascertain if there is significant difference between the right and left ureteric diameters in male and non-pregnant female patients. Material and Methods This study was conducted in the Department of Radiology, Hospital Universiti Kebangsaan Malaysia (HUKM). All patients had undergone intravenous urograms in the radiology department for routine and urgent clinical indications from period of 1 January, 2004 until 31 September, 2006 and fulfilled the inclusion criteria were included in this study. A negative study was defined as an examination that failed to yield positive findings suggesting primary or secondary diseases involving the ureter, such as: obvious dilatation and/or tortuousity of the ureter; asymmetry of right and left ureter; an increasing, dense nephrogram; kidney enlargement; delay calyceal opacification; pelvicaliectasis; a standing column of contrast; a filling defect within the ureter or pelvicalcyceal system; and spontaneous pyelosinus extravasation. All negative IVUs included in this study were verified by two independent, qualified radiologists. Patients with the following exclusion criteria were excluded: history of pregnancy within three months, diagnosed with bladder calculus disease, renal failure, diagnosis of urinary tumour of any type, stenosing ureteric disease, inadequate visualization of the entire ureter on the IVU, and poor opacification of the urinary collecting system. Non-Malaysian foreigners were also excluded. Equipment The X-ray apparatus used in this study was a Siemens overhead couch units model (8375040 G2107). IVU was performed with no fluid restriction but with standard oral preparation with diet modification and a prescription of laxatives (bicasodyl) two days prior to the examination. Control films were taken in all patients before injection with contrast material (Omnipaque, Iohexol 300) at dose of 1–2mL/kg body weight. All films were taken at a standard of 100 cm FFD, with the centering ray at the iliac crests for full-length films. Full-length films were taken five minutes post-injection. Abdominal compression was then applied and a 10-minute renal area radiograph was obtained. A 15-minfull-length film was taken after the release of compression; any subsequent films were taken at the discretion of the supervising radiologist/attending medical officer. The mean abdominal ureteric diameter was defined as the largest transverse dimension within 6 cm from the pelviureteric junction (PUJ), measured on either on 5-minute film or compressed film, whichever measurement was larger, in accordance with the method adopted by Bradley et al. (4,8). The PUJ is defined as the transition between the renal pelvis and upper ureter. Mean pelvic ureteric diameter was defined as largest the transverse dimension from the level of sacrum to its insertion point in the urinary bladder, measured either in 5-minute or released film, whichever measurement was larger. All measurements were made with aid of a 5x magnifying glass and a standard transparent ruler. Results A total of 92 patients were included in this study. The mean age of the study population was 40.6 ± 14 years (range 14–70 years). There were 53 males (57.6%) and 39 females (42.4%). The racial distribution in this study mirrored the racial distribution typically found in this community, 77.2% were Malays; 16.3% were Chinese; and 6.5% were Indians. Correlation between ureteric diameter and age Data on abdominal and pelvic ureteric diameter was plotted against subject age in a scatter plot. Pearson’s correlation test indicated poor correlation between age and ureteric diameter, as summarized in Table 1. Mean ureteric diameter The measurement of the abdominal and pelvic ureter divided into the right and left side ranges from 1 to 9 mm, as summarized in Table 2. Measurement according to gender There were 53 males and 39 females in this study. The mean right and left ureteric diameters of male and female were analysed with independent T-tests to ascertain any significant differences between them. Female The mean of the right abdominal ureteric diameter was 4.05 mm and the left was 3.90 mm. The mean of the pelvic ureteric diameter was 4.21 mm on the right and 4.18 mm on the left (Table 3). Although both the right abdominal and pelvic ureters appeared to be larger than the left, the difference is not statistically significant, with a P-value of 0.438 for the abdominal ureter and 0.891 for the pelvic ureter. Male The mean of the right abdominal ureteric diameter was 4.30 mm and the left was 4.75 mm. The mean of the pelvic ureteric diameter was 4.38 mm on the right and 4.51 mm on the left (Table 4). Although the left abdominal ureter appeared larger than the right, and the right pelvic ureter appeared larger than the left, the difference was not statistically significant, with a P-value of 0.699 for the abdominal ureter and 0.229 for the pelvic ureter. Female/Male Differences The means of measured