 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 17, No. 2, 2010, pp. 29-39 Special Communication Computed Tomography (CT) Imaging of Injuries from Blunt Abdominal Trauma: A Pictorial Essay Radhiana HASSAN1,2, Azian ABD. AZIZ1 1Department of Radiology, International Islamic University Malaysia,
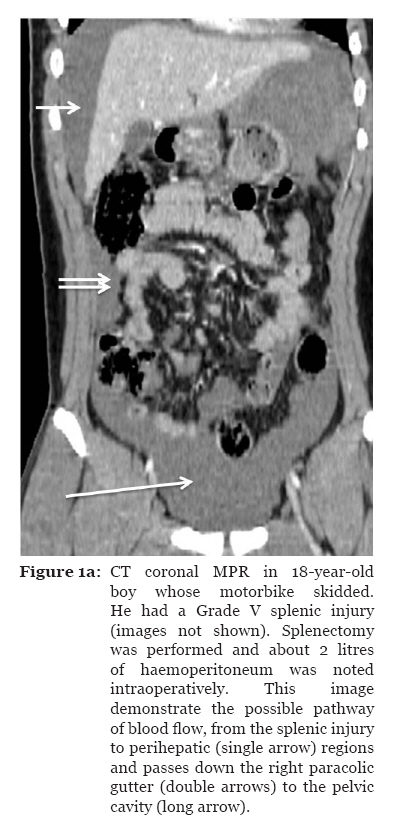
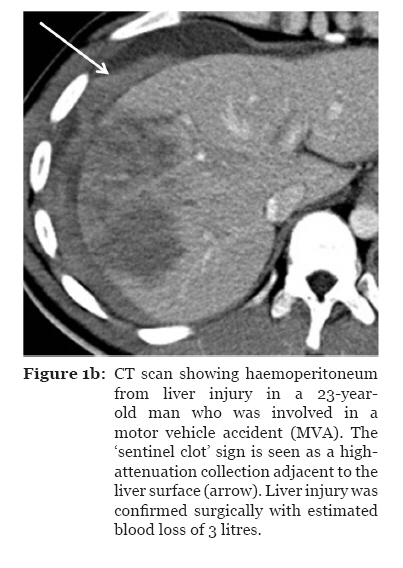
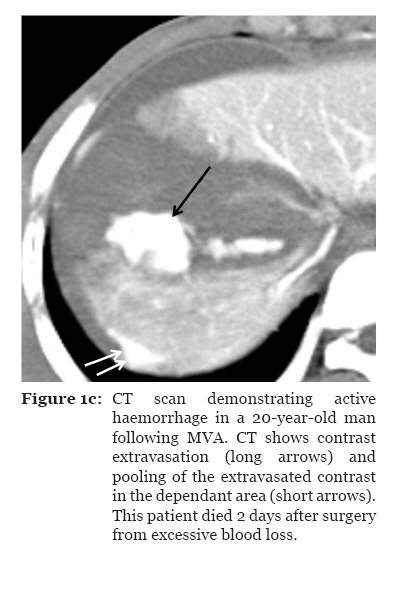
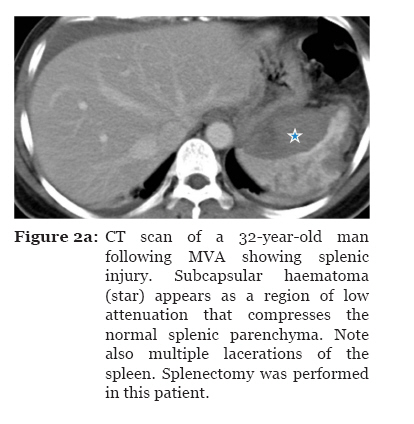
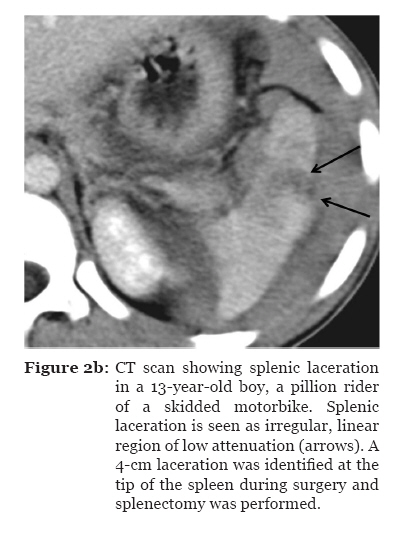
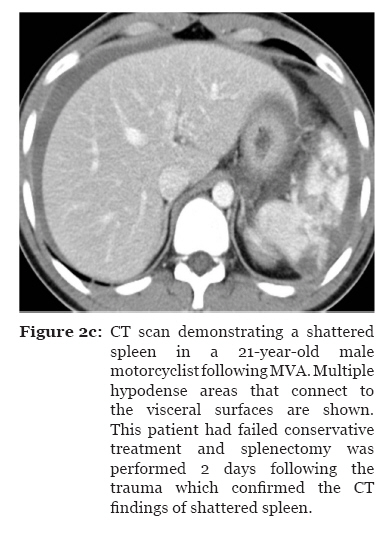
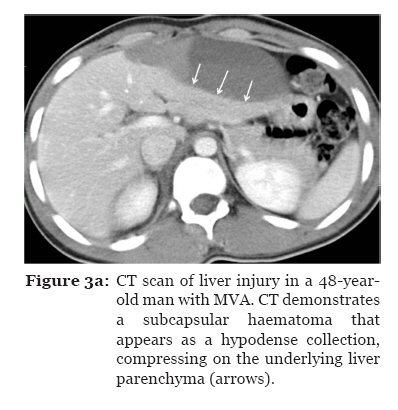
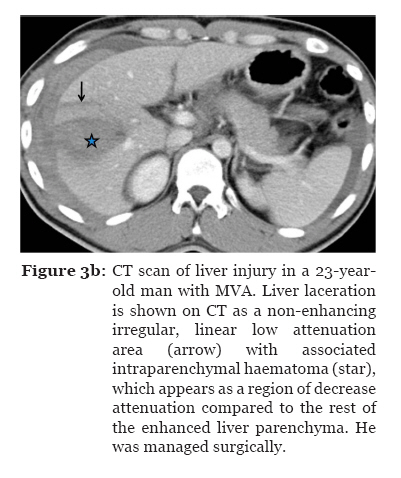
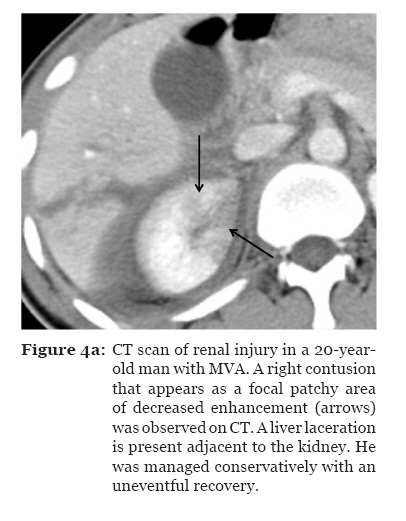
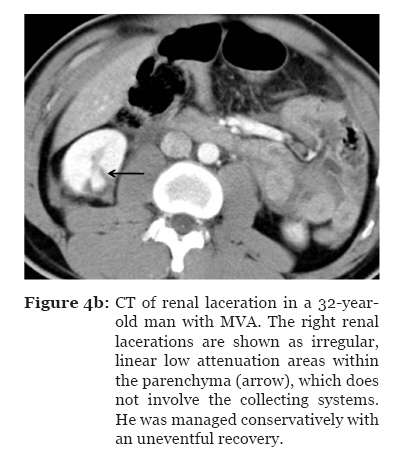
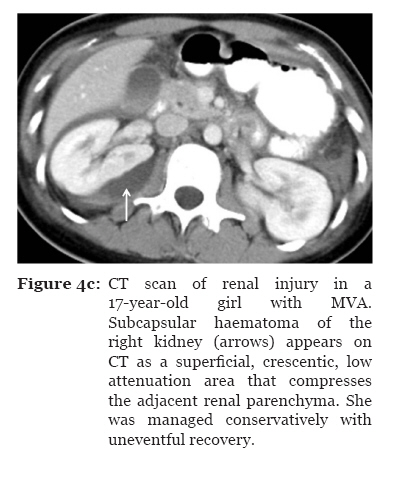
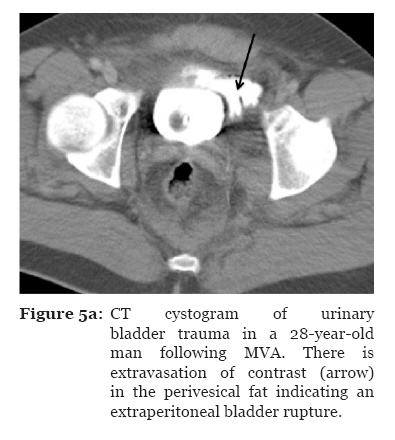
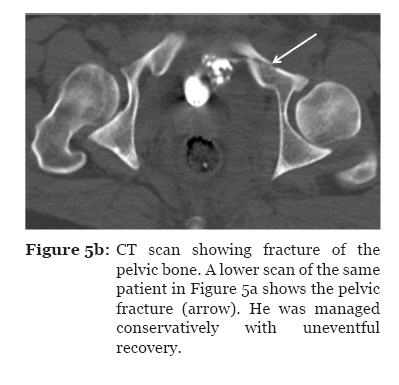
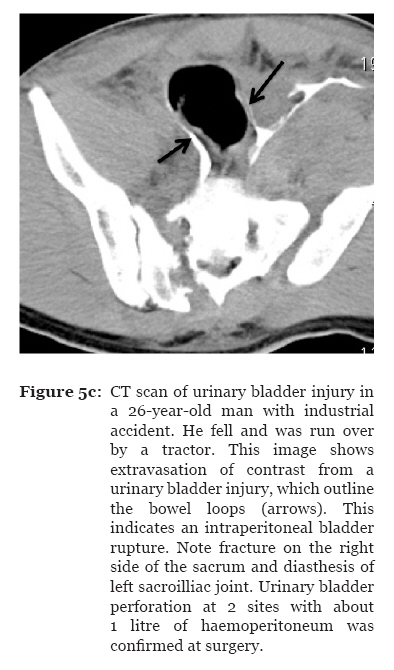
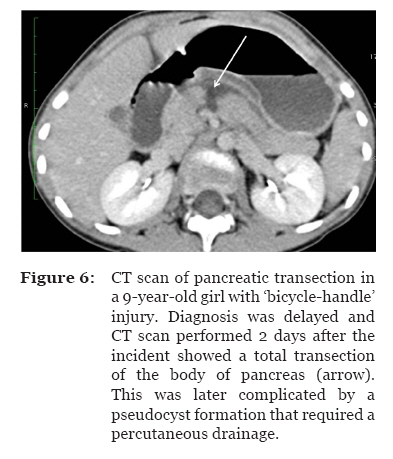
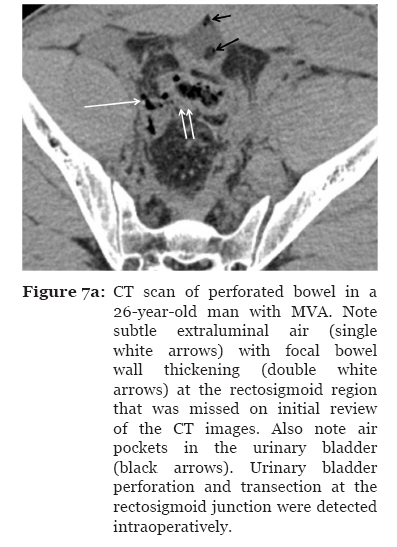
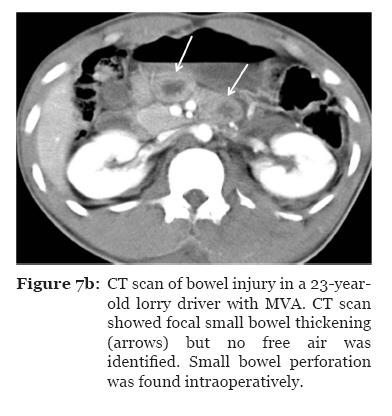
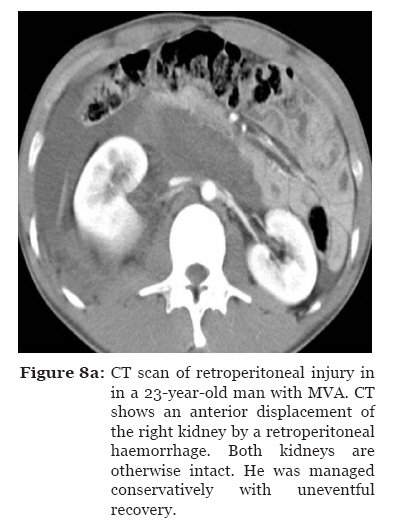
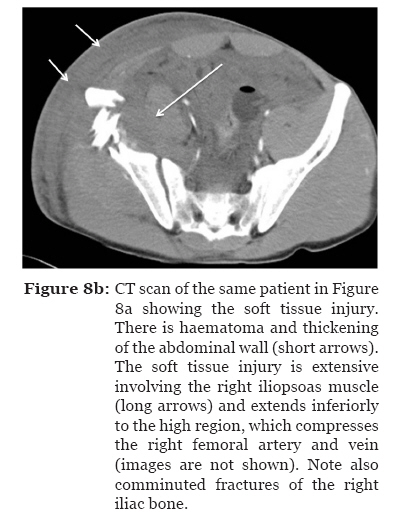
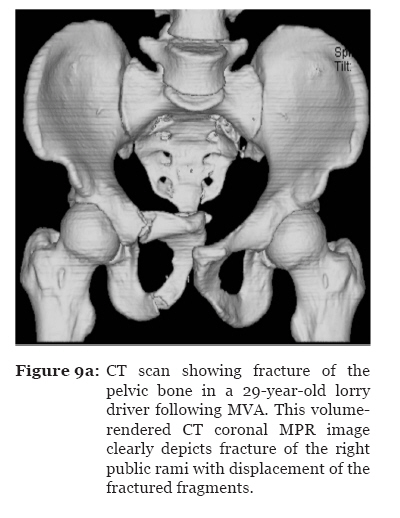
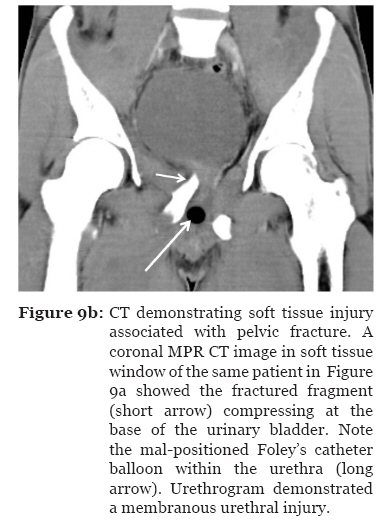
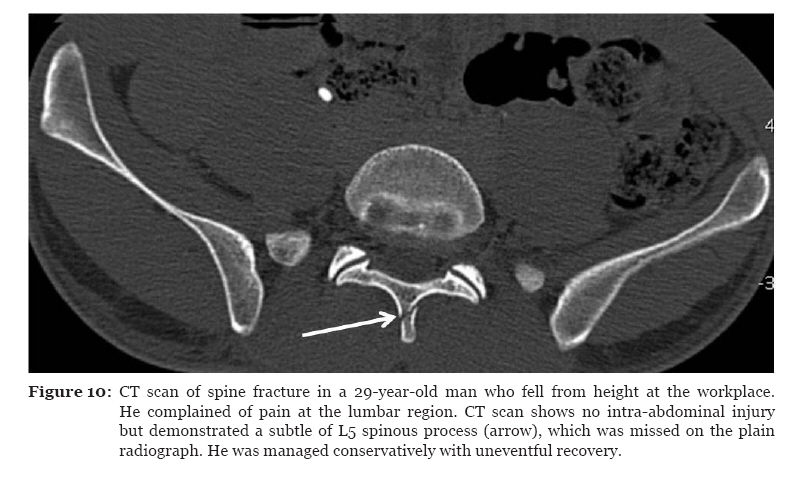
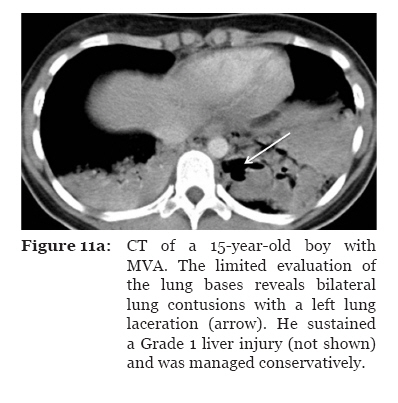
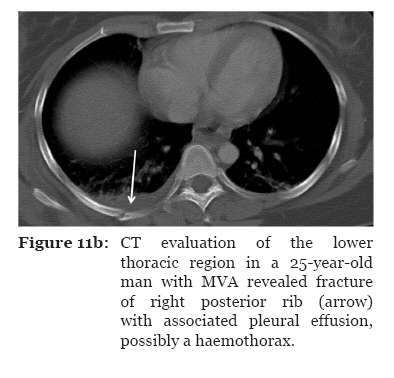
Bandar Indera Mahkota, Kuantan, 25200 Pahang, Malaysia Correspondence: Dr Radhiana Hassan, MD (USM), MMed (Rad) (USM), Department of Radiology, Kulliyyah of Medicine International Islamic University Malaysia (IIUM) Bandar Indera Mahkota, 25200 Kuantan, Pahang Darul Makmur, Malaysia, Tel: +609-557 2056 Fax: +609-514 9396 E-mail: radhianahassan@gmail.com Submitted: 27 Aug 2009 Code Number: mj10018 Abstract Blunt abdominal trauma can cause multiple internal injuries. However, these injuries are often difficult to accurately evaluate, particularly