 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
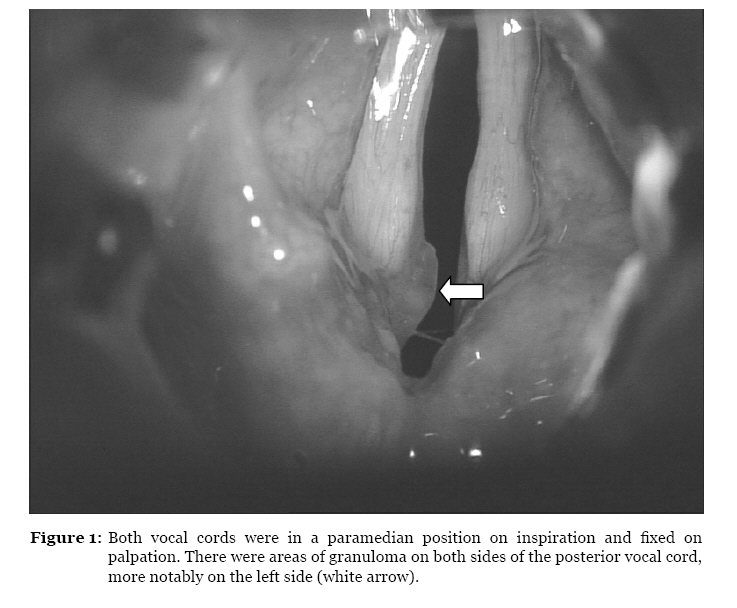
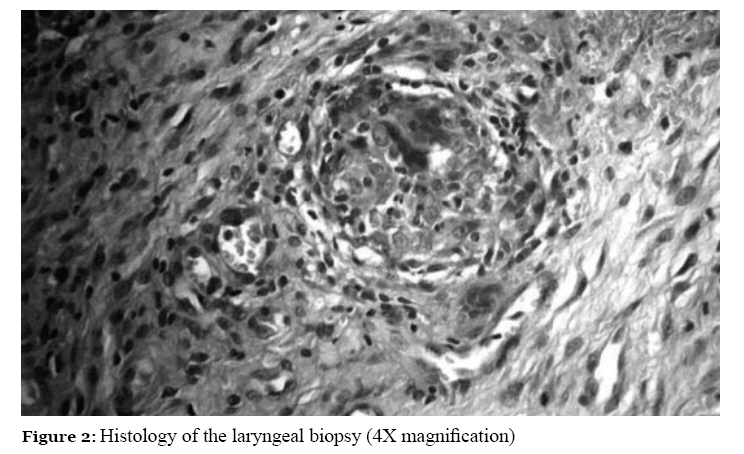
Malaysian Journal of Medical Sciences, Vol. 17, No. 2, 2010, pp. 56-60 Case report Bilateral vocal cord palsy as the sole presentation of acquired syphilis Zamzil Amin ASHA’ARI, Mohd Sayuti RAZALI, Raja Ahmad RL AHMAD Department of Otolaryngology–Head and Neck Surgery, International Islamic University Malaysia, Jalan Hospital, 26100 Kuantan, Pahang, Malaysia Correspondence: Dr Zamzil Amin Asha’ari, MBBCh (Dublin), MMed (ORL–HNS) (USM), Department of Otolaryngology–Head & Neck Surgery, International Islamic University Malaysia, Jalan Hospital, 26100 Kuantan, Pahang, Malaysia Tel: +6019-956 4996 Fax: +609-513 3615 E-mail: zamzilamin@yahoo.com Submitted: 8 Nov 2009 Abstract Bilateral vocal cord palsy is almost always caused by neck surgery, particularly surgery of the thyroid. We report a case of bilateral vocal cord palsy requiring emergency surgery to relieve the airway obstruction as the sole presentation of acquired syphilis. As the incidence of syphilis worldwide is rising, this unusual presentation may give clinicians a different perspective on the disease. Keywords: bilateral vocal cord palsy, syphilis, medical sciences Introduction Syphilis is a rare cause of vocal cord palsy. Syphilis manifestation is usually multisystemic, and a sole presentation of syphilis in the larynx is very rare. However, with the growing incidence of syphilis throughout the world, we may be facing more unusual presentations of syphilis. Syphilis is often said to be a great imitator, and Sir William Osler was quoted as saying “He who knows syphilis knows medicine”. Case report A 45-year-old Malay lady presented with noisy breathing for the past year. The condition was progressively worsening, and at the time of presentation, she had marked stridor that could be heard from the edge of her bed. Her general practitioner had previously diagnosed her with asthma and given her inhalers, but her symptoms did not improve. Over the past month, her voice had become huskier and easily fatigued. She denied any symptoms of aspiration, dysphagia, neck swelling, weight loss, headache or other central neurological symptoms. She did not have any previous neck surgery. Her first husband died ten years ago from pulmonary tuberculosis, and she had since remarried. Her current husband practices polygamy, and she is the second wife of three. They live in a small town bordering Thailand. She had loud biphasic stridor at rest and was unable to count from one to ten in a single breath. Her stridor was more marked in the supine position, and she quickly became dyspneic when lying flat. A lung examination revealed no abnormality. Indirect laryngoscopy followed by 70o laryngoscopy showed that both vocal cords were immobilised in a paramedian position, with very little airway patency. Due to the pending airway obstruction, we proceeded with emergency tracheostomy under local anaesthesia. After securing the airway, we performed a microscopic laryngeal inspection and palpation under general anaesthesia, which revealed bilateral fixed vocal cords in a paramedian position that did not move on palpation. There were areas of granuloma on both sides of posterior vocal cord, more notably on the left side (Figure 1). A biopsy was taken from the vocal cord lesion, and the histology showed the presence of foreign body-type giant cell granulomatous laryngitis (Figure 2). This raised the possibility of several differential diagnoses, with tuberculosis high on the list, given the history of previous contact. However, both Ziehl-Neelsen (ZN) and TB fluorescent stains and the specimen culture were negative. Blood investigations later confirmed the presence of Treponema pallidum antibody in the serum and a positive VDRL (Venereal Disease Research Laboratory) test with a titre of 1:128. Other investigations, including sputum for acid fast bacilli (AFB) and rapid HIV ELISA