ureteric diameters appeared to be larger in male subjects for both the right and left abdominal and pelvic ureters, compared to their female counterpart (Table 5). Comparing the means of right abdominal ureter, left abdominal ureter, right pelvic ureter and left pelvic ureter between female and male subjects using independent T-test, there is no significant difference between right and left abdominal as well as pelvic ureter for both the sexes. Discussions In the genitourinary system, it is known that the kidney size continues to grow until the seventh decade of life, when it starts to shrink (9). As for the ureter, previous research has documented that the ureteric diameter increases with age until 16 years of age (8). However, no previous study has examined if there is a significant change in ureteric diameter with age. It has been assumed that the ureteric diameter could be wider in the elderly due to laxity of the smooth muscles, similar to those of the common biliary duct. However, the findings in this study demonstrated that in an adult population, there is no progressive increment in ureteric diameter up to the seventh decade. This is an important finding, as the ureter is a structure for which measurement of its diameter reveals information regarding its condition. Combining data from this study with those of previous similar studies, it can therefore be concluded that the ureter reaches its maximum diameter at the end of growth spurt in the teenage years. Other intravenous urogram studies have cited different numbers. These figures range from as small as 2mm to as large as 8mm (3,4,5). Some of these figures are derived from a study of a specific sample population e.g., from post-partum females (3,4,5). Anecdotal observation of the ureteric diameter in IVUs is suggests that the actual number is less than that described in previous reports citing 7 or 8 mm (3,5). In light of current IVU studies using LOCM—versus 1970s studies using HOCM (3,5)—a new study is deemed necessary, as LOCM should, in theory, produces less distension of the ureters, in comparison to HOCM (5). Findings from the data collected in this study suggest that mean of the abdominal ureteric diameter is 4.19 mm, with an SD of 1.27 mm, and the mean for pelvic ureter is 4.45 mm, with an SD of 1.37 mm. The upper limits of the abdominal and pelvic ureters are 4.37 mm and 4.64 mm respectively, calculated to be within the 95% confidence interval for the given means. A maximal diameter of 7 and 8 mm (suggested in previous papers as being normal) may no longer be acceptable (3,5). These study findings are also supported by the work of Zelenko and colleagues, who observed a mean diameter of 1.8 mm with standard deviation of 0.9 mm, after having examined 212 patients who had undergone CT examinations (10). Even with radiographic magnification using the conventional radiographic technique, the distension caused by the osmotic and diuretic effect of excreted contrast media is unlikely to reach a maximal diameter of 8 mm, which is almost 300% more than the CT measurement. The likely explanation for the finding of reduced maximal ureteric diameter in this study is that current IVUs are performed with non-ionic contrast media, which in theory exert less of an osmotic effect onto the urinary collecting system, thus producing less diuresis and distension of the ureters, in comparison with high osmolar contrast media used in studies in the 1970s. It is a well-recognized fact that pregnancy is associated with upper urinary tract dilatation due to both physiologic processes and compression of the urinary system by the gravid uterus (2,3,7). The right-side urinary tract is involved in 86% of cases, with the left side affected in 10% of cases (7). Some authors also observed that such dilatation is transient while others argue that dilatation persists long after the post-partum period, analogous to the physiological changes that occur in the breast and the uterus (7). If this proves to be true, it may pose diagnostic difficulties – for example, such ureteric dilatation in post-partum females during IVU studies may mimic obstructive and other non-obstructive causes of ureteric dilatation. The mean of the right abdominal ureteric diameter was 4.05 mm, and the left was 3.90 mm. The mean of the pelvic ureteric diameter was 4.21 mm on the right and 4.18 mm on the left. Although right abdominal and pelvic ureters appeared to be larger than the left, the difference was not statistically significant. We therefore conclude that the data from female subjects in this study showed no significant differences between the right and left ureters. In other words, dilatation of the urinary collecting system during pregnancy is transient and does not persist beyond the post-partum period. In future IVU studies in post-partum women, such findings for ureteric dilatation must be viewed with a consideration for the obstructive and non-obstructive