in the presence of more obvious external injuries. Computed tomography (CT) imaging is currently used to assess clinically stable patients with blunt abdominal trauma. CT can provide a rapid and accurate appraisal of the abdominal viscera, retroperitoneum and abdominal wall, as well as a limited assessment of the lower thoracic region and bony pelvis. This paper presents examples of various injuries in trauma patients depicted in abdominal CT images. We hope these images provide a resource for radiologists, surgeons and medical officers, as well as a learning tool for medical students. Keywords: blunt abdominal trauma, computed tomography, injuries, medical sciences Introduction The rapid identification of life-threatening injuries and prompt initiation of appropriate care may increase the chance of survival for patients with trauma. However, it is often difficult to accurately clinically evaluate blunt abdominal injuries, which may be masked by other more obvious external injuries. CT imaging is the diagnostic tool of choice for the evaluation of abdominal injury due to blunt trauma in haemodynamically-stable patients (1). CT scans can provide a rapid and accurate appraisal of the abdominal viscera, retroperitoneum and abdominal wall (2). In addition, an abdominal CT scan can assist in the evaluation of coexisting abdominal injuries such as thoracic injuries (3) and unsuspected pelvic and spinal fractures. The ability of CT to perform and produce fast-processing images, such as multiplanar reconstruction (MPR), is important for the accurate interpretation of abnormalities. A variety of comments, reports and studies on the accuracy and efficacy of CT in the evaluation of blunt abdominal trauma are available in the medical literature; this topic is highly debated and has generated much discussion (4–11). CT has been reported to be valuable for the diagnosis of solid organ injuries and for the detection of active bleeding. The accurate detection of bowel and mesenteric injuries has also improved with the development of thin-section multidetector CT (MDCT) (7). The use of CT to evaluate blunt trauma has influenced current trends in the management of solid organ injuries, prompting a greater focus on non-surgical management (12). Although the decision to surgically intervene is usually based on clinical criteria rather than findings from images (13), CT information often increases diagnostic confidence and decreases rates of unnecessary exploratory laparotomy (14). In 2008, 92 abdominal CT scans were performed to assess blunt abdominal trauma in a tertiary referral centre (Hospital Tengku Ampuan Afzan (HTAA) in Kuantan, Pahang). In all of these cases, CT scans were performed based on the clinical suspicion of intra-abdominal injury. CT films and each patient’s case notes were followed and retrospectively reviewed. Of these 92 scans, CT images showed injuries involving various organs in 72% of cases; the remaining images did not show any injuries. All of the scans were performed using a four- row multislice CT scanner (Somatom Siemens Volume Zoom, Siemens Medical Systems, Erlangen, Germany) with a slice width of 10 mm, a 2.5 mm collimation, a 0.75 s rotation time, a table feed of 15 mm and a 3 mm reconstruction interval. Pre- and post-contrast scans were routinely performed and patients received 2 mL/ kg of intravenous contrast medium (Iohexol, 300 mg/mL). Oral contrast was not routinely given. The CT scans were acquired during the portal venous phase approximately 80 seconds after the contrast injection. When necessary, sagittal and coronal images were acquired using the maximum intensity projection (MIP) and MPR techniques. Full thoracic CT scans were not routinely performed when lower thoracic injuries were observed on the abdominal CT. The various injuries seen on the CT images were grouped and examined based on the injury site and the organs involved. Haemoperitoneum and the detection of active haemorrhage CT has high sensitivity and specificity for the detection of blood in the peritoneal cavity (15). Haemoperitoneum starts near the site of injury and spreads along the expected anatomic pathways (16). When the patient is in a supine position, blood from the liver collects in Morison’s pouch and passes down the right paracolic gutter to the pelvis. From the spleen, blood passes via the phrenocolic ligament to the left paracolic gutter and the pelvis (Figure 1a). Blood from a splenic injury also goes to the right upper quadrant (16). Although peritoneal lavage is a sensitive indicator of intraperitoneal haemorrhage, it is unable to detect the source or origin of the bleeding (17). The ‘sentinel clot’ sign indicates adjacent, focal higher attenuation clotted blood as a marker for the organ that is the cause of haemorrhage (16) (Figure 1b). A large amount of blood may collect in the pelvis without much haemoperitoneum seen in the upper abdomen. Active haemorrhage can appear as a region of extravasated contrast material and is indicated on a CT scan by an area of high attenuation, with values ranging from 85 to 350 Hounsfield units (HU) (Figure 1c) (18). The site of contrast extravasations noted on CT scans corresponds to the site of bleeding seen on angiography (19). Splenic injury The spleen is the most frequently injured abdominal organ during blunt abdominal trauma and accounts for up to 45% of all visceral injuries (20). A CT scan following the power injection of intravenous contrast is highly