 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 17, No. 2, 2010, pp. 10-17 Original Article Preventing HIV transmission in Nigeria: role of the dentists Clement Chinedu AZODO1, Adebola Oluyemisi EHIZELE1, Agnes UMOH2, Gabriel OGBEBOR3 1Department of Periodontics, University of Benin Teaching Hospital,
Benin City, Nigeria Correspondence: Dr Azodo Clement, BDS, MSc (University of Benin), Department of Periodontics, University of Benin Teaching Hospital, P.M.B 1111, Benin City, Edo State, Nigeria, Tel: +234-8034051699 E-mail: clementazodo@yahoo.com Submitted: 13 May 2009 Code Number: mj10015 Abstract Background: As healthcare providers, dentists are in a unique position to
foster behavioural changes that are needed to stem the spread of HIV infection.
This study was conducted to assess the role of dentists in the prevention of
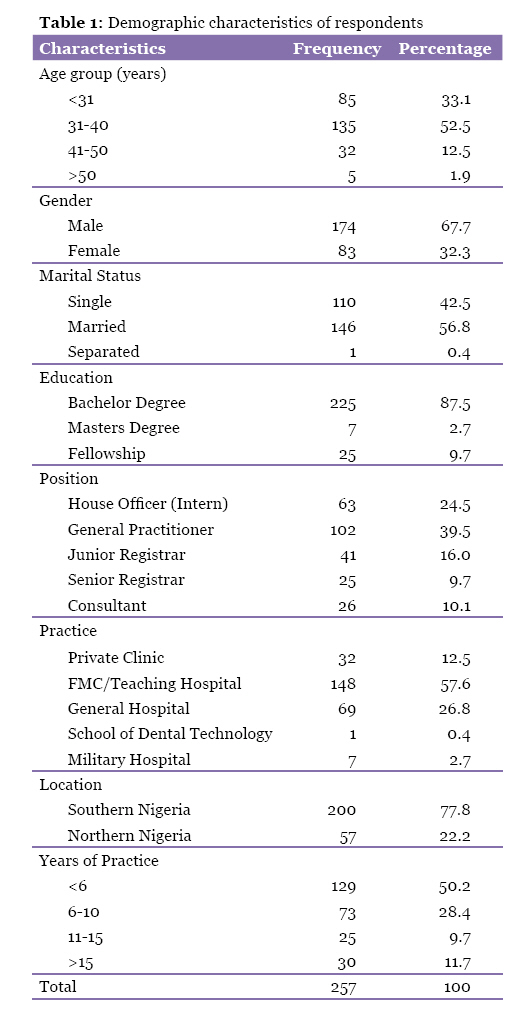
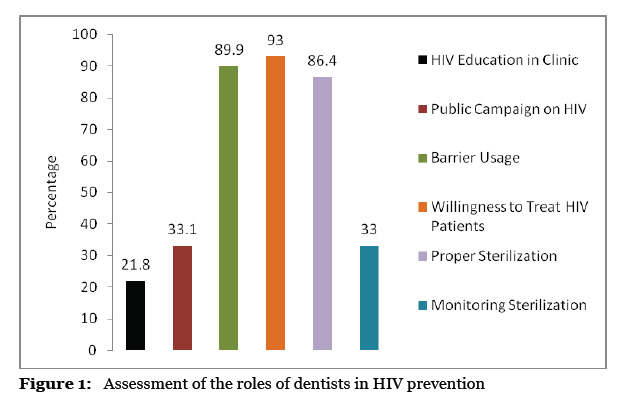
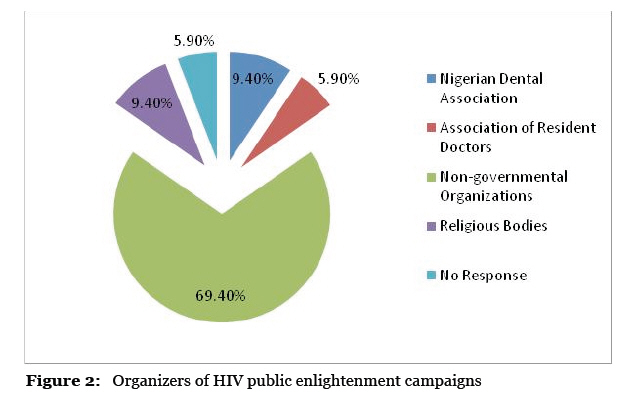
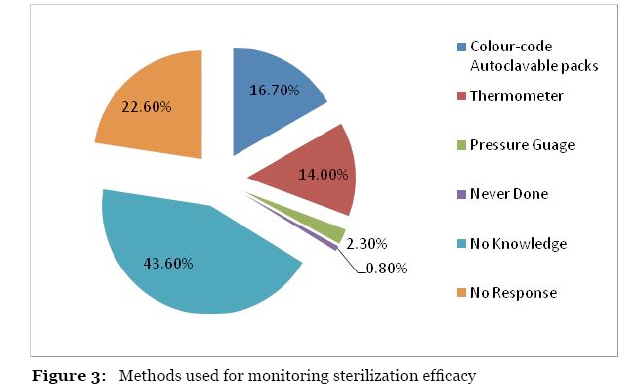
HIV transmission in Nigeria. Keywords: HIV, infection transmission, Nigeria, dentists practice patterns, prevention and control, dental sciences Introduction HIV/AIDS is the leading infectious cause of adult mortality in Africa (1). Africa is the most affected continent, accounting for 70% of the global HIV/AIDS pandemic (2). The magnitude of HIV/AIDS infection in Nigeria presents an alarming trend. Nigeria has the third highest number of people living with HIV/AIDS in the world after South Africa and India (3). Public perception of the HIV epidemic has culminated in heightened and persistent public anxiety. This anxiety is attributed to the high mortality rate of AIDS and the fact that there is, to date, no proven vaccine or cure. If the epidemic continues at its current rate or worsens, its effects could spread across the whole continent. Prevention is therefore a critical issue in Nigeria. HIV prevention must be a multidisciplinary approach involving physicians, dentists, pharmacists, nurses, health educators, therapists and other health care providers. National data on the utilisation of oral health services per annum in Nigeria were not available, but more than half of the population in America visit dentists yearly (4). A great percentage of HIV-infected patients and those at risk are in the age range between 15 to 49 years. The majority of patients visiting dental clinics are in a similar age range (5). Approximately 18–20% of young men and women in Nigeria between the ages of 15 and 24 correctly identified ways to prevent HIV transmission (6). Those infected with HIV may relapse to risky behaviour when preventive counselling is less than optimal. Provider-delivered risk reduction counselling has been shown to reduce risky behaviour by people living with HIV/AIDS in other settings. Dental health workers are well placed to provide information about HIV. The public is willing to discuss AIDS with dentists and is favourably disposed to the information dentists’ supply. Patients see dental practices as a place where they can discuss and receive valuable and trusted information about HIV. Studies consistently demonstrate that patients view their dentist as a trusted and authoritative source of health information (7). Studies in other disease prevention areas have shown that brief intervention delivered by dentists can translate into behavioural change (8). Dental patients are particularly receptive to health messages at their periodic check-up (9). For these reasons, dental clinics provide an excellent venue for HIV prevention and intervention services. There is a high possibility that dentists treat HIV-infected patients unknowingly because most patients are probably unaware of their HIV status. The undiagnosed, untreated patient may unknowingly be a hazard to dentists, dental staff and other patients, especially because everyday dental practices involve invasive procedures and instrument reuse. There is documented evidence of HIV transmission in dental operations (10). Only effective infection control measures in a clinical setting can prevent the spread of HIV and other highly infectious diseases. Failure to adequately clean, disinfect and/or sterilize dental instruments contaminated with HIV from previous patients will endanger subsequent patients. If adequate precaution is not taken to prevent blood and body fluid contamination, the risk of HIV