 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 17, No. 2, 2010, pp. 18-23 Original Article The Prevalence of Urinary Incontinence among the Elderly in a Rural Community in Selangor Sherina MOHD SIDIK Department of Community Health, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, 43400 Serdang, Selangor, Malaysia. Correspondence: Dr Sherina Mohd. Sidik, MBBS (Malaya), MMed (Family Medicine), Unit of Family Medicine, Department of Community Health, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, 43400 Serdang, Selangor, Malaysia. Tel: +603-8946 8449 Fax: +603-8945 0151 E-mail: sherina@putra.upm.edu.my Submitted: 7 Sep 2009 Code Number: mj10016 Abstract Background: Urinary incontinence is a common but poorly understood problem
in the elderly population. The aim of this study was to determine the prevalence
of urinary incontinence and its associated factors among the elderly in a community
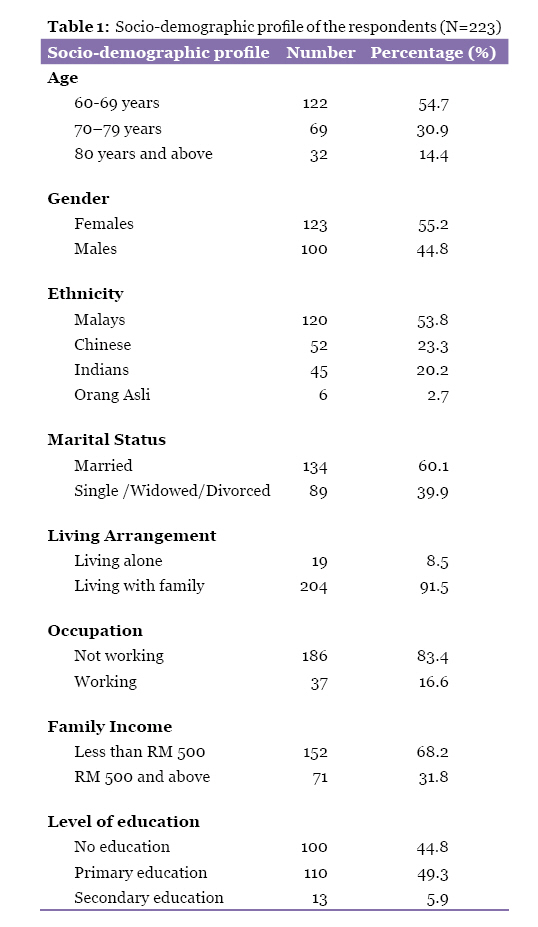
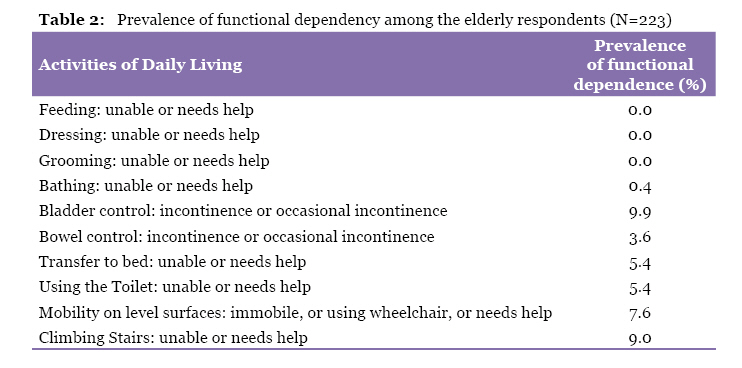
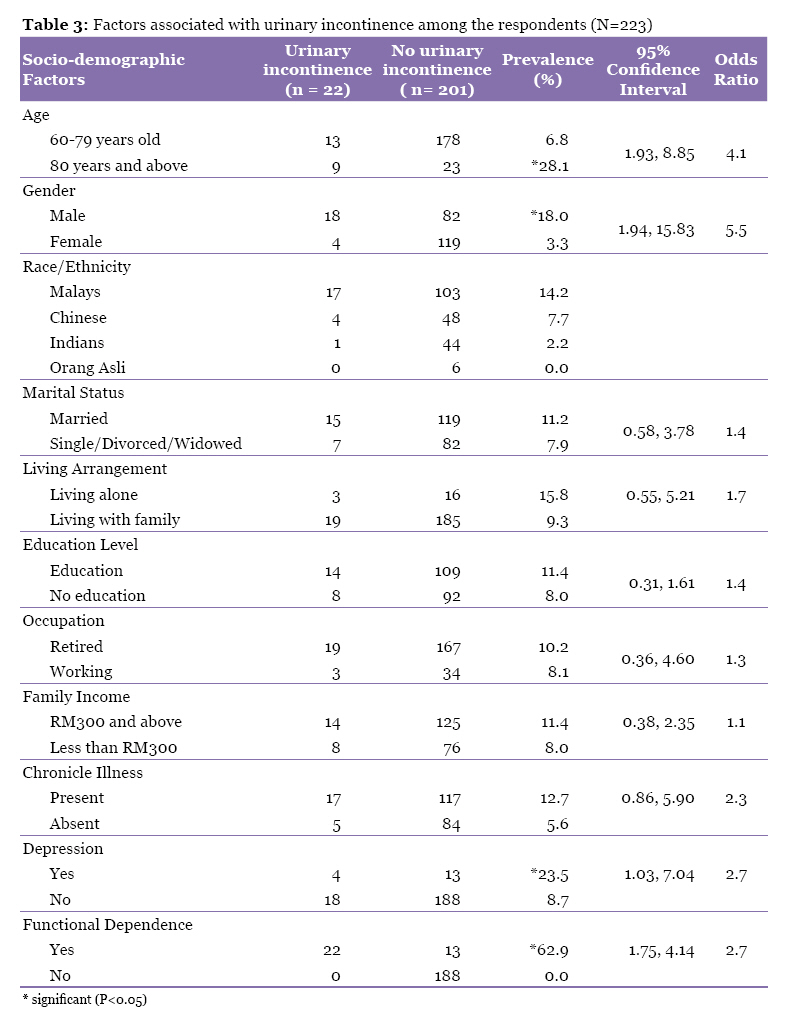
setting. Keywords: associated-factors, community, elderly, prevalence, urinary-incontinence, medical sciences Introduction Urinary incontinence is a common problem among the elderly (1). Many studies have recorded the prevalence of urinary incontinence in old people living in the community as well as those living in institutions. The prevalence rate in the community has ranged from 7% to 42%, (2–8) and the rate has typically been higher in institutions (9). The prevalence of incontinence may be significantly underestimated. The elderly may assume that urinary incontinence is a normal consequence of aging. Some elderly may be embarrassed by their incontinence or fear invasive testing, and thus, avoid evaluation. In primary health care clinics and hospitals, medical and health personnel rarely ask patients about urinary incontinence. Furthermore, patients seldom initiate discussions about incontinence (10). Urinary incontinence commonly results in medical, social, and economic consequences. Incontinence is a common reason for the institutionalisation of the elderly. The care of incontinent nursing home residents is significantly more expensive than continent residents, and requires more nursing time. Urinary incontinence can result in skin irritation and contribute to skin breakdown or pressure sores. The social consequences include guilt and isolation, with some elderly afraid to leave their homes (10). Though the younger age group comprises a large part of the population, the proportion of the older age group is substantially increasing (11). The health problems associated with the elderly in this country are a major cause of concern for health care providers. Urinary incontinence is a health condition that affects the elderly. We hypothesise that the prevalence of urinary incontinence among the elderly is not uncommon. The aim of this study was to determine the prevalence of urinary incontinence among the elderly in a rural community in Selangor. In addition, factors related to urinary incontinence were also studied. Materials and Methods A cross-sectional study was conducted in Sepang District, Selangor between 17th June and 20th August 2002. Stratified cluster sampling was used in this study; living areas in Mukim Sepang were stratified into traditional villages, small towns and one “Orang Asli” village. Three out of 6 traditional villages, 1 out of 2 small towns and 1 “Orang Asli” village were randomly selected. The study population consisted of elderly residents aged 60 years old and above who were Malaysian citizens. Exclusion criteria included elderly who were not Malaysians and those with significant communication problems such as deafness and stroke. The respondents who fulfilled the selection criteria were personally interviewed using a structured questionnaire. The questionnaire consisted of three parts. Part 1 consisted of questions on age, gender, ethnicity, marital status, living arrangement, educational