test, were negative. Computerised tomography of the brain to chest revealed no abnormal findings. A cerebrospinal fluid (CSF) analysis for neurosyphilis was not performed, as the patient did not permit it. Laser posterior cordectomy of the left vocal cord was performed after the airway was secured with a tracheostomy. This procedure was performed because the larynx was in a severely fixed position and the patient had earlier expressed the desire to avoid a long-term tracheostomy. The patient was also started on intramuscular procaine penicillin, 2.4 million units daily for 14 days. Following the diagnosis of acquired syphilis, we performed a thorough physical examination to look for other syphilis manifestations; none was found. The patient’s husband was screened and also found to be infected with syphilis. The patient was given a post-operative course of steroids, and tracheostomy decannulation was completed four days post-operation. She was discharged five days post-operatively. Her stridor disappeared after six weeks, although vocal huskiness was still noted. She completed the 14-day course of antibiotics, and a follow-up VDRL test nine months later was seronegative. The final diagnosis was bilateral vocal cord fixation secondary to a tertiary gummatous laryngeal syphilis. Discussion Syphilis is a sexually transmitted infection caused by the bacterium T. pallidum. In this millennium, the largest numbers of new syphilis infections have occurred in South Asia and Southeast Asia, followed by sub-Saharan Africa, and then Latin America and the Caribbean (1). However, recent data have shown that the incidence of syphilis in the Western world is also on the rise again in this new millennium, after periods of decline in the post-penicillin era of the last millennium (2,3). Thyroid or parathyroid surgery, which is often performed on both sides of the neck, can injure both recurrent laryngeal nerves and is by far the most common cause of bilateral vocal cord palsy (4). Granulomatous infections, such as tuberculosis and syphilis, can cause unilateral or bilateral palsy, but these account for less than 1% of the total causes (4). A search in PubMed and Scopus for the words “syphilis” and “larynx” yields fewer than 50 publications, and the majority of these were published in the last millennium. Syphilis usually has multisystemic manifestations, and it very rarely affects only one system. The interesting feature of this case is that the patient presented with lesions exclusively confined to the larynx. A case of syphilis exclusively presented in the larynx was described in 1917, before the antibiotic era, when the worldwide incidence of syphilis was epidemic (5). Head and neck presentation can be categorised according to the stage of infection. Chancre of the oral and nasal mucosa, nasal septum perforation, and cervical lymphadenopathy are the primary syphilis manifestations (6). Secondary syphilis may also present with mucous lesions and lymphadenopathy and with alopecia, meningitis, headache and ocular lesions (6). Tertiary syphilis can be further divided into cardiovascular syphilis, neurosyphilis and late benign stage (gumma). Neurosyphilis patients may present with headache, vertigo, dementia, delusions, confusions, and cranial nerve palsies (7). Gummatous lesions are monocytic infiltrates with tissue destruction in any organ. In this case, the vocal cord palsy was most likely due to the gummatous lesions on the vocal cords, which fixed both sides in the paramedian plane. However, as we did not do the CSF culture, we could not rule out the concurrent possibility of neurosyphilis causing bilateral recurrent laryngeal nerve paralysis. Performing routine investigations for granulomatous infections may not be cost-effective in all cases of vocal cord palsy. However, clinicians should remember to do them when the patient’s history and clinical examinations indicate their necessity. Medical history interviews should always include questions about contact