transmission increases tremendously. Studies have documented that 70–90% of HIV-positive individuals display oral manifestations of HIV, (11) but Nigerian-based studies reported a 48.8–53% prevalence of oral lesions in HIV-infected adults (12,13). Many different oral lesions may occur at different stages of the infection. Poor oral health could complicate the management of the medical conditions of HIV-infected patients and may create or exacerbate nutritional problems. Oral prophylaxis improves the oral health and quality of life of individuals with HIV/AIDS infection. There is therefore a need for HIV-infected patients to receive dental care at different times during the course of the disease. The AIDS INSTITUTE stated that the treatment of oral manifestations of HIV infection could improve a patient’s attitude, quality of life and general well-being (14). Dentists have an ethical, moral and professional obligation to protect themselves, co-workers, patients and society at large from any avoidable harm, including exposure to HIV infection. Dental services may therefore have a role in the primary prevention of HIV by providing information about HIV and promoting health through early diagnosis and treatment of oral manifestations of HIV/AIDS. Several researchers have documented the multiple roles of dentists in the HIV/AIDS pandemic (15–19), which include the following: the provision of routine dental care to HIV-infected patients; preventing the spread of HIV through proper infection-control practices; providing education to the community and clinic; oral lesion screening, diagnosis, treatment and recognition of its significance; educating other health care workers; acting as a resource to HIV-infected health care workers; collaborating with other health care workers and social support systems in delivering psychological counselling and drug rehabilitation; conducting research concerning HIV/AIDS; and finally, screening for HIV infection using a rapid oral fluid HIV antibody test. Oral health priority areas of the World Health Organisation (WHO) focus on the dissemination of information on HIV/AIDS and its prevention through every possible means of communication. The WHO advises the involvement of oral health personnel in the documentation of HIV/AIDS to ensure appropriate medical evaluations in prevention and treatment (20). The WHO established a task force to focus on key regions including the African Union and Southeast Asia. Nigeria is Africa’s most populous nation and ranks tenth in the world with a population of 140 million (21). The objective of the survey was to assess the role of dentists in the prevention of HIV transmission in Nigeria. Materials and Methods This study was designed as a cross-sectional descriptive survey. The survey population was 300 dentists practicing in private and government-owned dental centres in Nigeria. The sample population was divided into north and south groups. A multi-stage proportionate sampling technique was used because there are more dentists practicing in the southern part of the country. Data were collected using a pre-tested, self-administered questionnaire that contained open and closed-ended questions. The questions focused on dentist demographic data, dentist-to-patient education on HIV issues, participation in public enlightenment campaigns on HIV, attitudes to treating HIV-infected patients, infection barrier practices and sterilization. Questionnaires were hand-delivered by the authors to dentists at their dental centres, while some were delivered by mail. Informed consent was obtained from the participants. There was an introductory note in the survey that explained that the co-operation of respondents would be highly appreciated, and their responses would be treated with strict and the utmost confidentiality. The survey was anonymous. The duration of the study was seven months from June 2006 to January 2007. Data were analysed with SPSS version 13.0, and graphs were plotted with Microsoft Excel. Results Out of 300 questionnaires, 257 were returned completed, resulting in a response rate of 86%. Demographic characteristics Table 1 shows the demographic characteristics of respondents. HIV education Less than a quarter of respondents (21.8%) routinely educate patients on HIV in the clinic, and only one third of dentists (33.1%) were engaged in any HIV public enlightenment in the last 12 months (Figure 1). They were mostly males (24.7%) and younger dentists with 1–5 years’ experience (30.0%). HIV public enlightenment was organised by non-governmental organisations in almost 70% of cases (Figure 2). Willingness to treat HIV-infected patients The majority (93%) of respondents reported a willingness to treat HIV-infected patients observing universal precautions (Figure 1). Infection barrier usage Good infection barrier practice was adopted by 89.9% of the respondents (Figure 1). However, the most commonly used gloves during patient examination were non-sterile latex gloves (58.4%), while the least commonly used were sterile latex gloves (22.5%). Disposable cartridges for local anaesthetic agents were not reused by 93.4% of the dentists, and 95.7% of dentists did not reuse disposable dental needles. Sterilization Appropriate sterilization techniques were used by 86.4% of respondents (Figure 1). Dry heat accounted for 13.2%, and autoclaving was the most popular method (73.2%). Inappropriate methods were reported and included boiling water (5.1%), cleaning with bleach alone (3.1%) and cleaning with soap and water alone (0.4%). Those respondents that were unaware of the sterilization method used in their dental centre made up 1.6% of the total respondents, and only 2.7% gave no response. Less than half (33%) knew how to ascertain whether sterilization was effective, while 43.6% reported no knowledge. The efficacy of sterilization was monitored with the use of colour-coded autoclaving packs (16.7%), thermometers (14.0%) and pressure gauges (2.3%) (Figure 3). Discussion The role of dentists in the prevention of HIV transmission is largely ignored in the literature. To our knowledge, this report is the first comprehensive survey on the preventive roles of dentist in the HIV/AIDS pandemic. The response rate in this study was higher than other dentist-based studies reported in Nigeria (22) and other African countries (23). The high response is consistent with the impact that HIV has had on dental practices in Nigeria. The non-response rate in some questions was similar to that documented in a questionnaire-based survey of American dentists (24). The distribution of dentists in Nigeria may be a result of the location of dental schools. Only 12.4% of the dentists in this study had additional qualifications other than the basic dental degree. This result may be attributed to limited vacancies and the unattractive nature of dental postgraduate training prior to the new millennium. There are a limited number of counsellors and health educators in Nigeria. Nigerian dentists’ involvement in public education is very low (33.1%), and only 21.8% routinely educate patients on HIV in their clinics, as shown in this study. This level of involvement is inadequate, especially because it has been documented that this type of information giving can be effective (25), and dentists have a great deal of contact with potentially high-risk patients (26). The findings from this study are surprising because dental students have agreed to the adoption of public education as a preventive measure for HIV transmission (27). The currently low participation of dentists in public education may be a result of the poor coordination by their professional associations and governmental agencies. Most dentists who were involved in public education did so under the auspices of non-governmental organisations (65.9%). A positive attitude towards HIV patients and preparedness to advise these patients are essential elements for dentists to play a successful role in the management of HIV/AIDS. Providers’ attitudes about HIV/AIDS are an important factor in the delivery of quality care to people with HIV/AIDS. The willingness to treat patients while observing universal precautions was quite high (93%). This willingness is about 30% higher than reported by Uti et al. (28) and also higher than reported in a South African study (29), in which only 42% of dentists were willing to treat HIV-infected patients. In contrast, a Kenyan study (23) reported that 87% were willing to treat this group. Improved knowledge of HIV/AIDS in dental health workers over the last few decades may be the reason for the increased willingness to provide care and the more positive attitude towards HIV-infected individuals. Interestingly, 100% of the respondents that refuse to treat HIV-infected patients were female