level, occupation, family income and history of chronic illness. Part 2 consisted of the Malay version of the Barthel’s Index (BI). Part 3 consisted of the Malay version of the Geriatric Depression Scale. Data were collected via face-to-face interview by trained personnel. Interviews were approximately 20 to 30 minutes in length. The translated Malay version of the BI was used to identify the presence of urinary incontinence. This questionnaire was modified after the original BI (12) and was pre-tested in a locality not included in the study area. The internal reliability of the translated version was assessed using Cronbach’s alpha coefficient and was found to be satisfactory (coefficient alpha of 0.71). The questionnaire consists of 10 questions measuring basic Activities of Daily Living (ADL), including urinary incontinence. Functional dependence in basic ADL implied that the respondent required assistance in one or more of these tasks (8). Based on the BI, the presence of urinary incontinence was determined by asking the respondents whether they had problems with their bladder control. Answers of “yes” or “occasional” were grouped as having urinary incontinence. The translated Malay version of the Geriatric Depression Scale (GDS), which consists of 30 questions, was used to screen for depression. The total scores range from 0 to 30. Based on the GDS guidelines, a cut-off score of more than 10 was used to identify depression (13). The internal reliability of this translated version was also found to be satisfactory (coefficient alpha of 0.69). Written consent was obtained from each respondent. Ethics approval was obtained from the Faculty of Medicine and Health Sciences Ethics Committee of University Putra Malaysia. Data was analysed using SPSS version 10.0. The statistical significance was set at P < 0.05. Chi-square test with a confidence interval of 95% and odds ratio (OR) were used to determine the association between urinary incontinence and age, gender, ethnicity, marital status, living arrangement, occupation, family income, functional dependence, depression, presence of chronic illness and types of chronic illness. Results Of the 263 elderly residents, 223 agreed to participate, resulting in a response rate of 84.8%. Socio-demographic profile The age of the respondents ranged from 60–99 years, with a mean of 69.7 ± 6.8 years and a median of 68 years. The majority of the respondents were females (55.2%), Malays (53.8%), married (60.1%), living with family (91.5%), had formal education (55.2%), were not working (83.4%), and had a monthly family income of more than RM 300 or USD 91.70 (62.3%) (Table 1). Barthel’s Index The most common type of functional dependence was urinary incontinence (n = 22 or 9.9%) (Table 2). This was followed by problems with steps (n = 20), poor mobility (n = 17), problems with transferring (from bed to chair or chair to chair/commode) (n = 12), using the toilet (n = 12), bowel incontinence (n = 8), and bathing (n = 1). None of the respondents were dependent in feeding, dressing or grooming (n = 0). Urinary incontinence Urinary incontinence was found to be significantly associated with age, gender, functional dependence, depression and diabetes mellitus (P < 0.05) (Table 3). Discussion The prevalence of urinary incontinence among the elderly in this study was 9.9%. This is comparable to the studies conducted by Poi, which found the prevalence in Malaysia to be 9.1%, and by Chia at 9.0% (10,14). However, among the elderly in Singapore, Chan et al. found that the prevalence of urinary incontinence was 14.5% (15). Mayo estimated that at least 15% of community-dwelling elderly individuals and 50% of institutionalised elderly persons have significant urinary incontinence (16). All of the Malaysian studies reported a lower prevalence of urinary incontinence compared to other countries. This may be an underestimate of the actual situation as elderly in this country may not be as forthcoming