accurate (98%) in diagnosing acute splenic injuries (21). CT scans can detect a variety of splenic injuries, including laceration, a non-perfused region, intra-parenchymal haematoma and subcapsular haematoma (22) (Figures 2a, 2b and 2c). Several CT grading scales for splenic injury are available, but these grading scales have become less clinically important with the increasing popularity of non-surgical management of splenic injury (23–24). These scales are now most important for research and database use. Liver injury The liver is the second most frequently injured intra-abdominal viscus (2). The worldwide incidence of liver injuries is not known (9), although penetrating injuries (gunshots and stab wounds) account for the majority of liver injuries in North America and South Africa while blunt injuries cause the majority of liver injuries in Europe and Australasia (8). Although elevated transaminase levels are 100% sensitive and 92.3% specific in predicting hepatic injuries (25), CT is currently the diagnostic modality of choice. CT scans can be used to accurately diagnose parenchymal injuries and exclude surgical lesions such as bowel or pancreatic injuries (26) (Figures 3a and 3b). CT grading criteria have been proposed for liver injuries, but, as with splenic injury, these criteria do no correlate well with the need for surgical intervention or risk of subsequent complications. Surgical analyses have shown that up to 80% of liver injuries in adults and up to 97% of liver injuries in children can be treated without surgery (27). Urinary tract injury Renal injury occurs in about 10% of cases of abdominal injury and the majority of renal injuries (80% to 90%) result from blunt trauma (28). CT can provide a precise delineation of renal laceration, haematoma and perinephric collection (29); in