dentists. This finding is consistent with previously documented gender differences in caring for infected individuals (30). Interestingly, 100% of the respondents that will treat patients without observing universal precautions are male dentists. This finding may be because males are more likely to take risks in general than females. The proper use of infection barriers, like hand gloves (89.9%), reported by respondents in this study was higher than reported in 2003 among public hospital dentists in Lagos, Nigeria (70.6%) (22). The accepted universal practice is to use a fresh cartridge containing the local anaesthetic agent and a new disposable needle for each patient. Most dentists in this survey do not reuse needle and cartridges, but a significant few (16.7%) still reuse needles (chi-square test, P=0.002). Approximately 6% of private dental practitioners reuse anaesthetic cartridges, and 1.5% reused needles (31). Sterilization is the destruction of all forms of micro-organisms (vegetative and spores) for a given object, and it is the best method to prevent cross infection from patient to patient in oral health care. All critical and semi-critical dental operative instruments that are heat stable should be cleaned, debrided and then sterilized in a steam autoclave or dry-heat hot air oven at a specified temperature and duration. Autoclaving is the most popular sterilization method among respondents (73.2%), which is consistent with previously reported findings (22,23,29). Boiling water is presently seen as an inappropriate method of sterilization in dentistry because it kills vegetative bacteria within 2 or 3 minutes, but bacteria spores and viruses may take many hours. Despite the fact that the use of boiling water is being discouraged, 5.1% of the respondents reported boiling water as their mode of sterilization. Ideally, tests should be conducted routinely to check that sterilization is adequate. These tests may be performed with chemical indicators such as Browne’s autoclave tape, a standard test pack containing a thermocouple or by using standardised spore papers. Only about a third of dentists (33%) who use appropriate sterilization methods can ascertain whether their sterilization is optimal. Poor monitoring of sterilization was also reported in a study on university dental clinics in Nigeria (32), where it was discovered that sterilization ovens did not have thermometers and biological monitoring (spore testing) was not conducted. Conclusion Educating patients in Nigeria on HIV prevention by dentists both inside and outside clinics is at a very low level, while infection control based on barrier usage, appropriate sterilization methods and the willingness to treat HIV patients are relatively high. Inadequate monitoring of sterilization was evident, and a few dentists still use poor practices that may put themselves and their patients at risk. The overall assessment revealed that efforts by Nigerian dentists are still less than optimal. Recommendations The role of dentists in preventing HIV should be adopted as a topic in continuing education courses. Sensitisation and motivation of Nigerian dentists through seminars, workshops and lectures is advocated. The National Dental Association should actively disseminate information to educate members on their roles in the prevention of HIV and other blood-borne infections. The few practitioners that constitute the greatest risk should be targeted, and legislation should be enacted to prevent bad practice. Additionally, existing laws should be properly enforced. Acknowledgements The authors wish to thank Prof. M.A Ojo, Head of the Department of Oral Medicine and Pathology, Dr. N.O. Obuekwe, Acting Dean of the School of Dentistry and Dr. V. A. Omuemu, Public Health Physician in the Department of Preventive Medicine, University of Benin, Benin City, Nigeria, for reviewing this manuscript before it was presented at the 4th International AIDS Society Conference on Pathogenesis, Treatment and Prevention in Sydney, Australia. Authors’ contributions All authors contributed equally to the conception and design of the study, data collection, analysis, and interpretation, as well as drafting and critical revision of the article. References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10015f3.jpg] [mj10015f1.jpg] [mj10015f2.jpg] [mj10015t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}