with people with tuberculosis, syphilis or other granulomatous diseases and include a thorough sexual contact history. Blood examinations for syphilis should be done in all cases without an obvious cause of palsy, in those patients with a history of recent travelling to the endemic countries, in patients with low immunity status, abnormal sexual behaviour or sexual promiscuity and in patients with multiple sexual partners. In our case, we ordered tests to rule out tuberculosis, as it was initially the suspected diagnosis given that the patient’s first husband had the disease. These tests included sputum for AFB and ZN and fluorescent stain microscopy on the laryngeal specimens. However, all these tests were negative. Medical management consisted of a course of penicillin, with the duration of therapy dependent on the severity and stage of the disease. Because neurosyphilis was not ruled out, we followed the Center for Disease Control, USA (CDC) recommendation for neurosyphilis treatment in this patient. Medical management to improve the airway may delay or prevent surgical intervention, and in many centres, a wait-and-see period of six months to a year is usually practiced if the patient is not in respiratory distress (8). In our case, however, the patient presented with acute airway obstruction, and medical therapy alone could not provide relief. Hence, a tracheostomy was performed to secure the obstructed airway. After we secured the airway with tracheostomy, we needed to choose the best treatment for the underlying cause of the vocal cord palsy. Because the cause in this case was syphilitic infection, the best treatment had to be an antibiotic. A wait-and-see period of three to six months in this kind of case is advocated by many centres to determine how the patient responds to the treatment (8). Surgical repair of the vocal cord can be avoided in most cases if the mechanical obstruction is cleared with antibiotics. In our patient, however, we opted to perform an immediate surgical intervention because the vocal cord damage caused by the disease was so severe that we did not think antibiotics would totally resolve it. More importantly, our patient wished to avoid long-term tracheostomy, so we decided that a cordectomy was the best choice. Vocal cord surgery options include lateralisation procedures, such as posterior cordectomy, arytenoidectomy or arytenoidopexy. Dennis and Kashima first introduced a posterior partial cordectomy procedure using a carbon dioxide laser (9). This involves excising a C-shaped wedge from the posterior edge of one vocal cord to open up the airway. If this posterior opening is not adequate after six to eight weeks, the procedure can be repeated, or the same procedure can be performed on the other vocal cord. All of their patients achieved a functional airway and preserved voice quality without a tracheostomy, the same outcome that our patient experienced. Conclusion Laryngeal involvement is a rare manifestation of syphilis. However, this case shows that acquired syphilis may present solely in the larynx. As the incidence of syphilis worldwide is increasing again in this millennium, clinicians must be aware of uncommon presentations to ensure an accurate diagnosis. Acknowledgements We would like to thank the director of Hospital Tengku Ampuan Afzan, Kuantan, Pahang, Malaysia and the director general of health, Ministry of Health Malaysia, for permission to report this case. Written informed consent was obtained from the patient for the publication of this case report and the accompanying images. Authors' contributions ZAA was responsible for the overall management of this case and for preparing the manuscript. MSR performed the posterior cordectomy under the supervision of senior surgeon RARLA. All authors contributed to writing this case and have read and approved the final manuscript. References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10022f1.jpg] [mj10022f2.jpg] |
| |||||||||

{kind=link}
{kind=link}