causes of abnormal dilatation. We further tested to see if there was a significant difference between the mean ureteric diameters of male and female subjects to validate the fact that each ureter unit could be individually sampled for calculation of an overall mean and SD for the abdominal and pelvic ureteric diameters. The additional clinical implication of the above findings is that the fact that there is no significant difference between the right and left ureteric diameters in both male and female subjects, emphasizes the fact that symmetry in the ureteric diameter of both adult males and females is an expected normal finding in IVU research, and deviation from such findings should be considered abnormal. Limitations of study This study had certain limitations. It is a retrospective study of already-taken record images. Additional information could not be retrieved from the subjects, such as the weight and height of each patient. The sample was a group of patients who underwent IVU for routine indications at HUKM. Many of these subjects were referral cases from the satellite clinics around HUKM for which, in some of them, the IVU film was not returned to HUKM for record purposes. Many subjects also had incomplete sets of IVU films, with one or more films missing from their record. In those with complete sets, there are some with inadequate visualization of the entire ureter or poor quality of the opacification of ureter. Due to these limitations, and compounded by our strict exclusion criteria, many potential candidates were excluded, thus reducing the sample size. Within the limits of this clinical study, the IVUs of the examined subjects were reported to be normal. This study examined ureters in which there were no secondary signs of obstructive or non-obstructive dilatation of any part of the urinary collecting system, including the ureters. However, it must be remembered that all the patients were investigated for possible illness in their urinary collecting systems. All IVU examinations were done without fluid restriction. However, the actual fluid intake may vary amongst patients. Ureteric distension may thus vary depending on the hydrational statuses of patients. This is a limitation in IVU examinations in all previous studies, as fluid intake is difficult to quantify given the diversity of body mass/types of different patients. As different patients have different adipose tissue thicknesses, the magnification factor may vary between patients—a fact which was not corrected in this study. However this limitation is not of significant concern, as the aim of this study is not to examine the anatomical diameter of the ureter, as can be achieved by ultrasound or computed tomography examination, but rather to observe the range of projected diameters on radiographs in the sample population. Conclusion In conclusion, the mean abdominal ureter diameter was 4.19 mm with an SD of 1.27 mm, and the mean pelvic ureteric diameter was 4.45 mm, with an SD of 1.37 mm. Upper limits for the abdominal and pelvic ureteric diameters (based on confidence interval of 95%) are 4.37mm and 4.64mm, respectively. This study also finds no correlation between age and ureteric diameter. There is no statistically significant difference between the right and left ureters, particularly in females. Therefore, in a normal, non-pregnant female and in male subjects, symmetry of ureter is expected. Acknowledgements I wish to thank the following for their help in the preparation of this project report: Dr. Hamzaini Abdul Hamid, senior radiologist and lecturer, Radiology Department, HUKM for his invaluable guidance and supervision in the course of this project. Prof. Dr. Zulfiqar Mohd Anuar for generously giving her input and corrections and sharing her knowledge and opinions. Prof. Madya Zahiah Mohammad, Head of Radiology Department, HUKM for her consent to allow this study. Dr. Loi Hoi Yin, fellow radiologist and lecturer, radiology department, HUKM for his support and invaluable advice. Prof. Dr. Syed Zulkifli Syed Zakaria Al-Juffry, senior consultant and research fellow, UKM Medical Molecular Biology Institute, HUKM for his expert opinion on data interpretation and statistical analysis. I would also like to convey my heartfelt gratitude to the lecturers, colleagues, and staff of the radiology department, who have contributed in one way or another, to the completion of this project. Authors’ contributions Conception and design, provision of study materials or patients, data collection, analysis, and interpretation, statistical expertise, drafting of the article, final approval of article: WSL Administrative, technical or logistic support; critical revision of the article: HAH References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10014t5.jpg] [mj10014t4.jpg] [mj10014t1.jpg] [mj10014f2.jpg] [mj10014t2.jpg] [mj10014f1.jpg] [mj10014t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}