in revealing their health problem (13,15). Age was found to be associated with urinary incontinence. The odds of the elderly aged 80 years and above having urinary incontinence compared to those aged 60 to 79 years were 4:1. In this study, urinary incontinence may be related with difficulty in mobility and transferring. Many studies have shown very high prevalence rates of urinary incontinence in those aged 85 and older (2,4,5,7,17). Normal aging causes changes in urinary anatomy and patho-physiology, which allows incontinence to occur more easily. Aging results in the reduced size of the urinary bladder, producing a decreased bladder volume and a need for more frequent bladder emptying (urinary frequency). Many elderly individuals experience early detrusor contractions, even at low bladder volumes. This results in a sense of urgency to empty the bladder. Elderly individuals are, in general, less able to suppress early detrusor contractions (15). This study found that males had a higher risk of urinary incontinence compared to females (OR 5.5:1). This contrasted with other studies that found that urinary incontinence was more common among females as compared to males (1,2,4,5,7). Urinary incontinence was also found to be significantly associated with functional dependence. Nearly two-thirds of the elderly with functional dependence had urinary incontinence. Among the respondents without functional dependence, none complained of urinary incontinence. Studies have documented that as the degree of functional dependence increases, the prevalence of incontinence increases as well (15). Depression was also found to be associated with increased risk of urinary incontinence (OR = 2.7). Research has shown that urinary incontinence can adversely affect quality of life, leading to depression, negative affect, low life satisfaction, and restriction of activities (1). The elderly tend to be embarrassed of their problem and may even experience a sense of guilt. They are reluctant to go out and socialise because of their problem. This eventually leads to self-imposed social isolation (15). There was no association between chronic diseases and urinary incontinence. However, diabetes was found to be associated with a higher risk of urinary incontinence (P < 0.05). Studies have shown that in addition to changes of normal aging, diseases such as dementia and cognitive impairment, which are commonly experienced by the elderly, may contribute to the problem of urinary incontinence. Urinary tract infections, diabetes mellitus, benign prostatic hyperplasia, and immobility are also typical examples of conditions that may impact urinary incontinence (10,15). Conclusion The prevalence of urinary incontinence in this study is most likely underestimated due to the study’s limitation in determining the presence of urinary incontinence by a self-report method based on the BI. It is possible that mobility problems contributed to the presence of urinary incontinence among the respondents in this study. Another problem in the elderly age group is cognitive impairment, which also contributes to urinary incontinence. However, this risk factor was not examined in this study. Despite the limitations of this study, we acknowledge the fact that urinary incontinence is a common and poorly understood problem in our community. Based on the self-reported evidence in this study, urinary incontinence occurred in approximately 1 in 10 elderly respondents. A larger and more in-depth study might reveal a much higher prevalence. Detection of this problem is essential for preventing complications and improving the quality of life of the elderly. Acknowledgement We would like to express our gratitude to the Dean of the Faculty of Medicine and Health Sciences, Universiti Putra Malaysia for his support and permission to publish. References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10016t2.jpg] [mj10016t1.jpg] [mj10016t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}