addition, CT scans can be used to differentiate trivial injuries from those requiring intervention (28) (Figures 4a, 4b and 4c). To evaluate bladder injuries, CT cystography with retrograde bladder filling can be added to the routine CT abdominal examination (30). Bladder injuries have characteristic CT cystographic features that can be used to accurately classify injuries and plan treatment (Figures 5a, 5b and 5c). CT differentiates between extraperitoneal and intraperitoneal bladder ruptures and helps determine the management of these injuries. Pancreatic injury Pancreatic injury is encountered in only 3% to 12% of all abdominal injuries (31). Pancreatic injury is more common in children and young adults, possibly because these individuals have less retroperitoneal fat to act as a protective buffer (2). The identification of blunt pancreatic injury may be difficult because image findings are often subtle (32). Initial CT findings may be normal, even with pancreatic transaction, because the elastic pancreatic parenchyma resumes its normal contour (33). A repeated CT abdominal scan at 24 to 48 hours can help reveal evolving injuries (2). A delay in diagnosis can often result in recurrent pancreatitis, pseudocyst, fistula or abscess formation (27) (Figure 6). Bowel and mesenteric injury The sensitivity of CT to traumatic bowel injury varies from 69% to 92% and CT is 94%–100% specific for the diagnosis of bowel and mesenteric injuries (10, 34–35). CT findings can include focal bowel wall thickening, mesenteric infiltration, free air, the presence of intraperitoneal fluid without solid organ injuries and extravasated contrast material (10,11,34,36) (Figures 7a and 7b). CT images must be carefully examined to detect injuries and close attention should be paid to scanning techniques and optimal bowel contrast (37). Injury to the retroperitoneum, spine, abdominal wall and lower chest Before the use of CT, haemorrhage into the retroperitoneal space was difficult to diagnose (1). CT is valuable in the detection of retroperitoneal and abdominal wall injuries (38) (Figures 8a and 8b). In addition, CT scans can reveal various fractures involving the pelvis (Figures 9a and 9b) and spine (Figure 10) and can offer information about significant unsuspected or underestimated thoracic injuries (Figures 11a and 11b) that are common in patients with blunt abdominal trauma (3,39). Conclusion The examination of CT scans is extremely useful for the evaluation of blunt abdominal injuries in haemodynamically-stable patients. CT scans can reveal a wide variety of injuries. In addition, CT examination is fast and widely available. With appropriate scanning protocol, CT can provide good resolution images with MPR. Acknowledgements We would like to thank the surgical and radiological staff of HTAA and Kulliyyah of Medicine, IIUM for their continuous effort and assistance in the care and treatment of patients. The data obtained in this pictorial essay is part of a project funded by the IIUM Research Endowment Fund (Type A). Authors’ contributions RH and AAA had contributed equally towards drafting and revising the manuscript. References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10018f5a.jpg] [mj10018f8a.jpg] [mj10018f1b.jpg] [mj10018f4a.jpg] [mj10018f3b.jpg] [mj10018f1c.jpg] [mj10018f9a.jpg] [mj10018f11a.jpg] [mj10018f3a.jpg] [mj10018f4c.jpg] [mj10018f9b.jpg] [mj10018f8b.jpg] [mj10018f4b.jpg] [mj10018f7b.jpg] [mj10018f1a.jpg] [mj10018f2b.jpg] [mj10018f2a.jpg] [mj10018f2c.jpg] [mj10018f5c.jpg] [mj10018f7a.jpg] [mj10018f5b.jpg] [mj10018f6.jpg] [mj10018f10.jpg] [mj10018f11b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}